Request for Extracorporeal Photopheresis (ECP) for CTCL
advertisement
 for CTCL")
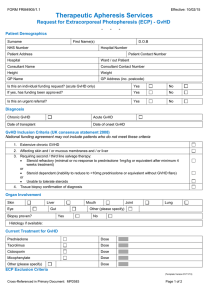
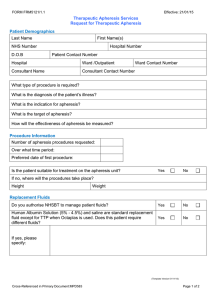
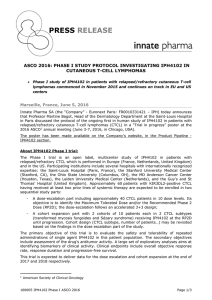
FORM FRM4906/1.1 Effective: 17/02/15 Therapeutic Apheresis Services Request for Extracorporeal Photopheresis (ECP) - CTCL - - - Patient Demographics Surname First Name(s) NHS Number D.O.B Hospital Number Patient Address Patient Contact Number Hospital Ward / out Patient Consultant Name Consultant Contact Number Height Weight GP Name GP Address (inc. postcode) Diagnostic criteria (tick all that apply) CTCL Stage III CTCL Stage IVA Circulating T cell clone Erythroderma Histology consistent with CTCL Sezary cells >10% circulating lymphocytes CD4 / CD8 ratio > 10 Other Information Is this an urgent referral? Yes No Does the patient have any significant co-morbidities which would require modification of the procedure (e.g. cardiovascular, renal, bleeding diathesis? Medication: Does the patient have any allergies? Yes No (If yes, please specify) A full blood count is included in the treatment package price. Please state any additional blood tests required and provide the completed relevant request forms ECP Exclusion Criteria 1. Pregnancy Yes No 2. History of heparin induced thrombocytopenia Yes No 3. Uncontrolled infection Yes No 4. Photosensitivity Yes No 5. Sensitivity to psoralen compounds Yes No 6. Aphakia Yes No Yes No 8. Platelet count < 20 x 109 / 1 Yes No 9. Severe diarrhoea > 1000ml daily Yes No 7. Neutrophil count < 1 x 109 /1 (Template Version 01/11/13) Cross-Referenced in Primary Document: MPD583 Page 1 of 2 FORM FRM4906/1.1 Effective: 17/02/15 Therapeutic Apheresis Services Request for Extracorporeal Photopheresis (ECP) - CTCL - - - Vascular Access (ECP requires 16g access in antecubital fossa and second access in opposite limb of at least 20g) Are peripheral veins adequate for apheresis? Yes No Is an apheresis central line already in place? Yes No Will an apheresis central line be inserted? Yes No (If yes, please advise date of insertion) Detail of member of staff completing this form Name: Grade: Phone Number: Date: Email address: Signature: (*To ensure confidentiality please ensure an nhs.net email address is provided) For Use by NHS Blood & Transplant ONLY Has the referral been accepted? Yes No Comments: (Template Version 01/11/13) Cross-Referenced in Primary Document: MPD583 Page 2 of 2