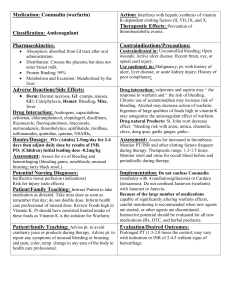
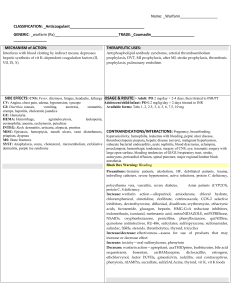
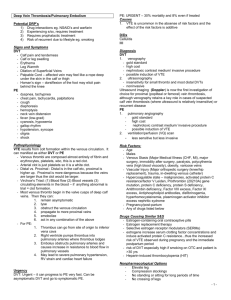
1. Describe the background of Anticoagulation Coagulation is the formation of a blood clot and involves platelet and clotting cascade activation Numerous factors such as blood vessel injury, blood stasis (blood flow slows or stops) and prothrombic conditions activate the coagulation process. Blood clots form in the brain, heart, lungs and legs. An activated clotting factor activates the next clotting factor in sequence until fibrin forms and cross links to hold clot together Activation pathway (Intrinsic) and Tissue factor pathway (extrinsic) lead to fibrin formation 2. Discuss the indications for anticoagulants Prevention of Cardioembolic stroke in Atrial fibrillation pts. o Valvular or mitral stenosis: Warfarin is preferred. o Non-valvular: DOACS are preferred. Prevention/treatment of VTE o Acutely ill or After knee/hip replacement o DOACS preferred, except in antiphospholid syndrome or mechanical heart valve. o UFH, LMWH, Fondaparinux (off label for HIT) Immediate treatment of ACS o Parenteral anticoagulants Reduction in the risk of major CVD events in CAD/PAD: Xarelto 3. Why is anticoagulation a high alert medication? Causes significant bleeding per ISMP Joint Commission require policies and protocols to initiate and mgmt therapy Defined process includes standardized ordering, dispensing, administration, monitoring and pt/caregiver education to improve outcomes and decrease cost. Common visible bleeding or acute Hgh drop > 2g/dL signify that bleeding occurred. o Epistaxis: nose bleeds o Gums: from gingivitis o Bruising o Hematoma: bad bruise o Hematemesis: blood in vomit from GI bleeding o Hematuria: blood in urine o Blood in the anus 4. What other drugs increase bleeding risk? o o o Other anticoagulants, antiplatelets, and fibrinolytics Herbal supplements o (5 G’s), chamomile, chondroitin, dong quai o High doses of Vitamin E and willow bark NSAIDs, SSRI’s and SNRIs 5. List other drugs that can increase blood clotting risk? o SERMS, Estrogen, and Aromatase inhibitors. 6. What supplements decrease the effectiveness of Warfarin? o Green tea, coenzyme Q10 and St. John’s Wort and possibly ginseng 7. Compare doses of anticoagulants o o Anticoagulants prevent blood clot formation and keep existing clots from becoming larger. o Parenteral Anticoagulants Heparins (Unfractionated heparin and LMWHs) UF VTE: 5000 units SQ Q8-12 hrs for ppx, 80 units/kg bolus, 18 units/kg/hr infusion UF ACS: 60 units/kg IV bolus than 12 units/kg/hr Enoxaparin ( Lovenox) o VTE ppx: 30 mg SUBQ Q12 hrs or 40 mg SC daily o VTE or NSTEMI treatment: 1 mg/kg SUBQ Q12 h or 1.5 mg/kg SC QD (inpt VTE tx) o STEMI treatment <75 y/o: 30 mg IV bolus plus 1mg/kg SQ o STEMI treatment > 75 y/o: No bolus, CrCl <30: 1 mg/kg SC daily Dalteparin (Fragmin): Doesn’t treat STEMI Direct Thrombin Inhibitors o Argatroban :Decrease dose in Hepatic impairment. Indicated for HIT and pts at risk of HIT undergoing PCI o Bivalirudin (Angiomax): Decease dose if crcl <30. Pts with ACS undergoing PCI including HIT Factor Xa Inhibitors o Fondaparinux (Arixtra): SC injection for VTE treatment/ppx. Caution in crcl 30-50 mL/min or crcl < 30 mL/min Oral Anticoagulants o What is one purported advantage of DOACs over VKAs? o Few drug- food interactions, shorter DOA, less comparable bleeding Vitamin K Antagonist (Warfarin) o (Jantoven or Coumadin) o Healthy outpatient: ≤ 10 mg daily for first 2 days than adjust dose per INR o Lower doses (≤ 5 