GKthesis finalversion
advertisement

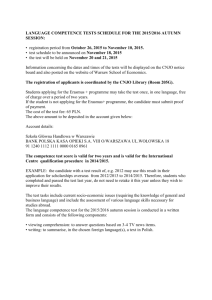
Running Head: NEGATIVE LIFE EVENTS The Relation of Negative Life Events to Symptoms and Functioning in Adolescents and Young Adults with a Childhood History of Chronic Abdominal Pain Gerianna Kneeland Honors Psychology Honors Thesis April 7, 2010 NEGATIVE LIFE EVENTS 2 Prevalence and Incidence of Chronic Abdominal Pain Chronic abdominal pain (CAP) is considered the most common form of pain complaint across childhood. According to the American Academy of Pediatrics (2005), between 2-4% of all pediatric clinic visits are related to chronic abdominal pain. Chronic abdominal pain affects an estimate of 10-15% of school-aged children (Walker and Greene, 1991). Chronic abdominal pain usually occurs in the age range of 5-16 years, with particularly high incidence between 8-12 years of age. It is uncommon for chronic abdominal pain to affect children under the age of 5. Although the onset of chronic abdominal pain is during childhood, some children continue to suffer from this condition into adolescence and eventually, adulthood (Garber, Smith, Van Slyke, Lewis Claar, and Walker, 2001; Kristjansdottir, 1997). Background and Significance of Problem Chronic abdominal pain is defined as “intermittent or constant abdominal pain of at least 3 months’ duration” (American Academy of Pediatrics, 2005). It is common for chronic abdominal pain to begin during childhood, and increase during the period of adolescence. In the stage of adolescence, chronic abdominal pain is more common in girls than boys. Chronic abdominal pain may be associated with anxiety, symptoms of depression, depressive disorders, absence from school, family disruption, and various somatic symptoms (Apley, 1975; Walker, Garber, and Greene, 1993; Garber et al., 2001). One of the major issues in the literature has been the defining criteria for chronic abdominal pain. For many years, “recurrent abdominal pain” was the term used in referring to persistent complaints of abdominal pain. Recurrent abdominal pain was NEGATIVE LIFE EVENTS 3 originally defined by Apley in the 1950s as 3 or more episodes of abdominal pain, which last for a period equivalent to 3 months or more. Apley’s research definition of recurrent abdominal pain was used as the criteria for selecting subjects for many studies and eventually came to be used clinically as a diagnosis for all children who have abdominal pain without an organic etiology. Because of the inappropriate use of the term, “recurrent abdominal pain” as a diagnosis, it has been replaced with the term “chronic abdominal pain” which is regarded as a symptom description. This term “recurrent abdominal pain” is no longer recommended for use in clinical practices (American Academy of Pediatrics, 2005; Walker and Greene, 1991a). Psychosocial factors and the effect on chronic abdominal pain Psychosocial factors have been found to influence some cases of somatic complaints in children with chronic abdominal pain. These forms of somatic complaints have been to linked to somatization, defined as “the tendency to express emotional distress in the form of somatic complaints” (Garber et al., 2001). According to Walker and Greene (1991a), many researchers have hypothesized that psychosocial factors influence illness in chronic abdominal pain patients. Most of these studies of chronic abdominal pain have examined stressors like school issues, illness or death of family members, and family disruption (as cited in Stone and Barbero, 1970). The most prominent psychosocial factors investigated in relation to CAP include child academic and social competence, parental somatic complaints, modeling of illness behavior, and negative life events (Walker et al., 1993; Walker et al., 1994). NEGATIVE LIFE EVENTS 4 Lack of competence is a psychosocial factor that may be linked with CAP as well as various childhood emotional disorders (Blechman, Tinsley, Carella, and McEnroe, 1985). A study by Cole and Lejune (1972) found evidence that people who distinguish themselves as being incapable of performing certain activities may take on a sick role as a means of coping with their academic and social difficulties. This study suggests the possibility that low academic and social competence might contribute to child somatic complaints and disability. Children with chronic abdominal pain who have poor social competence are likely to exhibit more disability than children with CAP who have good peer relationships (Claar, Walker, and Smith, 1999; Robinson, Alvarez, & Dodge, 1990). Parent somatic complaints have been linked to child somatic complaints, specifically complaints of chronic pain and stress-related symptoms. One of the proposed reasons for this relationship is that parents and children can have similar inclinations for responding to stress (Walker et al., 1994). Besides parent somatic