PECARN Rules: Reducing CT Scans in Pediatric Head Trauma
advertisement

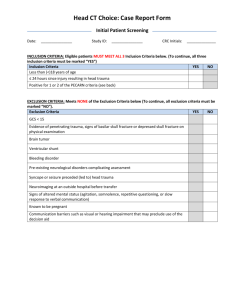
Applying the PECARN Prediction Rules to Reduce Unnecessary CT Scans in Children after Minor Head Trauma A collaborative effort of California ACEP and the Choosing Wisely Campaign Background - Between 1995 and 2005, CT use in children more than doubled - 20 - 60% of children assessed for head trauma in North American emergency departments undergo CT—major variability in practice from one ED to the next - Less than 10% of CT scans in children with minor head trauma (defined by GCS score of 14-15) show traumatic brain injury (TBI) - Injuries needing neurosurgery are very uncommon in children with GCS 14–15—only 0.1 – 0.2% Migliorett et al. JAMA Pediatr. 2013. Mannix et al. J Pediatr 2012. Palchak et al. Ann Emerg Med 2003. Background • Ionizing radiation from CT scans can cause lethal malignancies • Risk estimated at 1/1000-1/5000 • Risk increases as age decreases Brenner DJ. N Engl J Med 2007. Pearce MS. Lancet 2012. ACEP and Choosing Wisely A multi-year effort of the ABIM Foundation Mission: promote conversations among physicians and patients about using appropriate tests and treatments and avoiding care when harm may outweigh benefits. Since launching in April 2012, over 80 specialty societies and consumer groups have become “Choosing Wisely” partners. ACEP officially joined in February 2013. ACEP’s Oct 2013 recommendations were developed through a multistep process that included research and input from an expert panel of emergency physicians and the ACEP Board of Directors. PECARN Head Injury Prediction Rules - Large, diverse, prospective study of 42,000 children with minor head trauma (defined as GCS 14-15) - Validated prediction rules to identify children at very low risk of TBI after head trauma for whom CT is unnecessary - Prediction rule accuracy for low-risk group in validation sample (>50% of patients, accounting for ~ 25% of CTs): <2yo: NPV 100%, Sensitivity 100% >2yo: NPV 99.95%, Sensitivity 96.8% Kuppermann et al; Lancet 2009. Original published PECARN rules for < 2 years (A) and >= 2 years (B) PECARN Head Injury Prediction Rules How to use the rules for children < 2 y.o. High Risk of TBI (4.4%): GCS =14, palpable skull fracture, or altered mental status (AMS) → CT indicated Intermediate Risk (0.9%): occipital or parietal scalp hematoma, LOC > 5 seconds, severe mechanism of injury, or acting different per parent → Observation vs CT, shared decision-making Low Risk of TBI (<0.02%): none of the PECARN predictors → Observe in ED; CT not recommended PECARN Head Injury Prediction Rules How to use the rules for children >= 2 y.o. High Risk of TBI (4.3%): GCS =14, signs of basilar skull fracture, or AMS → CT indicated Intermediate Risk (0.8%): LOC, history of vomiting, severe HA, or severe mechanism of injury → Observation vs CT, shared decision-making Low Risk of TBI (<0.05%): none of the PECARN predictors → Observe in ED; CT not recommended Altered Mental Status (AMS) “AMS” is a proxy for “GCS 14” - agitation - somnolence - repetitive questioning - slow response to verbal communication Severe Mechanism of Injury - motor vehicle crash with patient ejection - death of another passenger - rollover MVC - pedestrian or bicyclist without helmet struck by motor vehicle - fall >5 ft(if >2 y.o.) or > 3 ft(if < 2 y.o.) - head struck by high-impact object (golf ball, baseball, golf club, horse hoof, etc.) What if this were YOUR kid, Doc? • If clearly high risk: CT • If clearly low risk: Observation • If intermediate risk: Shared DecisionMaking - Providing information on benefits and risks - Evaluating options based on goals and concerns - Providing appropriate disposition and follow-up Shared Decision Making is based on: • Physician experience • Parental preference • Multiple vs. isolated findings • Age < 3 months Worsening signs or symptoms after initial period of observation is an indication for CT scan Cal ACEP/ Choosing Wisely Collaboration Pediatric Head Trauma CT Decision Guide Children younger than 2 years GCS < 15 Palpable skull fracture AMS (agitation, somnolence, slow response, repetitive questioning) Pocket card High Risk--4.4% risk of ci-TBI* Yes to any CT No Scalp hematoma (excluding frontal) LOC >5 seconds Not acting normally per parent Severe mechanism of injury -Fall >3 ft -MVA w/ ejection, rollover, or fatality -Bike/ped vs. vehicle w/o helmet -Struck by high-impact object No Intermediate Risk--0.9% Yes to any Observation vs. CT using shared decision-making Low risk-- < 0.02% CT not indicated, Observe *ci-TBI: risk of clinically important TBI needing acute intervention, based on PECARN validated prediction rules