mg) for certain conditions Elderly, malnourished, drugs that Inc its INR, liver disease, HF, or high risk of bleeding INC INR: Metronidazole, Azoles, Amiodarone dec by 30-50%, TMP/SMX Dec INR: CYP2C9 inducers and foods high in Vitamin K (greens, broccoli, Brussel sprouts, collard greens and kale) o Warfarin colors: pink, Lavendar, green, tan, blue, peach, teal, yellow, white o 1 mg, 2, 2.5, 3, 4, 5, 6, 7.5, 10 Direct Thrombin Inhibitors (Dabigatran) o Pradaxa: o Stroke ppx: 150 mg BID, reduce to 75 mg BID if crcl is btw 15-30. o VTE treatment: 150 mg BID, start after 5-10 days of parenteral anticoagulation. Xa Inhibitors o Apixaban: (Eliquis) VTE TX: Initial 10 mg PO BID for 7 days, then 5 mg PO BID o Rivaroxaban (Xarelto): VTE tx: Initial 15 mg PO BID x 21 days than 20 mg QD with food. Avoid if crcl < 30 o Edoxaban (Savaysa): Don't use if Crcl > 90. VTE tx: Start after 5-10 days of parenteral anticoagulation. Stroke Prophylaxis in A. Fib 8. Compare the mechanism of action of parenteral and oral anticoagulants Warfarin: competitively inhibits the C1 subunit of the multi-unit vitamin K epoxide reductase (VKORC1) enzyme complex. o Reducing the regeneration of vitamin K epoxide and causes depletion of active clotting factors 2,7,9 and 10 and protein C & S Heparins: Indirectly inhibit thrombin (factor 2a) and factor 10a by binding to Antithrombin (AT). Fondaparinux: Binds to AT to increase AT activity (inactivate thrombin and factor xa) DTIs: Directly block thrombin, decreasing the amt of fibrin for clot formation 9. Describe UFH uses, advantages and disadvantages. 10. Uses: Continuous IV infusions for ACS tx and VTE tx/ppx bc of fast onset and shorth half-life. Advantages: safer in renal impairment and has an antidote (Protamine) Disadvantages: Heparin Induced Thrombocytopenia (HIT), unpredictable anticoagulation response and requires monitoring List the contraindication, warning, side effects and monitoring of UFH. Contraindications: uc active bleed, severe thrombocytopenia or history of HIT. Warning: Fatal medication errors: verify correct concentration o Heparin lock-flushes (HepFlush) only keeps IV lines open o Fatal errors, esp in neonates, occur if incorrect concentration is chosen. o Heparin injection and flushes look and sound alike Side effects: bleeding (every type), thrombocytopenia, HIT, hyperkalemia. Monitoring: baseline plt,hgb, hct (> 50% plt dec suggest HIT), aPTT or anti- xa levels after 6 hours and every 6 hours until therapeutic. Q24 hrs with dose changes. aPTT therapeutic range is 1.5-2.5 x control 11. How is the mechanism of action of LMWH different from UFH? 12. Accelerates AT activity and has much greater anti-factor Xa activity than IIa. How is the LMWH BBW, CI, SE and monitoring different from UFH? Advantage: More predictable anticoagulation response, Protamine antidote o Doesn't require anti-xa levels except for in pregnancy o Obtain peak anti xa levels 4 hours after SC dose BBW: Risk of hematomas and subsequent paralysis for pts receiving neuraxial anesthesia (epidural, spinal) or spinal puncture. CI: History of HIT or active bleed SE: bleeding, anemia, inj site rxns (e.g. pain, bruising, hematomas), decreased plts (thrombocytopenia, HIT) Monitoring: Platelets, Hgb, Hct, SCr o Useful in renal insufficiency, obesity, low body weight How is LMWH stored? Room temperature What causes patient to lose some drug? Expelling air bubble from springe 13. How to assess the probability of HIT? Calculate the 4Ts score Thrombocytopenia: unexplained >50% decrease in plts from baseline