complaints, parental dysfunction and emotional stress are characterized with the increased use of pediatric health services (Roghmann, and Haggerty, 1973). Another reason for the link between parent and child symptoms is that parents’ pain behavior may be behavioral modeling for the child (Walker et al, 1993). For example, Walker et al. (1993) noted that studies have recently found that unexplained or regular occurrences of child pain complaints are more likely to occur when other family members complain of pain (as cited in Osborne, Hatcher, and Richtsmeier, 1989). One of the most important psychosocial factors related to child somatic complaints are negative life events, or life stress. Apley (1975) believed that episodes of NEGATIVE LIFE EVENTS 5 pain are generally preceded by stressful events and followed with symptoms of emotional distress. Apley (1975) also believed that many stressful situations occur in a child’s life which may lead to outcomes such as acute physical illness, functional complaints, and emotional disorders. According to Walker et al. (1994), samples taken from different communities have found that higher levels of life stress are connected with more frequent episodes of illness (as cited in Beautrais, Ferguson, and Shannon, 1982). A study by Robinson et al. (1990) found that there is a relationship between stressful life events and the onset of abdominal pain symptoms in chronic pain patients. Some research even suggests that a family member can indirectly affect other members of the family by the stressful life events they experience (Walker et al., 1993, Walker et al., 1994). Several studies examine negative life events and other psychosocial factors in pediatric patients evaluated for chronic abdominal pain in medical settings. Studies that examined the role of psychosocial factors were conducted by Walker et al. in 1993 and 1994. In the study carried out in 1993, Walker et al. compared chronic abdominal pain patients to patients with organic illness, patients with psychiatric diagnoses, and well children in regard to factors including competence, negative life events, family functioning, family illness, emotional and somatic symptomatology, and encouragement of illness behavior. In relation to negative life events, Walker et al. (1993) found that chronic abdominal pain patients reported less negative life events than did the psychiatric patients and about the same number of reports as the well children. The study also found that chronic pain patients did not report more occurrences of health-related life events NEGATIVE LIFE EVENTS 6 than the other two groups. These findings suggest that negative life events alone cannot bring about symptoms in pain patients. Another study by Walker et al. (1994) carries the previous study further by examining the role of negative family life events in chronic abdominal patients and three possible moderator variables: child academic and social competence, gender, and parental somatic complaints. Results from this study indicate that for children with low levels of social competence, higher levels of negative life events were associated with more somatic complaints. In children with high social competence there was no association between life events and somatic complaints. Parental somatic symptoms also influenced child somatic complaints. For children whose fathers reported higher levels of somatic complaints, the child was also found to report higher levels of somatic complaints. However, a difference was found in the effect of maternal symptoms on boys and girls. Results found that boys report more somatic complaints when their mothers report higher levels of somatic symptoms in response to negative life events. Maternal somatic symptoms did no influence girls’ somatic symptoms. These findings suggest that the higher the levels of parental somatic symptoms and family life events, the higher the level of somatic complaints from children. The effect of negative life events on Functional disability Negative life events are not only associated with somatic complaints, but also with functional disability in pain patients. Functional disability is defined as “limitations in a person’s ability to perform activities relevant to daily life including physical, social, and personal activities” (Palermo, Long, Lewandowski, Drotar, Quittner, and Walker, NEGATIVE LIFE EVENTS 7 2008). According to Walker and Greene (1991b), there are many possible uses for measuring functional disability, including the examination of the course of trauma or disease on the child’s daily functioning, describing changes in the child’s daily functioning following intervention, and examining differences in individual patient’s functioning within certain patient groups. Walker and Greene (1991b) also noted different measures for assessing functional disability including the Functional Disability