Clinical factors used to guide decision-making: - Multiple vs. isolated factors - Worsening findings during observation (AMS, headache, vomiting) - Physician experience - Parental preference - <3 months old Cal ACEP/ Choosing Wisely Collaboration Pediatric Head Trauma CT Decision Guide Children 2 years and older GCS < 15 Signs of basilar skull fracture AMS (agitation, somnolence, slow response, repetitive questions) Pocket card High Risk--4.3% risk of ci-TBI* Yes to any CT No Vomiting LOC Severe headache Severe mechanism of injury -Fall >5 ft -MVA w/ ejection, rollover, or fatality -Bike/ped vs. vehicle w/o helmet -struck by high-impact object No Intermediate Risk--0.8% Yes to any Observation vs. CT using shared decision-making Low risk-- < 0.05% CT not indicated, Observe *ci-TBI: risk of clinically important TBI needing acute intervention, based on PECARN validated prediction rules Clinical factors used to guide decision-making: - Multiple vs. isolated factors - Worsening findings during observation (AMS, headache, vomiting) - Physician experience - Parental preference Explaining the Rationale Low risk = Concussion - Concussion is a clinical dx based on symptoms - Risks of CT outweigh benefits Intermediate risk - Intermediate risk symptoms warrant observation before deciding whether to do head CT - No increase in adverse outcome with this strategy Information for parents: sample page from parent pamphlet “What is a head CT?” “A CT (computed tomography) machine is a large scanner that uses radiation to take detailed pictures of your brain, eyes, nose, ear, and bones. The process usually takes 30-60 minutes, and may require your child to be sedated. CT images help doctors decide if a child needs surgery after a severe injury. For a minor head injury, or a concussion, CT scans usually do not provide any information that would change your child’s treatment, and could even be harmful for your child because of the radiation.” Weighing the risk in “intermediate” patients Give more consideration to CT scan if: - Child is < 3 months of age - Home observation is unreliable - Child has more than one “intermediate” risk factor, for example: • vomiting AND headache • headache AND LOC • high-risk mechanism AND parietal hematoma Weighing the risk factors - If patient has worsening signs and symptoms during observationget CT - Experts recommend observation period of: - ~2 hours post-injury in low-risk patients ~4 hours post-injury in intermediate-risk patients - Some of observation period can happen at home if there is a reliable observer Dispelling the Myths Myth: Delaying head CT leads to poorer outcomes Fact: Observation in the ED for ~4 hours in intermediate risk groups before making a decision about CT yields equivalent outcomes to doing immediate CT Fact: Risk of CT-induced malignancy in low risk group outweighs benefits of imaging Nigrovic et al. Pediatrics; 2011. Brenner DJ et al. N Engl J Med 2007. Dispelling the Myths Myth: Head CT is faster and easier than observation Fact: CT can take just as much or more time to obtain and read, especially if sedation is necessary Dispelling the Myths Myth: Not recommending CT can result in lower patient satisfaction scores and places provider at risk of litigation in event of poor outcome Fact: Explaining the research, including parents in the decision-making process, and asking about parent preference improves satisfaction Geijerstam et al. BMJ 2006. Case 1 A 20 month old girl falls down a flight of stairs and presents with 3 large, 3x3 cm, boggy hematomas, one on each side of the forehead, and one on the right parietal scalp. She had no loss of consciousness, no vomiting, and now 30 minutes after the event is playing, talking to her mom, and acting normal. There are no other clinical signs of skull fracture, and she has normal vital signs and an otherwise normal physical exam. Case 1 - < 2 years old + non-frontal scalp hematoma + severe mechanism of injury (fall > 3 ft) no LOC, acting normally Intermediate Risk (0.9%)- (criteria are: non-frontal scalp hematoma, LOC > 5 sec , severe mechanism of injury, not acting normally per parent) → Obs v CT PECARN Head Injury Prediction Rules Application -MDCalc.com algorithm Case 1 - Parents okay with observation after discussion with MD - Child did well - No sequelae on 24 hour phone follow-up Case 2 A 9 year old boy falls off his bike and strikes his head (unhelmeted) and sustains a large, boggy frontal scalp hematoma. He had no loss of consciousness, a moderate headache, no vomiting, and is mentating normally with an otherwise normal physical exam. Case 2 - > 2 years old Unhelmeted, but not hit by car fall < 5 ft. frontal scalp hematoma but no sign of fracture