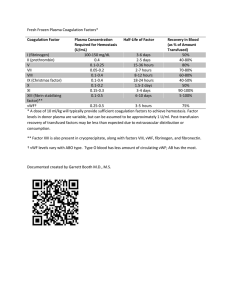
Type 2M von Willebrand Disease: F606I and I662F Mutations in... Ib Binding Domain Selectively Impair Ristocetin- but not Botrocetin-Mediated
advertisement

Type 2M von Willebrand Disease: F606I and I662F Mutations in the Glycoprotein Ib Binding Domain Selectively Impair Ristocetin- but not Botrocetin-Mediated Binding of von Willebrand Factor to Platelets By Cheryl A. Hillery, David J. Mancuso, J. Evan Sadler, Jay W. Ponder, Mary A. Jozwiak, Pamela A. Christopherson, Joan Cox Gill, J. Paul Scott, and Robert R. Montgomery von Willebrand disease (vWD) is a common, autosomally inherited, bleeding disorder caused by quantitative and/or qualitative deficiency of von Willebrand factor (vWF). We describe two families with a variant form of vWD where affected members of both families have borderline or low vWF antigen levels, normal vWF multimer patterns, disproportionately low ristocetin cofactor activity, and significant bleeding symptoms. Whereas ristocetin-induced binding of plasma vWF from affected members of both families to fixed platelets was reduced, botrocetin-induced platelet binding was normal. The sequencing of genomic DNA identified unique missense mutations in each family in the vWF exon 28. In Family A, a missense mutation at nucleotide 4105T = A resulted in a Phe606Ile amino acid substitution (F606I) and in Family B, a missense mutation at nucleotide 4273A = T resulted in an Ile662Phe amino acid substitution (I662F). Both mutations are within the large disulfide loop between Cys509 and Cys695 in the A1 domain that mediates vWF interaction with platelet glycoprotein Ib. Expression of recombinant vWF containing either F606I or I662F mutations resulted in mutant recombinant vWF with decreased ristocetin-induced platelet binding, but normal multimer structure, botrocetin-induced platelet binding, collagen binding, and binding to the conformation-sensitive monoclonal antibody, AvW-3. Both mutations are phenotypically distinct from the previously reported variant type 2MMilwaukee-1 because of the presence of normal botrocetin-induced platelet binding, collagen binding, and AvW-3 binding, as well as the greater frequency and intensity of clinical bleeding. When the reported type 2M mutations are mapped on the predicted three-dimensional structure of the A1 loop of vWF, the mutations cluster in one region that is distinct from the region in which the type 2B mutations cluster. r 1998 by The American Society of Hematology. V snake venom protein botrocetin, or by subjecting platelets and vWF to high shear stress.5-7 The domain that mediates vWF interaction with platelet GPIb is the large disulfide loop formed between Cys509 and Cys695 contained within the A1 domain of the vWF protein.8-10 vWD is broadly classified into types based on quantitative deficiencies of vWF (type 1 and type 3 vWD) and qualitative deficiencies in vWF (type 2 vWD).11 Type 2 vWD is further subdivided into various categories based on structural and functional abnormalities with the type 2M classification (type 2 mutations with normal multimers) being reserved for those that do not fit into the 2A, 2B, and 2N subgroups. Type 2M vWD was previously referred to as a variant of type 1 vWD, as there was no loss of high MW multimers, yet there was decreased platelet-dependent function.12 Our laboratory has recently reported type 2MMilwaukee-1 vWD, in which patients have a very mild bleeding disorder, a modest reduction of plasma vWF antigen (vWF:Ag) levels, disproportionately reduced vWF ristocetin cofactor activity (vWF:RCo), normal vWF multimers, and a parallel reduction in both ristocetin- and botrocetininduced binding of vWF to platelets.13 The genetic defect responsible for the low vWF:RCo activity in type 2MMilwaukee-1 vWD is an in-frame deletion of amino acids Arg629-Gln639 (DR629-Q639) in the large disulfide loop of the A1 domain of vWF. The only other type 2M variant to have been described and confirmed by recombinant expression of mutant vWF is subtype B vWD that is due to the missense mutation Gly561Ser (G561S).14 In comparing patients with low vWF levels and normal vWF