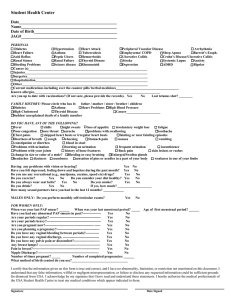
Date of Birth Year of first menstrual cycle Date of Last menstrual cycle How many days do you bleed for? How many days do you have a full flow of blood? How many days from your first day of bleeding to the next first day of your menstrual cycle? Do you have any spotting in between cycles? What is the color of your menstrual blood? Bright red? Dark red? Purple? Brown? Are there any clots? Do you have a heavy flow of blood or light flow? Do you have any pain, headaches, cramping, breast tenderness, bloating, gas around or during your menses? Please circle which ones and list anything else. How long have you tried to get pregnant in terms of months or years? Have you tried IVF and if so how many times? Has your husband’s sperm been analyzed and what was the result? Have you had any miscarriages? If so, how many and when? Are you tracking your ovulation? If so, on what day do you ovulate? Do you observe cervical discharge (white or creamy thick discharge or egg yolk like consistency) around ovulation time? Please describe what it is like Do you have any pain or bleeding during intercourse? Do you have annual pap smears? Have any been abnormal? When was last pap smear? Do you have any other medical conditions? Have you ever been diagnosed with cysts? If so, when? Are you taking any medications, herbs, or supplements? If so which ones? What do you eat for breakfast? What do you eat for lunch? What do you eat for dinner? How much caffeine do you consume? Cups? How many tea bags or spoons do you use? Do you or your husband smoke cigarettes? Do you exercise or get any physical exercise? If so, please describe it. Do you have a lot of stress in life? If so, what is the source?