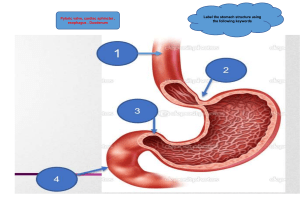
Nursing Care and Interventions NURS3105 Dr. Jane Tyerman Copyright © 2014 Elsevier Canada, a division of Reed Elsevier Canada, Ltd. • Electrocardiogram (P, QRS, T, U waveforms) • P wave - depolarization of the atria. • QRS complex - depolarization of the ventricles. • T wave - repolarization of the ventricles. • U wave, if present - repolarization of the Purkinje fibres or may be associated with hypokalemia. • PR, QRS, and QT intervals reflect the length of time it takes for the impulse to travel from one area of the heart to another. Cardiac output (CO) = blood pumped/min Normal 4-8L/min (Ave 5L/min) Cardiac index (CI) Heart rate (HR) Stimulation from SNS Stimulation from PNS Stroke volume (SV) = beat SV = CO/HR Average 75 ml Cardiac reserve Increase HR or SV Pulse pressure (40 mmHg) Differences between SBP and DBP Normally 1/3 of SBP Mean Arterial Pressure (MAP) MAP = SBP + 2(DBP) 3 Indicator of blood flow (better than SBP) MAP >60 needed to maintain adequate tissue perfusion Commonly used to titrate medication MAP 65 (ie. Norepinephrine/Levophed) Volume of blood in ventricles at end of diastole Affected by the amount of blood delivered to the heart Starling’s Law: greater stretch = greater preload Conditions that diminish preload: Decreased blood volume (hemorrhage, dehydration, shock) AV valve dysfunction (hinder free flow into ventricle) Vasodilation (increase vascular space, same volume) Conditions that increase preload Increase blood volume (renal failure, fluid resus, increased aldosterone) Poor EF/CHF-”back up” d/t inability to eject The heart's ability to function as a pump Ejection Fraction: index of myocardial function (60%) Percentage of blood ejected with each stoke volume SV divided by end diastolic volume Conditions that affect contractility ↑ contractility (Inotropes) and vasoconstriction Calcium release Digoxin, dopamine, dobutamine ↓ contractility: HYPOXIA (considered negative inotrope) ischemia and drugs (narcotics, anesthetics) Myocardial Contractility and Calcium Influx Cardiac muscle does not store calcium like skeletal muscles Importance of serum calcium levels and medications that affect calcium Calcium 2.25 – 2.75 mmol/L The peripheral resistance against which the left ventricle must pump The relationship among flow, resistance, and pressure Arterial pressure=flow (CO) x resistance (afterload) Impact of afterload on CO If afterload ↑, CO ↓, arterial pressure ↑ If afterload ↓, CO ↑, arterial pressure ↓ Conditions that affect afterload ↑ afterload: vasoconstriction- SNS, hypertension, renal failure, increase volume, medications, stenosis of valve impeding EF ↓afterload: • vasodilation- PNS, shock, spinal cord injury Stimulation of SA and AV nodes Conditions that: increase heart rate SNS stimulation Pain, anxiety, fear, perceived threats, medications Conditions that cause ↓ SV (to maintain CO) Cardiac conduction syndromes (WPW) Conditions that: decrease heart rate PNS stimulation (muscarinic receptors/vagal nerve) Valsalva Medications, conduction issues Subjective data Past health history Past and current medications Surgery or other treatments Cues to cardiovascular problems Fatigue, abdominal obesity, fluid retention, irregular heart rate, dyspnea, pain, calf tenderness, dizziness, altered neurological function, leg pain Objective data Physical examination Vital signs Peripheral vascular system Inspection: Colour, hair distribution, venous blood flow, edema, jugular veins Palpation: Neck and extremity pulses, pressure of pulse wave, rigidity of vessel Auscultation: Major arteries, bruit assessment Copyright © 2014 Elsevier Canada, a division of Reed Elsevier Canada, Ltd. Auscultation • S1 = the closure of the tricuspid and mitral valves (AV atrial ventricular) valves = LUB • S2 = the closure of the aortic and pulmonic valve (semilunar) = DUB -Extra heart sounds (best heard with the bell of a stethoscope as they are low-pitched) • S3 = ventricular vibration (mitral valve regurgitation • S4 = occurs in patients with CAD, left ventricular hypertrophy or aortic stenosis Noninvasive studies Chest radiograph Electrocardiogram Ambulatory electrocardiogram monitoring Transtelephonic event recorder Exercise or stress testing Echocardiogram EF, valves, chamber size Nuclear cardiology Magnetic resonance imaging (MRI) Computed tomography (CT) – CAD Blood studies Cardiac markers (serial CKs) • CK, CKMB (4-6 h), Troponin I or T (6 h) Serum lipids Lipoprotein-associated phospholipase A2 • athrosclerosis C-reactive protein Homocysteine • Risk of CAD, stroke, thromboembolism Cardiac natriuretic peptide markers (CNPM) • Distinguish between cardiac and respiratory cause of dyspnea Invasive studies • Cardiac catheterization and coronary angiography • Electrophysiology study – node function • Intracoronary ultrasound • Blood flow and pressure measurements • Peripheral vessel blood flow • Hemodynamic monitoring Nursing Management: Hypertension High blood pressure is one of the most important modifiable risk factors that lead to cardiovascular disease. 