Inventory, questionnaires, activities of daily living scales, and instruments that examine the patient’s total functional profile. Limitations of current knowledge The current body of knowledge on pain and disability that life stress places on chronic abdominal pain patients is not without limitations. Generally, life stress has been measured with questionnaires that assess negative life events during the previous year. This approach poses several limitations for the study of chronic abdominal pain. Most importantly, negative life events occur at different time intervals throughout the period of a year, while episodes of chronic abdominal pain could occur across the span of a day and possibly be preceded by small daily stressors that aren’t included in measures of negative life events. Also, children’s circumstances can change over the course of a year, which would affect the relationship of stress and illness in unpredictable ways. Although life stress is suggested to influence the severity of somatic complaints in chronic abdominal pain patients, it does not affect each child in the same way. Previous research has looked at the possibility of competence as a resource that may buffer individuals from the negative effects of life stress. For example, Compas and Phares (1991) suggested that higher levels of competence would buffer children from the NEGATIVE LIFE EVENTS 8 negative outcomes of life stress (as cited in Walker, Garber, and Greene, 1994). This hypothesis was tested by Walker, Garber, and Greene (1994) and results showed that among children who reported lower levels of social competence, higher levels of negative life events were related to more somatic complaints at follow-up. On the contrary, among children with high levels of social competence, life events and the amount of somatic complaints were not correlated. The measures used to assess functional disability have limitations as well. First, there are various ways to measure a patient’s level of functional disability, such as questionnaires and records of school absence. However, some studies may only consider one measure of functional disability when examining patients. Another limitation is that some of the measures for functional disability, for example questionnaires, could be very general without going into detail about the disability of the patient. Topic: This study will examine the impact of life stress and perceived competence on symptoms, emotions, and functioning in adolescents and young adults who had chronic abdominal pain when they were children. Data analysis will test two hypotheses: (1) higher levels of personal life stress will be associated with poorer patient outcomes at follow-up including more emotional symptoms, somatic symptoms, and disability; and (2) personal competence will moderate the effect of life stress on patient outcomes, such that life stress will be associated with poorer outcomes in patients with low competence compared to those with high competence. Participants: Participants were recruited from the research database containing 850 patients who were participants in a research protocol when they were evaluated for chronic abdominal pain at the Vanderbilt Pediatric Gastroenterology Clinic during the NEGATIVE LIFE EVENTS 9 period from 1993 to 2007.They were invited to participate in a follow-up assessment during the period 2006-2009. The participants were between the ages of 12 and 32 years during 2006 through 2009 after they had completed the follow-up assessment. Participants’ telephone numbers, addresses, and permission for additional contact were obtained from the participants at the time of study entry. Measures for this study 1. Life Events Questionnaire The Life Events Questionnaire (LEQ) assesses negative life events in the past year. This questionnaire includes both distinct life events and chronic stressors that were experienced by the child over the course of the year. Participants are asked to indicate which events occurred and the total scores equal the sum of the events (Walker, Garber, & Greene, 1993, cited in Masten et al., 1988). 2. SF-36 Health Survey The SF-36 Health Survey assesses functioning and emotions of participants. It is a multi-purpose, short form health survey composed of only 36 questions. It yields an 8scale profile of functional health and well-being scores as well as psychometrically-based physical and mental health summary measures. The SF-36 is a generic measure, in that it does not target a specific age, treatment group, or disease. It has proven to be beneficial in surveys including general and specific populations, comparing the burden of diseases, and differentiating the health benefits produced by a number of different treatments (Ware, Snow, Kosinski, & Gandek, 1993). 