Timing: onset occurs 5-10 days after initiation Thrombosis: can be new suspected or confirmed thrombosis or skin lesions Other causes: inability to identify other probable causes of HIT 14. How to treat HIT? Stop all forms of heparin or LMWH including heparin flushes or catheters If already on Warfarin and has HIT, D/C warfarin and give Vitamin K o Restart at lower doses (5 mg max) when plt count is > 150 cells/mm^3 o Bridge with another anticoagulant for min of 5 days until INR is in target range consecutively Immediate treatment: Rapid-acting non-heparin anticoagulants (e.g. Argatroban) Bivalirudin is preferred anticoagulant for urgent cardiac surgery or PCI 15. Why does Warfarin have to be bridged? Delayed onset of action 16. What is HIT? An immune – mediated IgG drug reaction that has high risk of venous and arterial thrombosis. Immune system forms antibodies that bind with heparin and platelet factor 4 (PF4) to form a complex The complex binds to the Fc receptors on platelets to cause platelet activation. This prothrombic state and if left untreated can cause many complications o HITT leading to amputations, post-thrombotic syndrome, and/or death 17. List Oral Direct Factor Xa Inhibitors BBW, CI, Warning, SE, and monitoring BBW: Same as LMWH, Edoxaban (reduced efficacy in CrCl >90 ml/min) CI: Active pathological bleeding Warnings: not recommended w/prosthetic heart valves or antiphospholipid syndrome Side effects: well tolerated, unless bleeding occurs Monitoring: Hgh, Hct, Scr, LFTs, no monitoring of efficacy required. 18. List Oral Direct Factor Xa Inhibitors Counseling and clinical pearls All can be crushed in apple sauce or in water for NG tube Apixaban (Eliquis): crushed into apple juice, D5W and apple juice Discontinue 24 hours before elective surgery or low bleeding risk for Eliquis Discontinue 48 hours before elective surgery if Eliquis pt at moderate- high risk of bleeding. Antidote Andexanet alfa (Andexxa) for Eliquis and Xarelto Take missed dose immediately on same day, don't double dose o Rivaroxaban (Xarelto): Take once daily medication immediately and take BID medication all at once Xarelto doses > 15 mg require an evening meal 19. List Fondaparinux BBW, CI, SE, Monitoring and Antidote Given SC BBW: Same as LMWH CI: Severe renal impairment (CrCl < 30 ml/min) and active major bleed SE: bleeding (all types), anemia, local injection site rxns (rash, pruritus, bruising) and thrombocytopenia. Monitoring: Anti-Xa levels (3 hours post- dose), platelets, hgb, hct , SCr No Antidote 20. Why are there factor Xa drugs interactions? Other drugs increase bleeding risk Rivaroxaban (Xarelto): CYP3A4 and P-gp substrate o Avoid dual inducers or decrease dose by 50% with strong dual inhibitors. Apixaban (Eliquis): CYP3A4 and P-gp substrate o Avoid dual inducers or inhibitors 21. How to switch between oral anticoagulants and warfarin? From Warfarin: INR lowers (READ, <3, <2.5, <2, <2) To Warfarin: Oral Xa: stop it and start parenteral anticoagulant + warfarin at next dose. To Warfarin: Start warfarin 1-3 days before stopping Dabigatran. 