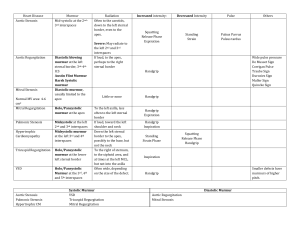
Mansoura University - Faculty of Medicine Mansoura – Manchester Programme for Medical Education Year 3. Semester 5 Cardiology Module Cardiology Module Name of lecture The information included in this presentation are not the only source for this topic and you should explore other valuable references in order to satisfy the ILOs of this topic. Cardiology Module Name of lecture Cardiac Murmurs By Prof. Ayman Abdelaziz Cardiology Module Name of lecture Intended Learning Outcomes (ILOs) • • • • • • • Define and Classify for cardiac murmurs Outline how heart murmurs described and graded How to auscultate for murmurs Systolic murmurs differential diagnosis Diastolic murmurs differential diagnosis Causes of continuous murmurs Innocent Murmurs Cardiology Module Name of lecture Cardiac Murmurs • Murmurs due to turbulent blood flow • Cardiac murmurs divided into three categories based on where they occur in the cardiac cycle. Cardiology Module Name of lecture Cardiac chambers, vessels pressure Cardiology Module Name of lecture What if you hear something? • • • • • • • Is it systolic, diastolic, or both? Where is it loudest? Does it radiate? Characteristics of Murmurs Intensity Maneuvers Are there other associated findings? • S2 splitting normal, loud P2, gallop sound? Murmurs Timing • Murmurs are prolonged in time while sounds are instantaneous Timing with carotid pulsation Intensity of Murmur Grade 1 just audible with a good stethoscope in a quiet room Grade 2 quiet but readily audible with a stethoscope Grade 3 easily heard with a stethoscope Grade 4 a loud, obvious murmur with a palpable thrill Grade 5 very loud, heard only over the pericardium but elsewhere in the body Grade 6 heard with stethoscope off chest Cardiology Module Name of lecture Murmur configurations Crescendo murmur Decrescendo murmur Crescendo-decrescendo murmur Plateau-shaped murmur Cardiology Module Name of lecture Systolic Murmurs Cardiology Module Name of lecture Pansystolic Murmur Causes: • Mitral regurgitation (MR) • Tricuspid regurgitation (TR) • Ventricular septal defect (VSD) Cardiology Module Name of lecture Systole LA AO RV LV Mitral Regurgitation Systole Early Mid S1 • Mitral Regurgitation Diastole Late Early S2 Mid Late Mitral Regurgitation • Rheumatic, Endocarditis, ischemic heart disease • High frequency, holosystolic, plateau murmur • Location: apex • Radiation: to the left axilla or back • Can radiate along left sternal border if posterior leaflet is affected • Can be associated with a loud S3 • Can be more intense with isometric handgrip Pansystolic murmur Tricuspid regurgitation • Pansystolic • Site : lower left sternal border • Increase with inspiration (Carvallo sign) Ventricular septal defect: Pansystolic Lower sternal border 4th, 5th intercostal space Radiation: all over precordium Associated with systolic thrill Cardiology Module Name of lecture Differential diagnosis of pansystolic murmur Mitral regurgitation Tricuspid regurgitation VSD Best heard Apex Lower left sternal area Left sternal border 3rd, 4th intercostal space Radiation Axilla , back No selective propagation All over pericordium Thrill rare no Common systolic thrill Character High pitched, soft, blowing High pitched, soft, blowing Medium pitched, rough , harsh Respiration No change Increase with inspiration Increase with expiration Associated features Decrease S1, S3 RVH, prominent V wave in Biventricular enlargement jugular pulse Ejection systolic murmur Causes 1. Aortic stenosis (valvular, supravalvular, subvalvular) 2. Hypertrophic cardiomyopathy (HCM) 3. Dilated aortic root. 4. Pulmonary stenosis (valvular, supravalvular, subvalvular) 5. Dilated pulmonary artery. 6- Hyperdynamic state Cardiology Module Name of lecture Aortic Stenosis • Congenital, rheumatic, degenerative-calcific • Site: right base (second right intercostal space) • Radiation: Neck, the right carotid - Can have a more musical quality at the apex (Gallavardin effect) • Crescendo-decrescendo, harsh , ejection systolic murmur (Peak in mid to late systole murmur) • The later the murmur peak, the more severe the stenosis Aortic Stenosis Systole Early S1 • Aortic Stenosis Mid Diastole Late Early S2 Mid Late Pulmonary Stenosis • Congenital • Site: left base (second left intercostal space) • Radiation: lower left sternal border • Crescendo-decrescendo, harsh , ejection systolic murmur late systolic murmur • Causes: Mitral valve prolapse Cardiology Module Name of lecture Diastolic Murmurs LA AO LV Cardiology Module Name of lecture Mid diastolic murmur causes • • • • Mitral stenosis Tricuspid stenosis : increases with inspiration Austin flint murmur in severe aortic regurgitation