multimers, we evaluated the ratio of vWF:RCo activity to vWF:Ag in 681 individuals as part of a previous study.13 Several patients, including those presented in this report, had vWF:RCo activity/vWF:Ag ratios that were decreased more than 2 standard deviations (SD) below the mean, suggesting a similar genetic lesion. We report here two new families with type 2M vWD, in which the affected individuals of both families have borderline or low vWF:Ag levels, normal vWF ON WILLEBRAND DISEASE (vWD) is a common, autosomally inherited bleeding disorder caused by a quantitative and/or qualitative deficiency of von Willebrand factor (vWF) affecting as many as 1% to 2% of the general population.1 vWF is an adhesive glycoprotein that is synthesized by both megakaryocytes and endothelial cells and is stored in the secretory granules of these cells as an array of multimers that range in molecular weight from 500-kD dimers to multimers in excess of 20,000 kD.2 The primary functions of vWF are to serve as a carrier protein for plasma factor VIII and as a ligand to support the adhesion of platelets to the subendothelial matrix at sites of vascular damage. vWF adheres to subendothelial matrix, likely through binding to collagen,3 after which there is a change in the conformation of vWF that converts it to an active ligand for the platelet adhesive receptor glycoprotein (GP) Ib.4 In vitro, vWF binding to platelet GPIb can be induced by the addition of the antibiotic ristocetin, the From the Blood Research Institute, The Blood Center of Southeastern Wisconsin, Milwaukee; the Department of Pediatrics, Medical College of Wisconsin, Milwaukee, WI; and the Howard Hughes Medical Institute and the Department of Biochemistry and Molecular Biophysics, Washington University School of Medicine, St Louis, MO. Submitted July 7, 1997; accepted October 17, 1997. Supported by Public Health Services Grants No. HL-44612 and HL-33721 (to R.R.M.), K08-HL-02858 (to C.A.H.), and Clinical Research Center Grant No. RR00058 from the National Institutes of Health and Grant-in-Aid 92-1340 (to D.J.M.) from the American Heart Association. Address reprint requests to Cheryl A. Hillery, MD, Blood Research Institute, The Blood Center of Southeastern Wisconsin, PO Box 2178, Milwaukee, WI 53233. The publication costs of this article were defrayed in part by page charge payment. This article must therefore be hereby marked ‘‘advertisement’’ in accordance with 18 U.S.C. section 1734 solely to indicate this fact. r 1998 by The American Society of Hematology. 0006-4971/98/9105-0006$3.00/0 1572 Blood, Vol 91, No 5 (March 1), 1998: pp 1572-1581 TYPE 2M VON WILLEBRAND DISEASE multimer patterns, disproportionately low vWF:RCo activity, and decreased ristocetin-induced platelet binding. Two new missense mutations were identified within the A1 loop of vWF. The vWF defects from affected individuals in the families described in the current report have normal botrocetin-induced platelet binding of vWF, normal collagen binding of vWF, and a stronger history of clinical bleeding and are thus phenotypically distinct from our previous report of type 2MMilwaukee-1 vWD.13 MATERIALS AND METHODS Patients. Two unrelated families with abnormal bleeding histories were identified with low vWF:Ag, disproportionately low vWF:RCo activity, and normal multimer structure in the affected members. Available members of three generations of each family were seen in the Pediatric Clinical Research Center at Children’s Hospital of Wisconsin. Plasma was evaluated by the Hemostasis Reference Laboratory at The Blood Center of Southeastern Wisconsin, Milwaukee, WI. Plasma vWF:RCo activity was determined by ristocetin-induced agglutination of formalin-fixed platelets as previously described.15 vWF:Ag levels of the same samples were measured by quantitative Laurell rocket immunoelectrophoresis.16 Plasma vWF multimers were analyzed by electrophoresis on a 0.65% sodium dodecyl sulfate (SDS)/agarose gel using a discontinuous buffer system and detection with 125I-anti–vWF antibody (Ab) as described by Ruggeri and Zimmerman.17,18 Polymerase chain reaction (PCR) amplification of