3. Child/adult Somatization Inventory (CSI) NEGATIVE LIFE EVENTS 10 The Child Somatization Inventory assesses the severity of nonspecific somatic symptoms most commonly reported by children with recurrent abdominal pain. The CSI includes symptoms from the revised 3rd edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III-R) and from the somatization factor of the Hopkins Symptom Checklist. Examples of items from the CSI included “headaches,” “feeling low in energy”, and “faintness or dizziness”. Respondents are asked to rate the extent to which they have experienced each of the 35 symptoms in the last 2 weeks using a 5-point scale ranging from not at all (0) to a whole lot (4). The total score from the CSI can range from 0 to 140. The CSI reports a three-month test-retest Pearson reliability was reported as .50 for well patients and .66 for chronic pain patients (Walker, Garber, & Greene, 1993, cited in Garber, Walker, and Zeman, 1991). 4. Functional Disability Inventory The Functional Disability Inventory assesses the extent to which functional disability, defined as “difficulty in physical and psychosocial functioning due to physical health status,” limits the child in different activities. The FDI consists of 15 items referring to the child’s disability in the past 2 weeks. It includes activities in the domains of school, home, recreation, and social interaction. The participant rates how difficult it was for him or her to perform each activity in the past few days along a 5-point severity scale, ranging from 1 (no trouble) to 5 (impossible). Sample activities include walking to the bathroom, being at school all day, reading or doing homework, and running the length of a football field. The FDI was found to have a 3-month test-retest reliability that is higher than .60 for chronic pain patients. (FDI; Walker & Greene, 1991). 5. Self-Perception Profile for Adolescents/Adults NEGATIVE LIFE EVENTS 11 The Self-Perception Profile (SPP) for Adolescents/Adults (Harter, 1985) assesses perceived global and domain-specific competence. For this study we administered the scale for global self-worth. The global self-worth scale has 6 items. The SPPC has a response format that ranges from 1 to 4. Children note the extent to which each of the items is “true” or “not true” for them. Harter reported acceptable levels of internal consistency and convergent validity for the SPPC. The SPPC was found to have a testretest reliability of .826. Procedure: In order to recruit for the study, former research participants were sent a letter introducing the study. A stamped postcard addressed to Vanderbilt was enclosed indicating that the recipient may “opt-out” of the study by returning the card. If the card was not returned within 10 days, participants received a recruitment phone call. In this call, participants (or their parents if they are younger than 18) were given details about the study and what their participation would entail. During this phone call, participant eligibility for the study was also assessed. If participants were eligible, they were invited to participate in the study. For participants who were between the ages of 12 and 17, consent was obtained from the parent. If the parent gave verbal consent to participate and to allow their son/daughter to participate, the researcher described the study to the youth and obtained their verbal assent to participate. At the end of the call, Telephone Interview #1 was scheduled with participants (and their parents if they were younger than 18). Participants who could not come to Vanderbilt to complete the full protocol had the opportunity to consent to the abbreviated protocol that entails Telephone Interview #1, Telephone Interview #2, and Online Surveys, but does not include the laboratory protocol. NEGATIVE LIFE EVENTS 12 Telephone Interview #1 Telephone Interview #1 consisted of questions regarding the participant’s use of health care services and physical symptoms they had experienced in the past year (for participants under the age of 18, parents answered the questions about health care system use). The time required for Interview #1 varied from person to person because some people experienced many of the symptoms they are asked about and some participants only experienced a few of the symptoms. The time required for telephone interview #1 ranged from 35 to 65 minutes. Telephone Interview #2 Telephone Interview #2 consisted of the Anxiety Disorders Interview Schedule (ADIS). [Participants who completed the full protocol completed the ADIS at Vanderbilt and did not participate in Telephone Interview #2]. During Telephone Interview #2, trained research assistants asked questions about the participants’ emotional health. Participants who were 19 completed the adult version of the ADIS. Participants who were under 18 completed the youth version of the ADIS and their parent completed the parentreport version of the ADIS in a separate telephone interview that was scheduled with the parent. The