Acute Rheumtic valvulitis (Carey Coombs murmur) • Increased flow across nonstenotic mitral valve (eg, MR, VSD, PDA, highoutput state) • Increased flow across nonstenotic tricuspid valve (eg, TR, ASD) Cardiology Module Name of lecture Mitral Stenosis • Rheumatic, congenital • Timing: Mid diastolic with presystolic accentuation • Site : apex • Radiation : localized (not radiating) • low frequency rumbling • Special position: better heard in left lateral position. best heard with the bell of the stethoscope. • Often associated with opening snap and loud S1 • Can be confused with Austin Flint murmur Left lateral decubitus Mitral Stenosis Systole Early S1 • Mitral Stenosis Mid Diastole Late Early S2 Mid Late Austin flint Murmur of Aortic regurgitation • Middiastolic murmur • Murmur arises from aortic regurgitant jets causing premature closure of the MV Cardiology Module Name of lecture Early diastolic murmur Causes: • Aortic insufficiency • Aortic dilatation or aneurysm • Pulmonic regurgitation : increase with inspiration • Pulmonary hypertension (Graham steell murmur) • Dilatation of the pulmonary artery Cardiology Module Name of lecture Aortic Insufficiency • Congenital (with AS), rheumatic, endocarditis • Timing : early diastolic • Site: 1st aortic area ( second right intercostal space second aortic area (3rd left intercostal space) • High frequency (blowing), decrescendo, diastolic murmur • Radiation: left lower sternal border if its due to 1ry valve dse - Radiation to the right sternal border if AR is due aortic root dilatation • Position: patient sitting, leaning forward, hold breath in expiration • Best heard with diaphragm AR easily missed Aortic Insufficiency Systole Early Mid S1 • Aortic Insufficiency Diastole Late Early S2 Mid Late Etiology of diastolic murmurs Early diastolic murmur - Aortic regurgitation - Functional pulmonary regurgitation ( Graham steell murmur) Mid diastolic murmur - Mitral stenosis - Tricuspid stenosis Presystolic murmur - MS - TS - Mitral diastolic flow murmurs: as in severe MR, left to right shunt (VSD and PDA) - AR (Austin flint) - Tricuspid diastolic flow murmurs: severe TR, left to right shunt (ASD) - Severe Aortic regurgitation (Austin flint murmur) - Acute Rheumatic carditis (Carrey coombs murmur) Continuous murmur Causes: • Patent ductus arteriosus (PDA) • Aorto-pulmonary window • Coronary arteriovenous fistula • Ruptured sinus of Valsalva aneurysm • Anomalous left coronary artery from the pulmonary artery • Bronchial collateral circulation • Pulmonary arteriovenous fistula • Mammary souffle of pregnancy • Cervical venous hum Patent Ductus Arteriosus (PDA): Gibson Murmur • Site : left infraclavicular and pulmonary area • “Machinery/continuous” murmur typically enveloping S2 • If pulmonary HTN develops, the murmur may systematically disappear (with reversal of flow) Patent Ductus Arteriosus Systole Early Mid S1 • Patent Ductus Arteriosus Diastole Late Early S2 Mid Late PDA Cardiology Module Name of lecture Innocent Systolic Murmur Caused by high flow in outflow tracts, common in children, anemia, fever, high output states Localized to either pulmonic or aortic areas (not radiating) - Short systolic murmur Soft (not be more than grade 3) Symptoms free Sounds normal Signs free The Cardiac Cycle: Events Systole Early Mid S1 Diastole Late Early Mid S2 • Ejection Sound • Opening Snap • Mid Systolic Click • S3 • Late Systolic Murmur (MVP) • S4 • Pericardial Rub Late Cardiology Module Name of lecture Review S1 S Early diastolic murmur of AR Pansystolic murmur of MR Ejection systolic murmur of AS S3 S4 Mid diastolic murmur of MS Cardiology Module Name of lecture Review Left lateral position for mid diastolic murmur of MS Timing with carotid pulsation Cardiology Module Name of lecture Review Right lateral position for pansystolic murmur of TR Cardiology Module Sitting , leaning forward for early diastolic murmur of AR Name of lecture Summary and wrap up • Murmurs could be systolic, diastolic and continuous murmurs • Pansystolic murmur is caused by mitral and tricuspid regurgitation and ventricular septal defect • Ejection systolic murmur is due to aortic stenosis, and pulmonary stenosis • Mid diastolic murmur main cause is mitral stenosis and should be differentiated from Austin flint murmur of severe aortic regurgitation • Early diastolic murmur heard in patients with aortic regurgitation and pulmonary regurgitation (Graham steell murmur) • Continuous murmur heard in PDA and AV fistula Cardiology Module Name of lecture References & recommended readings • Clinical Examination Epstein 2nd ED • Oxford Handbook of Clinical Examination & Practical Skills - 1st E Cardiology Module Name of lecture