Chapter13 The Brain and Cranial Nerves
advertisement

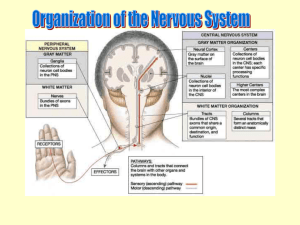
Chapter13 The Brain and Cranial Nerves Nervous System: Brain and Cranial Nerves • The Brain – Average weight of 1.35 to 1.4 kilograms – Outer surface folded in on itself – Four major regions: • • • • cerebrum diencephalon brainstem cerebellum – Cranial nerves originating here Overview of Brain Anatomy • Brain anatomy – With spinal cord, composes central nervous system – Outer surface • exhibits folds, gyri • shallow depressions, sulci • deeper grooves, fissures – Two common directional terms • anterior = rostral (“toward the nose”) • posterior = caudal (“toward the tail”) Brain Development and Organization: Overview of Brain Anatomy Brain Development and Organization Clinical View—Traumatic Brain Injuries: Concussion and Contusion – Traumatic brain injury • acute brain damage occurring as a result of trauma – Concussion • • • • most common type temporary loss of consciousness after blow to head headache, drowsiness, confusion, and amnesia possible may have a cumulative effect on intellectual abilities, personality, or mood – Contusion • bruising of brain due to trauma • loss of consciousness < 5 minutes – Second impact syndrome • individual with second injury prior to resolution of first trauma • develop severe brain swelling Gray Matter and White Matter Distribution • Two tissue areas of brain and spinal cord: – gray matter • color from motor and interneuron cell bodies, dendrites, and unmyelinated axons – white matter – color from myelin on axons – E.g., the cerebrum • superficial region of gray matter, termed cerebral cortex • covers surface • white matter deep to gray matter Protection and Support of the Brain • Brain protected and isolated by multiple structures – – – – The cranium provides rigid support The meninges surround and partition Cerebrospinal fluid cushions Blood-brain barrier prevents entry of harmful materials Cranial Meninges • Cranial meninges – Three connective tissue layers – Separate and support soft tissue of brain – Enclose and protect blood vessels supplying the brain – Help contain and circulate cerebrospinal fluid – From deep to superficial: • pia matter • arachnoid mater • dura mater Cranial Meninges Pia Mater – Innermost of cranial meninges Thin layer of areolar connective tissue – Tightly adheres to brain Follows contours of brain surface Arachnoid Mater – – – – Lies external to pia mater Partially composed of collagen and elastic fibers Extend through subarachnoid space contains cerebrospinal fluid Subdural space potential space between arachnoid and overlying dura mater • becomes actual space if blood or fluid accumulates there - subdural hematoma Dura Mater – Lies external to arachnoid mater – Tough, dense irregular connective tissue – Epidural space • potential space between dura mater and bones of the skull • contains arteries and veins nourishing meninges and cranium • becomes real space if blood or fluid accumulates Clinical View: Epidural and Subdural Hematomas – Epidural hematoma • pool of blood in epidural space of brain • usually due to severe blow to the head • adjacent brain tissue distorted and compressed • severe neurological injury or death unless bleeding stopped and blood removed – Subdural hematoma • hemorrhage in subdural space • typically from ruptured veins from fast rotational head movement • compression of brain tissue, more slowly than epidural hematoma Protection and Support of the Brain: Cranial Meninges Clinical View: Meningitis – Inflammation of the meninges – Typically caused by contagious viral or bacterial infections – Symptoms of fever, headache, vomiting, and stiff neck • pain from meninges sometimes referred to posterior neck – May result in brain damage and death if untreated – Bacterial meningitis with more severe symptoms – Vaccine for most common bacterial strains causing meningitis Protection and Support of the Brain: Cranial Meninges Cranial Dural Septa – Double layers of dura mater – Extend as flat partitions into the cranial cavity – Separate specific parts of the brain – Stabilize and support the brain – Four locations Protection and Support of the Brain: Brain Ventricles • Ventricles – Cavities within the brain – Derived from neural canal – Contain cerebrospinal fluid Cerebrospinal Fluid • Cerebrospinal fluid - Formed by choroid plexus – – – – Clear, colorless liquid Originates from blood plasma Circulates in ventricles and subarachnoid space Bathes and completely surrounds surfaces of CNS • functions: – buoyancy • brain floating here • reduces apparent weight by 95% • prevents collapse of brain through foramen magnum – protection • provides liquid cushion • protects delicate neural structures from sudden movements – environmental stability • transports nutrients and chemical messengers to brain • removes waste products (to venous circulation) • protects tissue from chemical fluctuations Figure 13.9a Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. CSF flow Arachnoid villi 5 Superior sagittal sinus (dural venous sinus) 4 Venous fluid flow Pia mater Choroid plexus of third ventricle 1 Choroid plexus of lateral ventricle Interventricular foramen 2 Cerebral aqueduct Lateral aperture Choroid plexus of fourth ventricle 3 Median aperture Dura mater Subarachnoid space Central canal of spinal cord (a) Midsagittal section Protection and Support of the Brain: Cerebrospinal Fluid Clinical View: Hydrocephalus – – – – – – Pathologic condition of excessive CSF Often leads to brain distortion May result from obstruction in CSF restricting reabsorption May result from intrinsic problem with arachnoid villi In a young child, head enlarged with possible neurological damage May be treated surgically • implant shunts that drain CSF to other body regions Protection and Support of the Brain: Blood-Brain Barrier • Blood-brain barrier (BBB) – Strictly regulates which substances enter brain’s interstitial fluid – Helps prevent neuron exposure to harmful substances • e.g., drugs • blood waste products • variations in levels of normal substances – e.g., ions, hormones • Barrier not absolute – Lipid-soluble compounds • • • • can diffuse across endothelial plasma membranes e.g., nicotine alcohol some anesthetics – Can be damaged by drugs such as cocaine Protection and Support of the Brain: Blood-Brain Barrier Brain: 2% of body wt, 15% of blood consumption, 20% of O2 and glucose consumptio Brain barrier system- strictly regulates what substances can get from bloodstream into brain tissue Blood-brain-barrier (BBB)tight junctions b/t brain and capillaries Astrocytes completely seal off gaps Exclude harmful substances Allow necessary ones to pass • Missing or reduced in 3 locations: – choroid plexus • needs to be permeable to produce CSF – hypothalamus and pineal gland • produce hormones requiring access to bloodstream Cerebrum • Cerebrum – Origin of all complex intellectual functions – Two large hemispheres on superior aspect of brain – Center of: • intelligence and reasoning • thought, memory, and judgment • voluntary motor, visual, and auditory activities • Cerebrum composition – Composed of two halves, left and right cerebral hemispheres – Separated by deep cleft, longitudinal fissure – Hemispheres separate, except at a few locations – Largest tract, corpus callosum • provides main method of communication between hemispheres Cerebrum: Cerebral Hemispheres • Cerebrum characteristics – Usually difficult to assign precise function to specific region • overlapping and indistinct boundaries • some aspects not easily assigned to any single region – e.g., memory – Innervation • hemispheres receiving information from opposite side of body • hemispheres projecting motor commands to opposite side of body • e.g., right cerebral hemisphere controlling the left side of body – Functional differences between hemispheres • termed cerebral lateralization • e.g., regions of brain responsible for speech in left cerebral hemisphere • primarily affects higher-order function Cerebrum: Lobes of the Cerebrum • Five Lobes – Four visible on external surface – Named for overlying cranial bones • frontal, parietal, temporal, and occipital • insula, not visible at surface (fifth lobe)- memory and taste Frontal lobe • Voluntary motor functions, motivation, foresight, planning, memory, mood, emotion, social judgment, aggression, decision making, personality Parietal lobe • receive and interpret signals of general senses – shape texture • Taste, touch, some visual Occipital lobe • Principal visual centervisual memory Temporal lobe • hearing, smell, learning, memory, some vision and emotion Cerebrum: Functional Areas of the Cerebrum • Structure and functions – Specific structural areas with distinct motor and