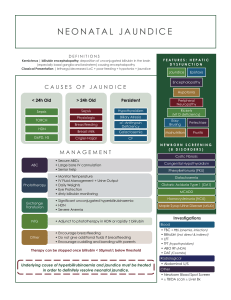
SCHOOL OF NURSING AND MIDWIFERY DEPARTMENT OF MIDWIFERY AND WOMEN’S HEALTH COURSE CODE: MDW 341 COURSE TITLE: PAEDIATRIC NURSING I JAUNDICE IN NEWBORNS i. PHYSIOLOGICAL AND INFECTIVE (Pathological) JAUNDICE ii. ABO and RHESUS INCOMPATIBILITY iii. EXCHANGE TRANSFUSION MR. HAMIDU NABILA YAKUBU (MPhil, PGDE, BSc., RN.Dip) WHAT JAUNDICE IS… • Jaundice is the yellowish discoloration of the skin, sclera and nails as a result of accumulated bilirubin in the blood. This is called HYPERBILIRUBINEMIA. • The condition is common in newborns and may be benign where no underlying condition is noted. It may also be pathologic in severe cases. • There are two forms of hyperbilirubinemia (conjugated/direct and unconjugated/indirect ) • Unconjugated hyperbilirubinemia is most commonly seen in newborns. PATHOPHYSIOLOGY • Rapid RBCs breakdown to release hemoglobin (RBC hemolysis) RBC lifespan in neonates is 70-90 days. • Hemoglobin splints into heme & globin(protein) • Heme fraction is converted into unconjugated bilirubin (bound to albumin which is insoluble i.e it is fat/lipid soluble) • The bilirubin detaches from the albumin when it moves to the liver. • An enzyme (glucuronyl transferase) converts the unconjugated bilirubin to conjugated bilirubin (highly soluble i.e it is water soluble) and excreted into the bile. • It is reduced by bacterial activity in the intestines to urobilinogen and stercobilinogen and released in urine and faeces (Process occurs in older children). PATHOPHYSIOLOGY CONT’D • However, in the newborn, because of poor peristalsis and relatively sterile bowel, conjugated bilirubin is converted back into unconjugated bilirubin by hydrolysis with glucurodinase. • It is then absorbed in the bowel and re-enters circulation for further liver metabolism. This type is called ENTEROHEPATIC CIRCULATION. TYPES OF JAUNDICE IN NEWBORNS • Almost all infants have some form of jaundice called PHYSIOLOGIC JAUNDICE (Icterus Neonatarum). Occurs after 24hours of life. • It has two phases: • First phase: bilirubin levels gradually increase to about 6mg/dL on 3rd day of life and decrease to 2-3mg/dL by 5th day of life • Second phase: maintains 2-3mg/dL levels until 12-14 days by which time levels decrease to normal (1mg/dL). This phenomenon is influenced by factors like racial group, method of feeding and gestational age. Bilirubin levels may go as high as 10-12 mg/dL at 4-5 days and reduce over 2-4 weeks period. TYPES OF JAUNDICE IN NEWBORNS CONT’D • Breastfeeding is tied to an increased level of jaundice. Two forms are related here: BREASTFEEDING ASSOCIATED JAUNDICE and BREAST MILK JAUNDICE. • Breastfeeding associated jaundice (early onset): onset is 2nd to 4th day of life. Levels rise 3rd -5th day. When mother’s milk is still not enough and baby has decreased amounts of caloric and fluid intake. This results in fasting/starving which is associated with decreased hepatic bilirubin clearance. Occurs in 10-25% of breastfed newborns. • Breast milk jaundice (late onset): onset is 5th-7th day of life and occurs in 2%-3% of breastfed newborns. Levels rise 10th-15th day and may persists for 3-12 weeks or more. TYPES OF JAUNDICE IN NEWBORNS CONT’D • Pathological jaundice: the following are indicators of pathologic jaundice that, when present, require further investigation as to the cause of the jaundice. • • • • • Onset is within 24 hours of life. Persistent jaundice after 1 week (term neonate) or 2 weeks (preterm) Total serum bilirubin levels 12-13mg/dL Increase in serum bilirubin 5mg/dL per daily Direct bilirubin 1.5-2mg/dL Possible causes of hyperbilirubinemia in newborns 1. Prematurity 2. An association with breast-feeding or breast milk 3. Excess production of bilirubin (e.g. hemolytic disease, Bio-chemical defects-maternal use of salicylates, sulphonamides; bruises) 4. Disturbed capacity of liver to secrete conjugated bilirubin (e.g. enzyme deficiency, bile duct obstruction) 5. Combined overproduction and undersecretion of bilirubin (e.g. sepsis) 6. Metabolic conditions (e.g. galactocemia, hypothyroidism, IDM) Summary of causes hyperbilirubinemia in newborns Diagnostic Evaluation • Evaluation of jaundice, apart from serum bilirubin levels, is also based on the following factors: 1. 