No LOC, mentating normally, moderate headache, no vomiting Low Risk of TBI (0.05%)- no severe HA, N/V, or LOC → Obs Case 2 MD Calc: Case 2 After one hour of observation, he started to experience a severe headache and vomited twice. Intermediate Risk: multiple, worsening findings CT performed → epidural hematoma → OR Harry’s CT scan Harry post-op, doing well Case 2 PECARN and other studies provide good evidence that delayed diagnosis of clinically significant TBI results in the same outcomes as doing CT immediately—no increase in deaths or disability Geijerstam et al, BMJ 2006 Kuppermann N et al, Lancet 2009 Case 3 - 3 month old baby accidentally dropped by mom - Mom “can’t remember” if he had LOC, or if he cried right away - Vomited once in the ambulance; now acting completely normal - Smiling, no signs of trauma on exam Case 3 < - 2 years old No scalp hematoma + severe mechanism of injury (fall > 3 ft) Unclear LOC, now acting normally Intermediate Risk (0.9%)- (criteria are: non-frontal scalp hematoma, LOC > 5 sec , severe mechanism of injury, not acting normally per parent) → Obs v CT Case 3 MD Calc: Case 3 - Mom is a teenager and is distraught; this happened in the middle of a family dispute where she was assaulted by a family member - Physician concerned that home observation may not be reliable - CT ordered Case 3 - Tiny frontal contusion Observed overnight No sequelae No other intervention Case 4 A 5 year old girl falls off a playground swing, sustaining a 2 cm occipital laceration with a boggy 3 x 3 cm hematoma. She had no LOC, no vomiting, and is acting normal per mom. She cries with exam but is otherwise normal-appearing, with no skull Case 4 > 2 years old - Fall of < 5 feet (not a high-risk mechanism) - No other high-risk features: no vomiting, no severe headache, no LOC, GCS 15, no sign of basilar skull fracture Low-risk (0.05%) Observation recommended Case 4 MD Calc: Case 4 Child was observed for 2 hours and did well Laceration repaired No sequelae at 24 hour phone follow-up Case 5 A 12 year old boy goes down during an aggressive soccer play, hitting his head on the ground and sustaining a 1 – 2 second loss of consciousness. He has no vomiting but complains of severe headache and nausea. He has an occipital hematoma but no signs of basilar skull fracture. GCS is 15. Case 5 - > 2 yrs of age + Severe headache + Brief loss of consciousness GCS 15, no basilar skull fracture No vomiting Intermediate risk (0.9%) – (criteria are: GCS 15, no basilar skull fracture, no LOC, no vomiting, no severe headache, no severe mechanism) Obs vs. CT Case 5 MD Calc: Case 5 - Given acetaminophen and ondansetron - Observed in the ED for 3 hours (4 hours post-injury) - Gradually improved; parents felt comfortable not getting CT - Doing well at 24 hour phone follow-up Future Application Potentials - QI process - Evaluation of impact on physician practice state-wide - Outcome measures - Grants Resources PECARN predicton rule: http://www.pecarn.org/currentresearch/documents/Kuppermann_2009_ The-Lancet.pdf PECARN prediction rule dataset: http://www.pecarn.org/studyDatasets/TBIPredictionRule.html Choosing Wisely communication modules: http://modules.choosingwisely.org/modules/m_00/default_FrameSet.htm Selected references Miglioretti DL, Johnson E et al. The use of computed tomography in pediatrics and the associated radiation exposure and estimated cancer risk. JAMA Pediatr. 2013;167:700-707. Mannix R, Meehan WP et al. Computed tomography for minor head injury: variation and trends in major United State pediatric emergency departments. J Pediatr. 2012;160:136-139. Palchak MJ, Holmes JF, Vance CW, et al. A decision rule for identifying children at low risk for brain injuries after blunt head trauma. Ann Emerg Med 2003; 42: 493–506. Kuppermann N, Holmes JF et al. Identification of children at very low risk of clinically important brain injuries after head trauma: a prospective cohort study. Lancet 2009; 374:1160-70. Pearce MS, Salotti JA et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort sutdy. Lancet 2012;380:499-505. Nigrovic et al. The Effect of Observation on Cranial Computed Tomography Utilization for Children After Blunt Head Trauma. Pediatrics 2011;127:1067-1073. Brenner DJ, Hall EJ. Computed tomography—An increasing source of radiation exposure. N Engl J Med 2007; 357: 2277–84 Geijerstam et al. Medical outcome after immediate computed tomography or admission for observation in patients with mild head injury: randomised controlled trial. BMJ 2006;333:465 Schonfeld D, Fitz BM, Nigrovic LE. Effect of the duration of emergency department observation on computed tomography use in children with minor blunt head trauma. Ann Emerg Med 2013;62:597.