sensory functions – Higher mental functions dispersed over large areas – Three categories of functional areas: • motor areas • sensory areas • association areas Cerebrum: Functional Areas of the Cerebrum Motor Areas – Control voluntary motor function – Housed within frontal lobes – Primary motor cortex located in precentral gyrus of lobe • control voluntary skeletal muscle activity • project contralaterally (opposite side) within brainstem or spinal cord • e.g., left primary motor cortex controlling right-side voluntary muscles – Motor speech area • also known as Broca area • located in inferolateral portion of left frontal lobe (in most people) • controls muscular movement for vocalization – Frontal eye field • on superior surface of middle frontal gyrus • regulates eye movements needed for reading and binocular visions Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Primary motor cortex (within precentral gyrus) Trunk Hip Knee Ankle Toes Figure 13.13a Pharynx Lateral Medial (a) Primary motor cortex (somatic motor area) Cerebrum: Functional Areas of the Cerebrum Sensory Areas – Primary somatosensory cortex • housed within postcentral gyrus of parietal lobes • receives somatic sensory information from: – proprioceptors, touch, pressure pain, and temperature receptors – Primary visual cortex • located within occipital lobe • receives and processes incoming visual information – Primary auditory cortex • located within temporal lobe • receives and processes auditory information – Primary olfactory cortex • located within temporal lobe • provides conscious awareness of smells – Primary gustatory cortex • located within insula • involved in processing taste information Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Leg Neck Hip Trunk Primary somatosensory cortex (within postcentral gyrus) Foot Toes Genitals Figure 13.13b Intra-abdominal Medial Lateral (b) Primary somatosensory cortex Cerebrum: Functional Areas of the Cerebrum Association Areas – – – – Connected to adjacent motor and sensory regions Process and interpret data or coordinate motor response Integrate new sensory inputs with memories Premotor cortex • within frontal lobe anterior to precentral gyrus • responsible for coordinating skilled motor activities – e.g., playing the piano Association Areas – Somatosensory association area • • • • within parietal lobe posterior to primary somatosensory complex integrates sensory information determines texture, temperature, pressure, and shape of objects allows us to identify known objections without seeing them Association Areas – Visual association area • • • • within occipital lobe surrounds primary visual area helps process visual information helps us identify things we see – Auditory association area • within temporal lobe • interprets characteristics of sound • stores memories of sound heard in the past – Functional brain regions • multi-association area between lobes • integrates information from individual association areas – Wernicke area, one example • typically located only in left hemisphere • involved in recognizing, understanding, comprehending language – Gnostic area, another functional brain region • composed of regions of parietal, occipital, and temporal lobes • provides comprehensive understanding of current activity Figure 13.12b Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. (b) Motor Areas Primary motor cortex Premotor cortex Motor speech area Control voluntary skeletal muscle activity Regulate skeletal muscle movements Involved with speech Plan and coordinate learned, skilled motor activities Figure 13.12c Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. (c) Sensory and Association Areas Primary visual cortex Primary gustatory cortex Visual association area Primary olfactory cortex Process taste information and provide conscious awareness of smells, respectively Process, integrate, and store visual information Primary auditory cortex Primary somatosensory cortex Auditory association area Somatosensory association area Process, interpret sounds, and store auditory memories Receive and interpret somatic information from receptors Figure 13.12d Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. (d) Functional Brain Regions Wernicke area Gnostic area Integrates all information being processed in adjacent lobes to provide a comprehensive understanding of a current activity This