2. 3. 4. Timing of the appearance of clinical jaundice Gestational age at birth Family history (maternal Rh factor) Feeding method INVESTIGATIONS INCLUDE: • Hemoglobin • Blood Film for red cell morphology • Infection screen • Maternal antibodies titre (indirect coombs test) • Direct antibody test (direct coombs test) • Maternal & infant blood group Complications of jaundice in newborn • Bilirubin encephalopathy (kernicterus): unbounded unconjugated bilirubin is fat-soluble and can cross the blood-brain-barrier (BBB) It should be noted that: bilirubin crosses the BBB under these circumstances: • When serum bilirubin concentration is markedly elevated • When serum albumin concentration is markedly low (eg, in preterm infants) • When bilirubin is displaced from albumin by competitive binders like certain drugs (eg, sulfisoxazole, ceftriaxone, aspirin) and free fatty acids and hydrogen ions (eg, in fasting, sepsis, or acidotic infants) • Intracranial infections e.g. meningitis Management of hyperbilirubinemia in newborns Aim is to prevent bilirubin encephalopathy. • Phototherapy (fluorescent light to exposed skin. Photoisomerization will alter bilirubin structure to soluble form (lumirubin) for excretion. Effectiveness is within first 24-48hours of treatment. • Exchange transfusion (this is mainly for reducing dangerously high bilirubin levels that occur with hemolytic disease) • Early initiation of feedings and frequent breastfeeding to promote bowel motility, decrease enterohepatic shunting and establishing normal bacterial flora in the gut to effectively enhance excretion of unconjugated bilirubin. Management of hyperbilirubinemia in newborns cont’d • Monitor bilirubin levels • Provide emotional support to parents by explaining all procedures with benefits and risks involved • Assess parents level of understanding of treatment involved and give clarification of the nature of treatment. Care during phototherapy • Infant should be nude under the light source. • Frequent reposition to expose all body parts to the light. • Shield infant’s eyes with an opaque mask to prevent exposure to light • Check infant’s eyes for evidence of discharge, excessive pressure on the lids or corneal irritation. Care during phototherapy cont’d • Feed infant intermittently, but remove eye shields during feeding to allow for visual and sensory stimulation. • Monitor temperature to prevent hyper/hypothermia • Maintain infant in a flexed position with rolled blankets along the sides of the body to help maintain heat comfort. • Observe skin for dehydration and drying, which can result to excoriation and breakdown. Avoid oily lubricants or lotions on skin to prevent increased tanning i.e. ‘a frying effect’ Care during phototherapy cont’d • Keep records of the following: • Start and stop time of phototherapy. • Type of fluorescent lamp used • Number of lamps • Distance between lamps and body of infant (no less than 18 inches). • Use of phototherapy in combination with an incubator • Photometer measurement of light intensity • Occurrence of side effects (loose, greenish stools, transient skin rashes, hyperthermia, increased metabolic rate, dehydration, electrolyte disturbances[hypocalcemia], and Priapism HEMOLYTIC DISEASE OF THE NEWBORN Hyperbilirubinemia in the first 24hours of life is most often the result of hemolytic disease of the newborn (HDNB) ERYTHROBLASTOSIS FETALIS-abnormal rate of RBCs destructions causing anemia. CONCEPT OF BLOOD INCOMPATIBILITY • On the membranes of human blood cells are a variety of antigens (agglutinogens). • These are capable of producing an immune response if recognized by the body as foreign. • Antibodies are found in the