time required for Interview #2 ranged from 40 to 60 minutes. Online surveys The Online survey consisted of several questionnaires. These questionnaires included the McGill Pain Questionnaire, State-Trait Inventory, Center for Epidemiological Studies-Depression Scale, Pain Beliefs Questionnaire, NEO Personality Inventory, Self-Perception Profile, Life Events Questionnaire, and the Anger Expressiveness Inventory. NEGATIVE LIFE EVENTS 13 Data analysis Data analysis tests two hypotheses: (1) higher levels of personal life stress (assessed by the LEQ) is associated with poorer patient outcomes at follow-up including more emotional symptoms (SF-36), somatic symptoms (CSI), and disability (FDI); and (2) personal competence (SPP) moderates the effect of life stress on patient outcomes, such that life stress is associated with poorer outcomes in patients with low competence compared to those with high competence. Results Table 1 lists the Demographic characteristics of the sample from the study. There were a total of 218 participants, ranging from 12-32 years of age. The range of scores on the Hollingshead Index was from 9-69, indicating that participants ranged from unskilled workers to professionals. Regarding gender, 57.8% of the participants in the study were females, and 41.7% were males. In this study, 90.8% of the participants were Caucasian, and 7.8% of the participants were categorized as “other”. Table 2 presents the correlations among study variables (see end notes). Effect of life stress and competence and their interaction on SF-36 scores, controlling for age and gender Table 3 shows results of a multiple regression analysis examining the effect of life stress and competence and their interaction on the SF-36. Gender was a significant control variable, with a significant p-value of .042 and a of .149, showing that males had higher SF-36 scores (better health) than females. Life events (LEQ) scores also were significantly associated with the SF-36, with a p-value of .001 and a score of -.292, thus illustrating that higher life events were associated with lower SF-36 scores (poorer NEGATIVE LIFE EVENTS 14 health), and low life events were associated with higher SF-36 scores (better health). Social competence was also significantly associated with the SF-36. We reported a pvalue 0f .001 and a of .442. This demonstrated that higher levels of social competence were associated with higher SF-36 scores. Effect of life stress and competence and their interaction on CSI scores, controlling for age and gender Table 4 illustrates the effects of life stress, competence, and their interaction on the CSI. Both age and gender were significantly associated with CSI scores; females and older participants had higher CSI scores. The predictor variables, life events (LEQ) and social competence were significantly associated with CSI scores as well. We reported a p-value of .007 and a score of .188 for the effect of life events on CSI scores. These results illustrate that higher levels of life stress were associated with higher CSI scores. For social competence, we reported a p-value of .010 and a of -.176, indicating that higher levels of competence were associated with lower CSI scores. We also looked at the two-way interaction between life events and social competence on CSI scores and found that this interaction was significant. We reported a p-value of .035 and a of -.670 for this interaction effect. Figure 1 provides a graphical representation of the two-way interaction effect of life stress and social competence on the CSI. For participants with high social competence, CSI scores were low regardless of their level of stress. In contrast, for those with low social competence, higher levels of stress were associated with higher CSI scores. Effect of life stress, competence, and their interaction on FDI scores, controlling for age and gender NEGATIVE LIFE EVENTS 15 Table 5 shows the results of multiple regression analysis examining the effects of life stress and competence on FDI scores. The control variables, age and gender, were both significantly associated with FDI scores. We reported a p-value of .000 and a score of .261 for the relationship between age and FDI scores, indicating that older children reported more disability than younger children. For the association of gender with FDI scores, we reported a p-value of .002 and a score of -.214, showing that females had higher FDI scores than males. Social competence was also significantly associated with FDI scores. We reported a p-value of .000 and a score of -.254, showing that higher social competence was associated with lower FDI scores. Discussion Results of this study provided support for our hypothesis that higher levels of life stress are associated with more somatic symptoms, emotional symptoms, and disability in individuals with a history of CAP. These results imply