35-23 35-24 Cardiac output (CO) is the total blood flow through the systemic or pulmonary circulation per minute. CO can be described as stroke volume (SV, or the amount of blood pumped out of the left ventricle per beat [~70 mL]) multiplied by the heart rate (HR) for 1 minute. Systemic vascular resistance (SVR) is the force opposing the movement of blood within the blood vessels. 35-25 • Sustained elevation of systemic arterial blood pressure (BP) • High BP is the most significant modifiable risk factor for cardiovascular disease and mortality in Canada. • As BP increases, so does the risk for myocardial infarction (MI), heart failure, stroke, and renal disease. 35-26 Normal BP: 120 mm hg/80 mm Hg Persistent elevation of Systolic blood pressure (SBP) ≥140 mm Hg or Diastolic blood pressure (DBP) ≥90 mm Hg or Current use of antihypertensive medication(s) 35-27 • Age • Women • Indigenous people • ‘Silent Killer’ 35-28 Isolated systolic hypertension (ISH) Sustained elevation of SBP ≥140 mm Hg and a DBP <90 mm Hg Common in older persons, related to loss of elasticity in large arteries 35-29 Primary (essential) hypertension • • Majority of adult patients Focus on primary hypertension related to prevalence in clinical practice Secondary hypertension • • • 5 to 10% of adults Many causes; treatment aimed at eliminating the underlying cause Contributing factors to hypertensive urgency 35-30 Primary (essential) hypertension Contributing factors • • • • • • ↑ SNS activity ↑ Sodium-retaining hormones and vasoconstrictors ↑ Sodium intake Diabetes mellitus > Ideal body weight Excessive alcohol intake 35-31 • Advancing age • Heavy alcohol consumption • Cigarette smoking • Diabetes mellitus • Elevated serum lipids • High dietary sodium • Gender 35-32 Clinical findings that suggest secondary hypertension include • Unprovoked hypokalemia • Abdominal bruit • Variable pressures with a history of tachycardia, sweating, and tremor • Family history of renal disease 35-33 Causes • Coarctation or congenital narrowing of the aorta • Renal disease such as renal artery stenosis and parenchymal disease • Endocrine disorders such as pheochromocytoma, Cushing’s syndrome, and hyperaldosteronism • Neurological disorders such as brain tumours, quadriplegia, and head injury • Sleep apnea • Medications • Pregnancy-induced hypertension Genes Sodium and water retention Altered renin–angiotensin–aldosterone mechanism Stress and increased SNS activity Insulin resistance and hyperinsulinemia Endothelial cell dysfunction Obesity The animation referenced below can be viewed in the PowerPoint Animations asset. Aldosterone Regulation Mechanism 35-36 Hypertension is a silent disease. Frequently it is asymptomatic until it becomes severe and target-organ disease has occurred. Secondary symptoms with severe hypertension include fatigue, reduced activity tolerance, dizziness, palpitations, angina, and dyspnea. Hypertensive heart disease Coronary artery disease Left ventricular hypertrophy Heart failure Cerebrovascular disease Peripheral arterial disease Nephrosclerosis Retinal damage • Urinalysis • Blood chemistry (potassium, sodium, blood urea, and creatinine) • Fasting blood glucose • Fasting total cholesterol and high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, and triglycerides • Standard 12-lead electrocardiography • Assess urinary albumin excretion in patients with diabetes • All patients with treated hypertension need to be monitored for the appearance of diabetes. • Ambulatory blood pressure monitoring • 24-hour readings • Useful in diagnosis of uncomplicated mild-tomoderate hypertension • Helpful in patients with suspected white coat hypertension, masked hypertension, apparent medication resistance, hypotensive symptoms with hypertensive medications, episodic hypertension, or autonomic nervous system dysfunction Risk stratification Lifestyle modifications Nutritional therapy Weight reduction Modification in alcohol consumption Physical activity Avoidance of tobacco products Stress management FIG. 35.3 Treatment of systolic/diastolic hypertension (HTN) without other compelling indications. Nursing assessment