Therapeutic Apheresis Services Request for Therapeutic Plasma Exchange Ward Contact Number
advertisement

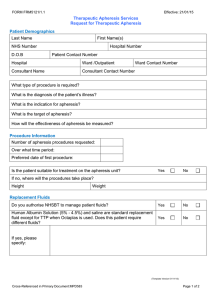
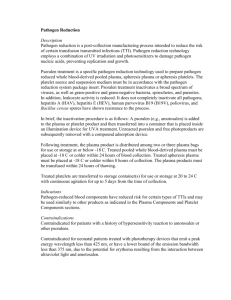
FORM FRM5122/1.1 Effective: 21/01/15 Therapeutic Apheresis Services Request for Therapeutic Plasma Exchange Patient Demographics Last Name First Name(s) NHS Number D.O.B Hospital Number Patient Contact Number Hospital Ward /Outpatient Consultant Name Consultant Contact Number Ward Contact Number Diagnosis Patient diagnosis: What is the indication for plasma exchange? What is the aim of plasma exchange? How will the effectiveness of plasma exchange be monitored? Treatment Requested Number of plasma exchanges requested: Over what time period: Preferred date of first procedure: Is the patient suitable for treatment on the apheresis unit? Yes No If no, where will the procedures take place? Height Weight Replacement Fluids Do you authorise NHSBT to manage patient fluids? Yes No Human Albumin Solution (5% - 4.5%) and saline are standard replacement fluid except for TTP when Octaplas is used. Does this patient require different fluids? Yes No If yes, please specify: (Template Version 01/11/13) Cross-Referenced in Primary Document: MPD583 Page 1 of 2 FORM FRM5122/1.1 Effective: 21/01/15 Therapeutic Apheresis Services Request for Therapeutic Plasma Exchange Other Information Does the patient have any significant co-morbidities which would require modification of the procedure (e.g. cardiovascular, renal or bleeding diathesis)? Medication: Does the patient have any allergies? Yes No (If yes, please specify) A full blood count is included in the treatment package price. Please provide forms / requests for any additional blood tests required Please provide relevant blood test / laboratory results Vascular Access Are peripheral veins adequate for apheresis? Yes No Is an apheresis central line already in place? Yes No Will an apheresis central line be inserted? Yes No (If yes, please advise date of insertion) Detail of member of staff completing this form Name: Grade: Date: Signature: Phone Number Email address: (*To ensure confidentiality please ensure an nhs.net email address is provided) For Use by NHS Blood and Transplant Has the referral been accepted? Yes No Comments: (Template Version 01/11/13) Cross-Referenced in Primary Document: MPD583 Page 2 of 2