that negative life events are associated with several aspects of poor health. In our second hypothesis, we looked further to determine whether competence could serve as a moderator of the effect of life stress on patient health. We found support for this hypothesis with respect to CSI scores but not FDI or SF-36 scores. Specifically, participants with high social competence had lower CSI scores regardless of whether they had low or high stress levels. In contrast, participants with low social competence and high stress levels had higher CSI scores than those with low social competence and low stress levels. This finding suggests implications that life stress does not have a universal effect on individuals; the effect of stress on somatic symptoms (CSI) is stronger for those with low social competence. This may be because individuals with low social competence have less support for dealing NEGATIVE LIFE EVENTS 16 with life stress. However, because our data are cross-sectional, we cannot rule out the possibility that low social competence contributes to life stress. For example, people with low social competence might not be skilled at managing relationships with their boss or co-workers, which could create stress in their workplace. In addition, there could be other factors not examined in this study that potentially influence the extent to which high stress levels can have a negative effect on health,. Other factors such as socio-economic status, peer pressure, the pressure to perform academically, and community safety could play a role in how stress affects health. This study had several limitations that should be considered in interpreting our results. First, competence is a self-report measure. The SPP assesses the extent to which individuals report whether the items are “true” or “not true”. This poses a problem because individuals may not be able to accurately give reliable reports of their level of competence. They could over- or under-estimate the amount of competence they possess. Second, this was a cross-sectional study, which limits potential conclusions we may be able to draw regarding causality. Since this study was cross-sectional, we assessed the participant’s negative life events and health at the same time. For this reason, we do not know the extent to which life events influenced health or health influence life events. Third, we assessed life events for the year preceding the interview. People’s personal situations can change significantly over the course of year, which may affect the relationship that stress has on illness in variable ways. It is also possible that life events may not be the actual trigger for symptoms. It could be possible that there are other contributing events that could influence, or trigger these symptoms before the negative life event occurs. NEGATIVE LIFE EVENTS 17 Based on our findings, future studies should now look towards considering other factors that could potentially moderate levels of stress. These studies could consider issues such as socio-economic status, access to health care, educational background, and community awareness and safety. These aforementioned issues can help account for the third-variable problem such that all factors that could influence stress are considered in the data analysis. Also, future studies should have prospective designs. Prospective studies will allow researchers to keep track of changes in participants’ life stress and health over time, allowing better understanding of how stress and health may influence each other. NEGATIVE LIFE EVENTS 18 “References” Apley, J. (1975). The child with abdominal pains. London: Blackwell. Beautrais, A., Ferguson, D., & Shannon, F. (1982). Life events and childhood morbitdity: A prospective study. Pediatrics, 70, 935-940. Blechman, E. A., Tinsley, B., Carella, E. T., & McEnroe, M. J. (1985). Childhood competence and behavior problems. Journal of Abnormal Psychology, 94, 70-77. Claar, R., Walker, L., Smith, C. (1999). Functional disability in adolescents and young adults with symptoms of irritable bowel syndrome: the role of academic, social, and athletic competence. Journal of Pediatric Psychology, 24, 271-280. Cole, S., and Lejune, R. (1972). Illness and the legitimation of failure. American Sociological Review, 37, 347-356. Greene, J. W., Walker, L. S.. Hickson, G.. & Thompson, J. (1985). Stressful life events and somatic complaints in adolescents. Pediatrics. 