Subjective data • Important health information • Symptoms: Dyspnea, fatigue, intermittent claudication, nocturia, dizziness, erectile dysfunction Objective data • Cardiovascular: BP, pulse • Musculoskeletal: Truncal obesity • Neurological: Mental status changes • Possible findings Medications” • Diuretics (Furosemide, HCTZ) • Antihypertensives (ACE Inhibitors, Calcium Chanel blockers) Overall goals Achieve and maintain target BP Understand and implement therapeutic plan Minimal or no unpleasant adverse effects Confident of ability to manage and cope with condition Adherence Nursing implementation Health promotion • Individual patient evaluation • Screening programs • Cardiovascular risk factor modification Ambulatory and home care • Physical activity • Home blood pressure monitoring • Patient adherence Evaluation 35-45 Hypertension is common in individuals age 60+ years. Age-related changes • Loss of tissue elasticity • Increased collagen content and stiffness of the myocardium • Increased peripheral vascular resistance • Decreased β-adrenergic receptor sensitivity • Blunting of baroreceptor reflexes • Decreased kidney function • Decreased renin response to sodium and water depletion • Severe, abrupt increase in DBP (defined as >120–130 mm Hg) • Rate of increase in BP is more important than the absolute value • Often occurs in patients with a history of hypertension who have failed to adhere to their medication regimen or who have been undermedicated Nursing Management: Coronary Artery Disease and Acute Coronary Syndrome Heart disease is the second major cause of death in Canada, with 27.6% of all deaths. 2.4 million Canadians over age 20 will experience ischemic heart disease. 36-49 36-50 Prevalent Etiologies of CAD CAD is one of the leading Atherosclerosis: partially or causes of morbidity and completely blocked coronary mortality in the US and Canada. arteries Coronary vasospasm CAD results in ischemia and infarction of myocardial tissue. Microvascular angina LAD (left anterior descending artery) is most commonly affected. Highly sensitive CRP (hsCRP) Reduction of Risk Factors Smoking cessation Weight loss–DASH Lowering cholesterol levels Glycemic control Stress reduction Medication compliance ↑ Activity/exercise CAD is one of the leading causes of morbidity and mortality in Canada. CAD results in ischemia and infarction of myocardial tissue. LAD (left anterior descending artery) is most commonly affected. Highly sensitive CRP (hsCRP) 36-52 36-53 The animation referenced below can be viewed in the PowerPoint Animations asset. Coronary Artery Disease 36-54 Risk factors for coronary artery disease Nonmodifiable risk factors • • • • Age Gender Ethnicity Family history and genetics 36-55 Modifiable major risk factors • • • • • Elevated serum lipid levels Elevated blood pressure (BP) Tobacco use Physical inactivity Obesity 36-56 Modifiable contributing risk factors • • • • • Diabetes mellitus Elevated fasting bold glucose level Psychosocial risk factors Homocysteine elevation Substance use 36-57 Health promotion • Identification of people at high risk • Management of people at high risk • Physical activity Nutritional therapy • Reduce serum triglyceride • Ideal body weight • Cholesterol <200 mg/day 36-58 36-59 Cholesterol-lowering medication therapy Antiplatelet therapy Beta Blockers Nitrates Calcium channel blockers Thrombolytics 36-60 Morphine Sulfate Analgesic; ↓ anxiety; ↓ tachypnea; relaxes bronchial smooth muscle; improves gas exchange β-Blockers ↓heart rate; ↓workload of heart; ↓ oxygen demand of myocardium Calcium Channel Blockers ↓conduction through AV node; slow heart rate; ↓ oxygen demand by myocardium Thrombolytic Therapy (within protocol guidelines) Useful when infarction is diagnosed early; streptokinase and tPA; administered IV Most effective if given within 6 hours of onset of chest pain; heparin therapy will usually follow thrombolytic therapy Four heart valves: • Tricuspid and mitral valves • Pulmonic and aortic valves • Prevent regurgitation • Open and close in response to pressure gradient changes • Thickened and stenotic valve leaflets • Caused by Rheumatic fever (main) Calcification Congenital factors Mitral Valve Stenosis Early period—may have no symptoms Later—excessive fatigue, dyspnea on exertion, orthopnea, dry cough, hemoptysis, or pulmonary edema Rumbling apical diastolic murmur and a-fib are common Nursing and Collaborative Management CHF care Monitor for a-fib with thrombus formation Prophylactic antibiotic therapy before any invasive procedures (dental, surgical, childbirth) May require surgical repair or