multi-association area helps understand spoken or written language. Cerebrum Clinical View: The Case of Phineas Gage – – – – – Famous neurological case in 1848 Rod shot through Gage’s head, below left eye Before accident, capable, well-balanced, and shrewd After accident, was irreverant, fitful, and profane Helped uncover link that frontal lobes are important in personality, and linked to basic elements of decision making Cerebrum: Cerebral Lateralization • Hemispheric asymmetries – Petalias, shape asymmetries of frontal and occipital lobes – Right frontal petalias Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Right frontal petalia Right-handed • right frontal lobe projection farther than the left frontal lobe – Left occipital petalias • left occipital lobe projecting farther than right occipital lobe – Right-handed individual with these patterns – Left-handed individual with left frontal petalias and right occipital petalias Left occipital petalia (a) Petalias Figure 13.15 Cerebrum: Cerebral Lateralization • Hemisphere specialization – Called cerebral lateralization – Higher order centers with different but complementary functions – Categorical hemisphere • • • • • specialized for language abilities usually contains Wernicke area and motor speech area involved in sequential and analytical reasoning tasks the left hemisphere in most people left-handed people with either hemisphere as categorical Cerebrum: Cerebral Lateralization • Hemisphere specialization – Representational hemisphere, other hemisphere • involved in visuospatial relationships • seat of imagination, artistic skill, pattern perception • right hemisphere in most people – Hemisphere in constant contact through commissures • especially corpus callosum – Develops prior to 5-6 years of age – Differs between sexes • women with a thicker posterior corpus callosum • adults with more lateralization – Correlated with handedness • right-handed and left-handed with different lateralization patterns • right-handed individuals usually with left categorical hemisphere • left-handed individuals with either categorical hemisphere Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Left eye Right eye Left Right visual visual field field Left Right visual visual field field Left hand Right hand Right hemisphere (representational hemisphere) Left hemisphere (categorical hemisphere) Figure 13.15b Verbal memory Memory for shapes (limited language comprehension) Corpus callosum Speech (motor speech area) Left hand motor control Right hand motor control Feeling shapes with left hand Feeling shapes with right hand Musical ability Recognition of faces and spatial relationships Superior language and mathematic comprehension (Wernicke area) Right visual field Left visual field Primary visual cortex (b) Cerebral lateralization Cerebrum Clinical View: Hemispherectomies and Cerebral Lateralization – Epilepsy • • • • • neurological disorder neurons transmitting action potentials too frequently and rapidly most controlled by medications may require surgical removal of part of brain in most severe cases, may require hemispherectomy – side of brain responsible for seizure activity removed • hemisphere able to take over some functions of missing hemisphere Cerebrum Clinical View: Cerebrovascular Accident – Cerebrovascular accident (CVA, or stroke) • • • • reduced blood supply to part of brain due to blocked arterial blood vessel or hemorrhage my cause brain tissue death if greater than 10 minutes symptoms of blurred vision, weakness, headache, dizziness, and walking difficulty • affect opposite side of body • brief episode, transient ischemic attack (TIA) Diencephalon • Diencephalon – Components of diencephalon: • epithalamus, thalamus, and hypothalamus – Provides the relay and switching centers for: • sensory and motor pathways • control of visceral activities Figure 13.17 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Corpus callosum Diencephalon Septum pellucidum Fornix Choroid plexus in third ventricle Thalamus Habenular nucleus Interthalamic adhesion Pineal gland Anterior commissure Posterior commissure Hypothalamus Tectal plate Frontal lobe Mammillary body Cerebral aqueduct Optic chiasm Infundibulum Cerebellum Pituitary gland Fourth ventricle Midsagittal section Epithalamus Diencephalon • Epithalamus – Partially forms posterior roof of diencephalon – Posterior portion • houses pineal gland - endocrine gland secreting melatonin • helps regulate day-night cycles, circadian rhythm • Thalamus • functions – Principal and final relay point for incoming sensory information – Processed and projected to primary somatosensory cortex – Information filter • e.g., “filters out” sounds in a busy cafeteria while you study Figure 13.18 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Medial group Interthalamic adhesion Lateral group (a ) Location of thalamus within brain Pulvinar nucleus Lateral geniculate nucleus Anterior group Ventral anterior Ventral lateral nucleus nucleus Ventral posterior nucleus Ventral group (b) Thalamus, superolateral view Posterior group Diencephalon Clinical View: Brain Disorders – Headache • due to dilated blood vessels in skull or muscle contraction • migraine headaches, very severe, affect one side of head • not true brain disorder, but may accompany them – Cerebral palsy • group of neuromuscular disorders • result from damage to infant brain before, during, or right after birth • impairment of skeletal muscle, sometimes mental retardation – Encephalitis • acute inflammatory disease of brain, usually due to virus • drowsiness, fever, headache, possibly coma and death Diencephalon Clinical View: Brain Disorders (continued) – Huntington disease • • • • hereditary disease affecting cerebral nuclei Rapid, jerky, involuntary movements also with intellectual deterioration fatal within 10 to 20 years after onset – Parkinson disease • affects muscle movement and balance • stiff posture, slow voluntary movements, resting tremor • caused by decreased dopamine production in substantia nigra Diencephalon: Hypothalamus • Hypothalamus – Infundibulum • thin stalk extending inferiorly from hypothalamus • attaches to pituitary gland • Functions of the hypothalamus – Master control of the autonomic nervous system • influences heart rate, blood pressure, digestive activities, and respiration • Hunger thirst – Regulation of sleep-wake rhythms • directs pineal gland to secrete melatonin • regulates circadian rhythms – Master control of the endocrine system • • • • oversees most of endocrine system secretes hormones that control activities in posterior pituitary gland produces antidiuretic hormone(water balance) and oxytocin(labor) Figure 13.19 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Paraventricular nucleus Dorsomedial nucleus Preoptic area Posterior nucleus Anterior nucleus Supraoptic nucleus Mammillary body Suprachiasmatic nucleus Ventromedial nucleus Arcuate nucleus Optic chiasm Infundibulum Posterior pituitary Anterior pituitary Sagittal section of hypothalamus Pituitary gland Brainstem • Brainstem – Connects cerebrum, diencephalon, and cerebellum to spinal cord – Bidirectional passageway – Contains many autonomic centers and reflex centers – Houses nuclei of many cranial nerves – From superior to inferior: • midbrain • pons • medulla oblongata Brainstem: Midbrain • Components of midbrain • houses neurons producing dopamine – involved in movement, emotions, pleasure and pain response • pathology here in Parkinson disease - integrates information from cerebrum and cerebellum • issues involuntary motor commands to erector spinae – helps maintain posture Brainstem: Pons • Components of pons – Bulging region on anterior brainstem – Sensory and motor tracts located here • connect to brain and spinal cord – respiratory center • helps regulate skeletal muscles of breathing – Cranial nerve nuclei • sensory and motor nuclei for: – trigeminal, abducens, facial, and vestibulocochlear nerves Brainstem: Medulla Oblongata • Medulla oblongata – Most caudal part of the brainstem – Continuous with spinal cord inferiorly – All tracts between brain and spinal cord passing through here – Pyramids • most cross to opposite side of brain • cerebral hemisphere controlling movement on opposite side Brainstem: Medulla Oblongata • Autonomic nuclei of medulla – Cardiac center • regulates heart’s rate and strength of contraction – Vasomotor center • • • • controls blood pressure alters diameters of arterioles increased blood pressure when vessels constrict decreased bp when vessels relax – Medullar respiratory center • regulates respiratory rate • influenced by pontine respiratory center – Other nuclei in the medulla • involved in coughing, sneezing, and salivation • swallowing, gagging, and