75, 19-22. Guite, J. W., Lobato, D. J., Shalon, L., Plante, W., & Kao, B. T. (2007). Pain, disability, with functional and symptoms among siblings of children abdominal pain. Journal of Developmental and Behavioral Pediatrics, 28(1), 2-8. Kristjansdottir, G. (1997). Prevalence of pain combinations and overall pain: a study of headache, stomach pain and back pain among school-children. Scandinavian journal of social medicine, 25, 58-63 Mulvaney, S., PhD., Warren Lambert, E., PhD., Garber, J. PhD., & Walker, L. S., PhD. (2006). Trajectories of Symptoms Impairment for Pediatric Patients With Functional Abdominal Pain: A 5-Year Longitudinal Study. Child Adolescent Psychiatry, 45(6), 737-744. Osborne, R. B., Hatcher, J. W., and Richtsmeier, A. J. (1989). The role of social modeling in unexplained pediatric pain. Journal of Pediatric Psychology, 14, 4361. Palermo, T. M., PhD, Long, A. C., PhD, Lewandowski, A. S., MA, Drotar, D., PhD, Quittner, A. L., PhD, & Walker, L. S., PhD (2008). Evidence-based assessment of health-related quality of life and Functional impairment in Pediatric Psychology. Journal of Pediatric Psychology, 33(9), 983-996. Retrieved 2008, December 6 from American Academy of Pediatrics Web site: http://www.aap.org/healthtopics/stages.cfm#middle Robinson, J. O., Alvarez, J. H., & Dodge, J. A. (1990). Life events and family history in NEGATIVE LIFE EVENTS 19 children with recurrent abdominal pain. Journal of Psychosomatic Research, 34, 171-181. Rogers, K. D., and Reese, G. (1965). Health studies—presumably normal high school students: 3 Health room visits. American Journal of Diseases of Children, 109, 28-42. Roghmann, K. J., and Haggerty, R. J. (1973). Daily stress, illness, and use of health services in young families. Pediatric Research, 7, 520-526. Stone. R., & Barbero, G. (1970). Recurrent abdominal pain in childhood. Pediatrics. 45. 732-738. Walker, L. S., Garber, J., Smith, C. A., Van Slyke, D. A., & Claar, R. L. (2001). The relation of daily stressors to somatic and emotional symptoms in children with and without recurrent abdominal pain. Journal of Consulting and Clinical Psychology, 69(1), 85-91. Walker, L. S., Garber, J., & Greene, J. W. (1993). Psychosocial correlates of recurrent childhood pain: A comparison of pediatric patients With recurrent abdominal pain, organic illness, and psychiatric disorders. Journal of Abnormal Psychology, 102(2), 248-258. Walker, L. S., Garber, J., & Greene, J. W. (1994). Somatic complaints in pediatric patients: A prospective study of the role of negative life events, child social and academic competence, and parental somatic symptoms. Journal of Consulting and Clinical Psychology, 62(6), 1213-1221. Walker, L. S., and Greene, J. W. (1991a). Negative life events and symptom resolution in pediatric abdominal pain patients. Journal of Pediatric Psychology, 16(3), 341360. Walker, L. S., & Greene, J. W. (1991b). The Functional Disability Inventory: measuring a neglected dimension of child health status. Journal of Pediatric Psychology, 16(1), 39-58. Ware, JE, Snow KK, Kosinski M, Gandek B. (1993). SF-36 Health Survey Manual and Interpretation Guide. Boston, MA: New England Medical Center, The Health Institute. NEGATIVE LIFE EVENTS 20 Table 1 Demographic Characteristics of sample (n=218) Variable Range Mean Std. Deviation Age 12-32 yrs 21.45 4.48 Hollingshead 9-69 39.14 13.10 Gender (% female) 57.8% Gender (% male) 41.7% Race (% Caucasian) 90.8% Race (% other) 7.8% Table 2 Pearson’s Product-Moment Correlations Among Variables 1. 2. 3. 4. 5. 6. 7. Variable 1 Life stress Competence SF-36 CSI FDI Age Gender -- 2 3 4 5 -.246** -.413** .271** .207** -.502** -.234** -.292** --.506** -.432** -.758** -- **. Correlation is significant at the 0.01 level (2-tailed). *. Correlation is significant at the 0.05 level (2-tailed). 6 -.026** -.034 -.052 .180** .245** -- 7 -.173* .008 .130 -.253** -.174** -.002 -- NEGATIVE LIFE EVENTS 21 Table 3 Effect of life stress and competence and their interaction on SF-36 scores, controlling for age and gender Predictor variable Step 1: Control variables Age -.026 Gender .149 Step 2: Predictor variables Life events (LEQ) -.292 Social competence .442 Step 3: Two-way interaction Life Events x Social Competence .337 T p-value -.361 2.050 .719 .042 -4.721 7.255 .00 .00 1.188 .236 Table 4 Effect of life stress and competence and their interaction on CSI scores, controlling for age and gender Predictor variable Step 1: Control variables Age Gender Step 2: Predictor variables Life Events (LEQ) Social competence Step 3: Two-way interaction Life Events x Social Competence T .175 -.286 2.543 -4.158 .012 .000 .188 -.176 2.713 -2.588 .007 .010 -.670 -2.129 .035* p-value *p < .05 Table 5 Effect of life stress and competence and their interaction on FDI scores, controlling for age and gender Predictor variable Step 1: Control variables Age .261 Gender -.214 Step 2: Predictor variables Life events (LEQ) .123 Social competence -.254 Step 3: Two-way interaction Life Events x Social Competence -.456 T p-value 3.800 -3.112 .000 .002 1.797 -3.754 .074 .000 -1.453 .148 NEGATIVE LIFE EVENTS 22 Figure 1. The two-way interaction effect of stress and competence on CSI scores C S I S C O R E S 0.35 0.3 0.25 0.2 0.15 0.1 0.05 0 HighIV2 competence High Low IV2 Low competence IV 1 LowLow stress Highstress IV1 High High IV3