valve replacement Teach about the need for lifelong anticoagulant therapy if valve replacement done Mitral valve regurgitation (MR) • Insufficient or incompetent mitral valve (prolapse) • Regurgitation of blood back into LA • Can lead to left sided heart failure Aortic valve regurgitation (AR) – aka aortic insufficiency • Incompetent aortic valve, allows blood from aorta back into LV during diastole • LV hypertrophy to maintain SV • Systolic murmur • Rheumatic fever Etiology CAD, prior MI Chronic HTN Cardiomyopathy Thyroid Diabetes Valvular and congenital heart disease Pulmonary diseases Progressive→ cardiac remodeling to maintain stroke volume and cardiac output LV remodeling d/t disease process CAD, DM, cardiomyopathy, valvular heart disease Etoh, drug abuse Hyperlipidemia, HTN Risk Factors – Table 13-4 Causes: LV infarct, cardiomyopathy, hypertension Symptoms: shortness of breath, cough, orthopnea, pulmonary edema, paroxysmal nocturnal dyspnea Signs: S3 gallop, tachycardia, inspiratory rales beginning at lung bases, expiratory wheezes due to bronchospasms (misdiagnosed with asthma) Laboratory findings: • ABGs reveal hypoxemia • chest x-ray shows pulmonary edema or pleural effusions • ↑b-type natriuretic peptide (BNP) BNP levels greater than 500 ng/mL indicate heart failure is probable. Systemic Congestion Causes: LHF, RV infarct, pulmonary or tricuspid valve disease, pulmonary HTN, COPD, PE Symptoms: dyspnea on exertion, fatigue, weight gain, fluid retention Signs: ↑ CVP, JVD >3-4 cm, hepatomegaly, ascites, peripheral or sacral edema, and pleural and pericardial effusions Lab Tests: ↑ LFTs, ↑BUN/Cr, ↑ PT/INR, hyponatremia Other symptoms and signs Fatigue JVD, Edema, Crackles, S3 http://en.wikipedia.org/wiki/File:Elevated_JVP.JPG Classic respiratory symptoms Orthopnea Dyspnea Paroxysmal nocturnal dyspnea Diagnostic Echo, Doppler,12 lead Medications ACE Inhibitors ARBs Beta blockers Loop and Thiazide diuretics Daily weights Fluid restrictions Oxygen Reposition and perform coughing, and deep breathing exercises q2h Limit sodium intake Fluid restriction only if Na+ <132 mmol/L (mEq/L) Avoid excessive fluids Avoid alcohol Educate on signs of worsening condition such as weight gain 1.36 kg (3 lb) or 0.45-0.9 kg (1-2 lb) overnight; increasing DOE, orthopnea or PND. Regular exercise is strongly encouraged Supply vs demand Increased demands ↑ heart rate, ↑ contractility, ↑ preload Decreased supply CAD, spasm, anemia, hypoxemia, shock Age Gender Race Family history Hyperlipidemia Dietary Obesity Sedentary lifestyle Hypertension Smoking Diabetes Chronic kidney disease Metabolic syndrome Menopause Hyperhomocysteinemia Vascular inflammation Multifactoral Grade 1 Angina occurs with strenuous exertion Grade 2 Angina occurs w/walking 2 blocks or 1 flight of stairs Grade 3 Angina occurs w/walking < 2 blocks Grade 4 Rest angina Copyright © 2014 Elsevier Canada, a division of Reed Elsevier Canada, Ltd. Copyright © 2014 Elsevier Canada, a division of Reed Elsevier Canada, Ltd. Women Discomfort rather than pain Shortness of breath Extreme fatigue Clients with Diabetes Asymptomatic Neuropathy Dyspnea Elderly clients Confusion/delirium Dizziness Shortness of breath Copyright © 2014 Elsevier Canada, a division of Reed Elsevier Canada, Ltd. Diagnostic studies • • • • • 12 lead ECG Stress test Holter Echocardiogram Cardiac catheterization 12 Lead ECG ECG (12 lead) Confirm By Biomarkers Troponin Myoglobin Cardiac enzymes Drug therapy • Short-acting nitrates • Sublingual nitroglycerin • Long-acting nitrates • Nitroglycerin ointment • Transdermal controlled-release nitrates • β-Adrenergic blockers • Calcium channel blockers • Angiotensin-converting enzyme inhibitors Silent ischemia • Nocturnal angina and angina decubitus Prinzmetal’s (variant) angina • Occurs at rest Treatment • To prevent MI and reduce symptoms • ASA • ABCDEF Therapy (MONAM) Monitor Oxygen Nitroglycerin ASA Morphine β-Adrenergic blockers Angiotensin-converting enzyme inhibitors Antidysrhythmia drugs Cholesterol-lowering drugs Stool softeners Chest pain that is new in onset, occurs at rest, or has a worsening pattern. • Unstable angina is unpredictable and represents an emergency. • First manifestation of CAD • May evolve from chronic unstable angina • Symptoms more subtle in women - Fatigue SOB Indigestion anxiety Stable Angina • Predictable • Exertion induced • Pain relieved by Ntg + rest • Short lived <20 min Unstable Angina • New onset c/p that can occur many times per day • Pain is increasing in severity; unrelieved w/ Ntg • Rest angina • Indicative of unstable plaque • Preinfarct or crescendo