vomiting Cerebellum • Cerebellum – Second largest part of the brain – Produces fine control over muscular actions – Helps maintain equilibrium and posture – Stores memories of movement patterns • e.g., playing scales on a piano – Partitioned into three regions: • cerebellar cortex, outer gray matter of cortex • internal region of white matter, arbor vitae • deepest gray matter layer of cerebellar nuclei Figure 13.25 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Primary motor cortex Voluntary movements The primary motor cortex and the basal nuclei in the forebrain send impulses through the nuclei of the pons to the cerebellum. Cerebral hemisphere Assessment of voluntary movements Proprioceptors in skeletal muscles and joints report degree of movement to the cerebellum. Integration and analysis The cerebellum compares the planned movements (motor signals) against the results of the actual movements (sensory signals). Corrective feedback The cerebellum sends impulses through the thalamus to the primary motor cortex and to motor nuclei in the brainstem. Thalamus Cerebellar cortex Corpus callosum Pontine nucleus Pons Direct (pyramidal) pathway Sagittal section Cerebellum: Functions Clinical View: Effects of Alcohol and Drugs on the Cerebellum – Variety of drugs impairing cerebellar function • include alcohol • leads to: – disturbance of gait – loss of balance and posture – inability to detect proprioceptive information Functional Brain Systems: Limbic System • Limbic system – – – – Composed of multiple cerebral and diencephalic structures Collectively process and experience emotions Structures forming a ring around the diencephalon Hippocampus • nucleus superior to parahippocampal gyrus • assists in storing memories and forming long-term memory • connects to diencephalon – Amygdaloid body • connects to the hippocampus • involved in several aspects of emotion, especially fear • can help store emotions depending on emotional context – Olfactory bulbs, olfactory tracts, olfactory cortex • process odors that can provoke emotions – Fornix • thin tract of white matter • connects hippocampus with other limbic structures Figure 13.26 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Components of the limbic system Cingulate gyrus Corpus callosum Fornix Anterior thalamic nucleus Anterior commissure Septal nucleus Mammillary body Hippocampus Amygdaloid body Parahippocampal gyrus Olfactory tract Olfactory bulb Midsagittal section Functional Brain Systems: Limbic System What are the main functions of the limbic system? The limbic system is involved with processing and experiencing emotions. Functional Brain Systems: Clinical View: Pathologic States of Unconsciousness – Fainting • brief loss of consciousness • often signals inadequate cerebral blood flow due to low blood pressure – Stupor • arousable only to extreme stimuli • with metabolic disorders, liver or kidney disease, brain trauma, or drugs – Coma • deep and profound unconsciousness alive but unable to respond • from severe head injury, metabolic failure, very low blood sugar, or drugs – Persistent vegetative state • person without thinking and awareness of environment • continuation of noncognitive brain functions some spontaneous movements possible – Electroencephalogram (EEG) • diagnotic test where electrical activity of the brain is measured • plots different types of brain waves – waves varying with age, sleep, seizure, or pathology Integrative Functions and Higher-Order Brain Functions • Higher-order mental functions – – – – Include learning, memory, and reasoning Occur within the cortex of cerebrum Involve multiple brain regions Both conscious and unconscious processing involved • Cognition – Mental processes • e.g., awareness, knowledge, memory, perception, and thinking – Association areas of the cerebrum responsible • process and integrate information between sensory and motor areas Integrative Functions and Higher-Order Brain Functions: Memory • Memory – Requires higher-order mental functions – Depends on complex interactions among brain regions • Types of memory: – sensory memory • form important association based on sensory input • lasts for seconds – short-term memory (STM) • limited capacity (about seven small pieces of information) • brief duration (seconds to hours) – long-term memory (LTM) • can be converted from short-term memory if information repeated – termed encoding • may exist for limitless periods of time • needs to be retrieved occasionally or can be “lost Integrative Functions and Higher-Order Brain Functions: Memory Clinical View—Alzheimer Disease: The “Long Goodbye” – – – – – – – – Leading cause of dementia in developed world Slow, progressive loss of higher intellectual function Usually starts after age 65 Changes in mood and behavior Eventual loss of memory and personality Underlying cause unknown No cure, some medications to help slow course Identifiable with positron emission tomography (PET) Integrative Functions and Higher-Order Brain Functions: Memory Clinical View: Amnesia – Partial or complete loss of memory – Usually temporary and affecting only a portion of experiences – Causes: • psychological trauma • direct brain injury – Type and degree of recovery • depends on part of the brain damaged – Most serious kind • results from damage to thalamus and limbic structures, especially hippocampus Integrative Functions and Higher-Order Brain Functions: Emotion • Brain regions involved in emotion – Emotions interpreted by limbic system – Expression controlled by prefrontal cortex • decides appropriate way to show feelings – Amygdaloid body and hippocampus important structures • if damaged or artificially stimulated, get deadened or exaggerated emotions • Brain regions involved in language – Includes functions of reading, writing, speaking, and understanding – Wernicke area • involved in interpreting writing and oral language • in the categorical hemisphere in most people Integrative Functions and Higher-Order Brain Functions: Language • Brain regions involved in language (continued) – Broca area, motor speech area • receive axons from Wernicke area • regulates motor activities needed for speech • sends signals to primary motor cortex – innervate muscles of cheeks, larynx, lips, and tongue – Angular gyrus • posterior to Wernicke area • processes words read into speakable form – Region opposite Wernicke area in representational hemisphere • recognizes the emotional content of speech – Region opposite motor speech area in representational hemisphere • responsible for producing speech with emotion • lesion producing aprosodia, dull emotionless speech Figure 13.29 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Primary motor cortex Motor speech area Wernicke area (a) Lateral view 1 Auditory information about a sentence travels to the primary auditory cortex. The Wernicke area then interprets the sentence. (b) PET scans 2 Information from the Wernicke area travels to the motor speech area. 3 Information travels from the motor speech area to the primary motor cortex, where motor commands involving muscles used for speech are given. (left): © Wellcome Dept. of Cognitive Neurology/Photo Researchers, Inc.; (center): © WDCN/Univ. College London/Photo Researchers, Inc.; (right): © Scientifica/ADEAR/Visuals Unlimited Integrative Functions and Higher-Order Brain Functions: Language Clinical View: Dyslexia – – – – – – Inherited learning disability Problems with single-word decoding Individuals with trouble reading, writing, and spelling Level of reading competence below expected intelligence Improvement in some individuals with time May be form of disconnect syndrome • impaired transfer of information through corpus callosum Cranial Nerves • Cranial nerves – Part of the peripheral nervous system – Originate on inferior surface of brain – Numbered with Roman numerals according to their position • begin with most anteriorly placed nerve – Name related to function On Old Olympus' Towering Top, A Finn And German Viewed Some Hops Oh, Oh, Oh, To Touch And Feel Virgin Girl's Vagina And Hymen Some Say Marry Money, But My Brother Says Big Breasts Matter Most • Cranial nerves – Olfactory nerve (CNI) • olfaction – Optic nerve (CNII) • vision – Oculomotor (CNIII) • four extrinsic eye muscles • elevates eyelid, constricts pupils, rounds lens of eye – Trochlear nerve (CNIV) • superior oblique eye muscle – Trigeminal nerve (CNV) • sensory from anterior scalp, face, oral cavity, and others • muscles of mastication and others – Abducens (CNVI) • lateral rectus eye muscle – Facial nerve (CNVII) • taste anterior tongue, muscles of facial expression, others • gland secretions from lacrimal, submandibular, and salivary glands • Cranial nerves – Vestibulocochlear nerve (CNVIII) • hearing, equilibrium – Glossopharnygeal (CNIX) • sensory and taste to posterior tongue • sensory to part of pharynx and others • secretions from parotid gland – Vagus nerve (CNX) • • • • visceral sensory from heart, lungs, and abdominal organs general sensory from part of pharynx, larynx, others most pharyngeal and all laryngeal muscles smooth muscles and glands of heart, lungs, larynx, and most abdominal organs – Accessory nerve (CNXI) • trapezius and sternocleidomastoid muscle – Hypoglossal (CNXII) • intrinsic and extrinsic tongue muscles Figure 13.30 Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Cranial nerves Olfactory bulb, termination of olfactory nerve (CN I) Olfactory tract Optic chiasm Optic nerve (CN II) Infundibulum Optic tract Oculomotor nerve (CN III) Trochlear nerve (CN IV) Pons Trigeminal nerve (CN V) Pons Abducens nerve (CN VI) Facial nerve (CN VII) Vestibulocochlear nerve (CN VIII) Medulla oblongata Glossopharyngeal nerve (CN IX) Vagus nerve (CN X) Accessory nerve (CN XI) Hypoglossal nerve (CN XII) Spinal cord (right): © The McGraw-Hill Companies, Inc./Rebecca Gray, photographer Medulla oblongata I. Olfactory Nerve • Function: Sense of smell • Composition: Sensory • Clinical Test: Determine whether subject can smell aromatic substances – Coffee, vanilla, clove, oil, soap • Effect of Damage: impaired sense of smell II. Optic Nerve • Function: Vision • Composition: Sensory • Clinical Test: Test peripheral vision and visual acuity • Effect of Damage: Blindness in part or all of visual field III. Oculomotor Nerve • Functions: Controls muscles that turn eyeballs up, down, medially – Controls iris, lens, and upper lid • Composition: Motor • Clinical Test: Look for pupil shape differences – Test pupillary response to light – Test ability to track moving objects • Effect of Damage: Drooping eyelid, dilated pupil, inability to move eye in some directions, double vision, difficulty focusing IV. Trochlear Nerve • Function: Controls a muscle that rotates eyeball medially • Composition: Motor • Clinical Test: Test ability of eye to rotate inferolaterally • Effect of Damage: double vision, inability to rotate eye inferolaterally V. Trigeminal Nerve • Function: Important in facial sensations • Composition: Both • Clinical Test: Test facial sensation of forehead, cheeks, and chin. – Test subjects ability to open mouth against resistance • Effect of Damage: Loss of sensation from face and impaired chewing VI. Abducens Nerve • Function: Controls a muscle that turns eyeball laterally • Composition: Motor • Clinical Test: Test lateral eye movement • Effect of Damage: Inability to turn eye laterally, at rest eye will turn medially VII. Facial Nerve • Function: Important nerve of facial muscles and taste • Composition: Both • Clinical Test: Test tongue for taste response, test ability to make facial expressions • Effect of Damage: inability to control facial muscles, sagging due to loss of muscle tone, distorted sense of taste VIII. Vestibocochlear Nerve • Function: Hearing and equilibrium • Composition: Sensory • Clinical Test: Look for nystagmus, test hearing, balance, ability to walk in a straight line • Effect of Damage: deafness, dizziness, nausea, loss of balance, nystagmus IX. Glossopharyngeal Nerve • Function: Food ingestion, salivation – Sensations from the tongue, throat, and outer ear • Composition: Both • Clinical Test: Test gag reflex, swallowing, and coughing • Effect of Damage: impaired swallowing X. Vagus Nerve • Function: Control of cardiac, pulmonary, digestive, and urinary functions • Composition: Both • Clinical Test: Speech abnormalities, swallowing abnormalities, absence of gag reflex, weak or hoarse voice, inability to cough • Effect of Damage: Hoarseness or loss of voice, impaired swallowing XI. Accessory Nerve • Function: Controls swallowing and neck and shoulder muscles • Composition: Motor • Clinical Test: Test ability to rotate head and shrug shoulders against resistance • Effect of Damage: impaired movement of head, neck, and shoulders, difficulty shrugging shoulder on damaged side XII. Hypoglossal Nerve • Function: Controls tongue movements • Composition: Motor • Clinical Test: Note deviations of the tongue as subject protrudes and retracts it • Effect of Damage: impaired speech and swallowing, inability to protrude tongue if both sides damaged, deviation of tongue toward injured side