plasma while antigens are on the RBC. When antibodies in the plasma of one blood group is mixed with antigens of a different blood group it produces agglutination. CONCEPT OF BLOOD INCOMPATIBILITY CONT’D • Antibodies occur naturally in the ABO blood group system. • In the Rh system, the antibodies are formed when the person is exposed to the Rh antigen. The exposure will cause sensitivity response known as Isoimmunization Rh Incompatibility (isoimmunization) • There are many antigens in the Rh blood group. And ‘D’ is the most prevalent of the antigens. • Rh positive means the presence of the antigen. • Rh negative means the absence of the antigen • Therefore the presence or absence of the Rh factor determines the blood type • If Rh blood type of mother and fetus are the same, Or if mother is Rh positive and fetus is Rh negative, there will be no problem. Rh Incompatibility (isoimmunization) cont’d • However, if mother is Rh negative and fetus is Rh positive, a problem might develop. • HOW WILL THE PROBLEM DEVELOP? • Fetal blood mixes with maternal blood through breaks in placental vessels. An Rh positive fetus antigens enters maternal blood which is Rh negative. • There is production of anti-Rh antibodies. • In subsequent pregnancies, the Rh antigens from fetus cross to mother to stimulate these anti-Rh antibodies which enters into fetal blood and cause hemolysis. Factors that increase incidence of transplacental haemorrhage • Multiple gestation • Abruption placenta • Placenta previa • Manuel placental delivery • Caesarean section Instances when mother does not become sensitized though exposed to Rh positive blood • In a strong placental barrier where fetal blood does not cross to mother. • Immunological inability of mother to produce anti-Rh antibodies. Complications • Progressive hemolysis result in: • • • • • Fetal hypoxia Cardiac failure Generalised edema (anasarca) Pericardial, pleural and peritoneal effusions Severe respiratory distress ABO INCOMPATIBILITY Major blood group’s antigens of the fetus are different from those of the mother. Major blood groups are: (A, B, AB, and O). Naturally occurring antibodies in the recipient’s blood cause agglutination of a donor’s RBCs. ABO INCOMPATIBILITY • ABO incompatibility is more common that Rh incompatibility and also less severe in hemolytic reaction. • Most common blood group incompatibility in the neonate is between a mother with O blood group and an infant with A or B blood group. • Mother’s O blood group has naturally an anti-A and anti-B antibodies already present in maternal circulation. They will cross the placenta and attack the fetal RBCs causing hemolysis. • ABO incompatibility may occur in the first pregnancy Potential Maternal-Fetal ABO Incompatibilities MATERNAL BLOOD GROUP INCOMPATIBLE FETAL BLOOD GROUP O A or B B A or AB A B or AB Clinical Manifestations • Jaundice may set in within the first 24hours • Rising levels of serum unconjugated bilirubin. • Marked pallor • Hypovolemic shock • hypoglycaemia Diagnostic Evaluation • Indirect comb’s test for maternal antibody at first prenatal visit • Amniocentesis for fetal blood type if mother antibody screen is positive or • Amniocentesis using polymerase chain reaction to determine fetal blood type. • Ultrasonography to detect alteration in the placenta, umbilical cord and amniotic fluid volume EXCHANGE TRANSFUSION • 5-10mL blood is removed at a time, and replaced with compatible blood like Rh negative blood. Donor’s blood is usually double of infant’s blood. • Removes the sensitized erythrocytes, lowers serum bilirubin level to prevent bilirubin encephalopathy, correct anemia and prevent cardiac failure HOW EXCHANGE TRANSFUSION IS DONE • Catheter inserted into umbilical vein and threaded to the inferior vena cava. • 5-10ml blood drawn within 15-20seconds • Same volume donor blood infused over 60-90 seconds • If blood is citrated, give calcium gluconate after every 100ml of donor blood to prevent hypocalcemia