22. What is BBW, CI, Warning, SE, Monitoring and notes of Dabigatran? BBW: same as LMWH and Xa inhibitors CI: active pathological bleeding and mechanical prosthetic heart valves SE: dyspepsia (indigestion), gastritis- like symptoms, bleeding (including GI bleeding) Monitoring: Hgb, Hct, Scr, no monitoring of efficacy required Antidote: Idarucizumab( Praxbind) Keep capsules in original container and discard in 4 months to protect from moisture. Swallow capsule whole and don't administer by NG tube: took quick rapid anticoagulation 23. What is the CI, Warning, SE and Monitoring of Injectable DTI? CI: active major bleeding Side effects; bleeding (mild- severe), anemia Monitoring: aPTT, activating clotting time, plts, hgb, hct, renal function Argatroban: increases INR, dose cautiously and avoid LD of warfarin Safe with active HIT or history of HIT: no cross reaction with HIT antibodies NO ANTIDOTE 24. What is BBW, CI, Warning, SE and Monitoring of Warfarin? BBW: Major or fatal bleeding CI: Pregnancy (except with mechanical heart valves) Warnings: Tissue necrosis/gangrene, HIT (CI as initial tx in HIT), presence of CYP2C9 *2 or *3 allele and/or polymorphism of VKORC1 increases bleeding risk SE: bleeding/bruising, skin necrosis, purple toe syndrome Monitoring: INR after initial 2-3 doses and every 4-12 weeks if on stable dose o Goal: for most indications: 2-3 o Goal for mechanical mitral valve: 2.5-3.5 Antidote: Vitamin K S-warfarin is more potent than R therefore drugs that interact via CYP2C9 have greater impact of Warfarin anticoagulant impact. o Minor substrate of 2C19 and 3A4. 25. What are a few key points of Warfarin? Healthy pts: Initiate doses ≤ 10 mg daily for the first 2 days than adjust based on INR Acute DVT/PE treatment: Start on the same day as parenteral anticoagulant and continue for minimum of 5 days and until the INR is ≥ 2 for 24 hours No pharmacogenomic testing, VK supplementation or bridging with single low INR, obtain another INR within 1-2 weeks if on stable dose and have one out of range INR ≤ 0.5 26. Why use reversal agents? Reverse life-threatening bleeding or pt requires surgery. Protamine MOA: binds to acidic heparin to form a stable salt complex which neutralizes anticoagulant activity of heparins 27. How does Protamine dosing differ for the heparins? UFH: 1mg of Protamine reverses about 100 units of heparin given in the last 2-2.5 hours (short half life) Maximum dose: 50 mg LMWH o Enoxaparin: 1mg per 1 mg of Lovenox given in last 8 hours 0.5 mg Protamine per 1 mg of Lovenox given > 8 hours o Dalteparin : 1 mg per 100 anti-xa levels of Dalteparin Formulation: Administer slow IV push (max rate of 50 mg over 10 minutes) 28. What are the formulations, BBW, SE and counseling points of Phytonadione? Vitamin K (Mephyton): comes as oral and IV BBW: Hypersensitivity rxns (HSR) occur rarely during or after administration SE: Anaphylaxis, flushing, rash, dizziness Requires light protection during administration Why not SC or IM route? Variable absorption and risk of hematoma o SC for slow onset 29. List other reversal agents? 4 Factor Prothrombin Complex Concentrate (Human) (Kcentra) o Administer with Vitamin K o Refrigerate and sit at room temp before use o Against Factors: 2,7,9, 10, Protein C and S 3 Factor Prothrombin Complex Concentrate (Human) (Profilnine) o Administer with Vitamin K (off label use) o Warning: Contains factor 2, 9, 10 and subtherapeutic levels of 7 Factor 7a Recombinant ( NovoSeven, Sevenfact) o Off-Label use o BBW: serious thrombotic events 30. Discuss Warfarin reversal in depth. Elevated INRs are concerning for increased risk of bleeding Vitamin K + or – other medications (K centra) Oral Vitamin K: 2.5-5 mg preferred without significant major bleeding IV Vitamin K: for serious bleeding. Infuse slowly to avoid anaphylaxis Symptoms/INR value o INR ≤ 4.5: Reduce or skip warfarin dose, monitor INR o INR 4.5-10: Hold 1-2 doses of Warfarin o INR > 10: Oral Vitamin K. Monitor INR. Resume warfarin at lower dose o Major Bleeding: Slow IV injection of Vitamin K (5-10 mg) & PCC 31. How to mgmt patients on Warfarin before operation? Stop warfarin 5 days before major surgery o Resume 12-24 hours after surgery when hemostasis is achieved. Recommend bridge therapy with LMWH or UFH for mechanical heart valve, AF or VTE pts at high risk of thromboembolism o Bridging means stopping warfarin and using LMWH or UFH doses for a short period to prevent clotting. o D/C SC LMWH 24 hours before surgery o D/C IV UFH 4-6 hours before surgery 32. How to diagnosis patient with VTE? Symptoms: pain in affected limb and unilateral lower extremity swelling DVT diagnosed by an ultrasound PE diagnosed by a pulmonary CT angiogram 33. What are risk factors for the development of VTE? Modifiable Risk Factors o Acute medical illness, Immobility o Medications SERMS, Estrogen, ESAs o Obesity (BMI >30 kg/m^2) o Pregnancy/Postpartum o Recent surgery or major trauma Non-modifiable Risk Factors o Increasing age o Cancer or chemotherapy o Previous VTE o Inherited or acquired thrombophilia Antithrombin deficiency Factor V Leiden Antiphospholipid syndrome Protein C or S deficiency o Certain disease states Heart failure, nephrotic syndrome, respiratory failure 34. What anticoagulants are approved for VTE ppx? UFH, LMWH, fondaparinux, rivaroxaban and apixaban If contraindicated, use nondrug alternatives o Intermittent pneumatic compression (IPC) devices o Graduated compression stockings (GCS) o Long-distance travelers at risk of VTE Frequent ambulation, calf muscle exercises and graduated compression stockings 35. How to determine the duration and preferred drugs in VTE tx ? Duration depends on if VTE was provoked or unprovoked o Reversible risk factor: 3-month treatment o Unprovoked risk factor: > 3-month treatment if bleeding risk is low o 2+ Unprovoked episodes: long-term treatment considered Preferred drug depends on if pts had cancer o No cancer: Dabigatran (Praxada) or Oral Xa inhibitors preferred o Cancer: Oral Xa inhibitors are preferred 36. Why use anticoagulants in Atrial fibrillation? A. Fib pts can form a clot in the heart that can travel to the brain causing a cardioembolic stroke or transient ischemic attack (TIA). Stroke prevention is an important goal in A fib pt. o Some pts undergo cardioversion to regain normal sinus rhythm o Recommended anticoagulation tx prevents atrial thrombosis and subsequent stroke due to procedure AF> 48 hrs or unknown: anticoag. For 3 wks before and 4 wks after cardioversion AF≤48 hours: start anticoag at presentation, perform cardioversion, and continue full anticoagulation for at least 4 wks. The need for chronic anticoagulation tx is based on stroke risk o Mechanical heart valve pts has the highest risk for clotting/strokes Warfarin only used o Major of pts has non-valvular AF o CHA2DS2-VAS: estimates stroke risk Score of 2 (m) or 3 (w)= anticag for ppx HAS-BLED assesses bleeding risk for pts on anticoag. For stroke ppx o Higher score= greater bleeding risk 37. What is recommended for stroke ppx in A. Fib pts? DOACS recommended warfarin. 38. Which agent is the best choice for prevention or treatment for a pregnant woman with DVT? Pneumatic compression devices + or – LMWH preferred. Warfarin is teratogenic, switch back to warfarin in pts with mechanical heart valve or inherited thrombophilia than converted back to LMWH closer to delivery. Monitoring the anti-Xa levels are recommended with LMWH use. 39. Where can a patient inject Enoxaparin? On the left or right side of tummy 2 inches from belly button Don't rub inj site