genomic DNA. After obtaining informed consent, blood samples were collected from individuals in both families. Genomic DNA was prepared from peripheral white blood cells from patients AII-1 and AIII-1 in Family A and patients BII-1, BIII-1 and BIII-2 in Family B as previously described.19 The vWF DNA sequence is numbered starting from the ATG of the initiating Met codon of exon 2.20 Amino acid numbering starts with the mature vWF sequence. For selected Family A patients, vWF exon 28 was amplified from genomic DNA by PCR with Amplitaq Taq polymerase (Perkin-Elmer Cetus, Norwalk, CT) using sense primer VsI27-4:EcoRI (GAGgaatTcTGGGAATATGGAAGTCATTG) located in intron 27 and antisense primer VaI28-6:BamHI (tGAGgatccTCTTGGCAGATGCATGTAGC) located in intron 28 of the vWF gene.21 These primers were chosen for selective amplification of vWF gene sequence without interference from the vWF pseudogene.22 Lower case letters indicate where nucleotides (nt) differ from the vWF gene sequence for the purpose of introducing restriction enzyme sites into the final product. For selected Family B patients, DNA from exon 28 of the vWF gene was amplified by PCR using sense primer VsI27-3 (CCACAGGTTCTTCCTGAACCATT) located in intron 27 and antisense primer a5040-5020 located in exon 28 of the vWF gene. This was followed by a second amplification using nested sense primer Vs3673-3697:Nsi I (atgCAtTGTGATGTTGTCAACCTCA) and antisense primer a44884462. After PCR amplification, the amplified DNA products were subcloned into plasmids (TA cloning PCR Vector by Invitrogen, Carlsbad, CA; Version 2.0) and sequenced using Sequenase kit (V.2.0, United States Biochemical, Cleveland, OH). Rapid PCR/restriction digestion method for detection of mutations. Because the mutation in Family A does not create or delete a restriction site, a Bcl I restriction site unique to the mutation in Family A was created using additional base changes in a PCR primer. Primer Vs4067 (tgtggtGCGAGGTCTTGAAATACACACTGTTCCtgATC) introduced a TG (underlined) at nts 4100-1 such that the Bcl I restriction site (tgATCA4105) is created only when the missense mutation 4105T = A in the mutant vWF allele is present. When this PCR primer is paired with antisense primer Va4398-4357:Nsi I (AGGAGGGGaTgCAtGGGCAgGGTCACAGAGGT), the product is 336 bp long. When PCR product is digested with Bcl I, only the mutant vWF PCR product is cut into two fragments, 302 and 34 bp long. In Family B, the new mutation 4273A = T results in the loss of a restriction site for BstYI (Pu-GATCPy). Genomic DNA 1573 was subjected to first round PCR with sense primer VsI27-3 and antisense primer a5040-5020 as described above. After a second PCR amplification with nested primers Vs3673-3697:Nsi I and a4488-4462, a 815-bp product is amplified from vWF genomic DNA. When this PCR product is digested with BstYI, only the normal allele is cut into two fragments of 598 and 217 bp, respectively. Plasmid constructs and expression of recombinant vWF. The Asp I/Nco I restriction fragments (nt 3832-4481 of vWF) of the subcloned PCR products amplified from genomic DNA from patients AII-1 and AIII-1 in Family A and patients BII-1 and BIII-2 in Family B were subcloned into P18vW1, an intermediate vector that was constructed by the insertion of the BamHI/Kpn I restriction fragment (nt 2717-4752 of mature vWF) from the full length vWF cDNA expression plasmid pvW198.1 (provided by Dennis Lynch, Dana Farber Cancer Center, Boston, MA) into the plasmid vector pUC-18 (United States Biochemical).19 The BamHI/Kpn I restriction fragment of the resulting construct containing the vWD mutant sequence was ligated into the corresponding BamHI and Kpn I sites of the full-length vWF expression plasmid pvW198.1. The pvW198.1 and mutant expression plasmids were used to transfect COS-7 cells in the presence of Lipofectamine (GIBCOBRL, Gaithersburg, MD) using the protocol of Felgner et al.23 After 48 hours, conditioned media were harvested, cleared by low speed centrifugation, and stored at 280°C. vWF:Ag levels in conditioned media were assayed by antigen-capture enzyme-linked immunosorbent assay (ELISA) using monoclonal antibody (MoAb) AvW-124 and detected by anti-vWF rabbit polyclonal Ab followed by biotinconjugated goat antirabbit IgG (Pierce, Rockford, IL). Immune complexes were detected using avidin-horseradish peroxidase, and o-phenylenediamine substrate (Sigma, St Louis, MO). Multimer analysis of recombinant vWF. Recombinant vWF was immunoprecipitated with vWF MoAb AvW-1 coupled to Sepharose-4B (Pharmacia, Piscatay, NJ). Immunoprecipitated vWF (14 ng) was analyzed on a 1.5% resolving gel as described by Raines et al,25 with the following modifications. After adding the samples to the wells, electrophoresis was performed at 150 V (constant) for 7 to 8 hours in a Bio-Rad Model 1415 electrophoresis chamber (Bio-Rad Laboratories, Richmond, CA) cooled to 15°C. After electrophoretic transfer to nitrocellulose, recombinant vWF multimers were detected using antivWF rabbit polyclonal Ab followed by horseradish peroxidaseconjugated goat antirabbit IgG (Pierce) and visualized by chemiluminescence using the ECL Western blot detection system (Amersham Corp, Arlington Heights, IL). Platelet binding assay. The binding of vWF to fixed platelets was measured using a modification of a procedure previously described.19,26 Briefly, AvW-1, a vWF MoAb that does not interfere with vWF binding to either GPIb or GPIIbIIIa,24,27 was labeled with 125I (DuPont NEN, Boston, MA) using Iodo-Beads (Pierce). 125I-AvW-1 was incubated with either plasma (3 parts plasma: 1 part 125I-AvW-1, 6,000 cpm/µL) or conditioned medium (60 parts conditioned medium: 1 part 125I-AvW-1, 2,000 cpm/µL) for 30 to 60 minutes at 22°C. For recombinant vWF experiments, conditioned medium from transfected COS-7 cells or normal pooled human plasma were diluted in Tris-saline (20 mmol/L Tris pH 7.4, 150 mmol/L NaCl) such that equal amounts of vWF (determined by ELISA as described above) were used within a single platelet binding experiment (range, 50 to 100 ng/mL). Labeled plasma (35 µL, 50,000 cpm) or conditioned media (300 µL, 10,000 cpm) was incubated with formalin-fixed platelets (200 µL of 2 3 108/mL for plasma, or 40 µL of 4 3 108/mL for recombinant vWF experiments, BioData, Hatboro, PA) in the presence of ristocetin (Helena, Beaumont, TX), botrocetin, or control buffer and gently rocked for 30 to 60 minutes at 22°C. Botrocetin was purified as described by Andrews et al.28 After pelleting platelets and platelet bound vWF (12,000g, 10 minutes), the upper half of the supernatant was transferred to a clean tube. The amount of radioactivity in the pellet half (a) and the supernatant half (b) fractions was determined using a gamma counter. The percent of vWF 1574 bound to the platelets was calculated using the formula: [(a 2 b)/(a 1 b)]*100. Collagen and AvW-3 binding assay. Type III collagen (6 µg/mL, Southern Biotechnology Associates, Birmingham, AL), vWF MoAb AvW-1 (5 µg/mL), or MoAb AvW-3 (5 µg/mL), a vWF MoAb that binds vWF and inhibits its interaction with GPIb,27,29 in a carbonate buffer was plated on microtiter wells (50 µL/well) at 4°C overnight. After blocking (0.05% Tween-20 in Tris-saline, 2 to 3 hours, 22°C) and washing, 50 µL of conditioned medium from transfected COS-7 cells, diluted to approximate concentrations of both 100 ng/mL and 50 ng/mL of recombinant vWF in blocking buffer, was added to wells in triplicate and incubated at 22°C for 60 minutes. After washing the wells, bound recombinant vWF was detected by ELISA using rabbit anti-vWF polyclonal Ab followed by horseradish peroxidase-conjugated goat antirabbit IgG (Pierce). Immune complexes were detected using o-phenylenediamine (Zymed, San Francisco, CA). Bound vWF was quantitated by comparing the resultant optical density (above background) with a standard curve of pooled normal plasma vWF binding that was performed in parallel in each of these studies. The amount of vWF added to the wells was quantitated by binding to AvW-1–coated wells in parallel experiments. The amount of recombinant vWF bound to collagen or AvW-3 was expressed as a ratio of the amount of vWF bound to collagen or AvW-3 divided by the amount of vWF added to the well. vWF A1 domain molecular model. The coordinates for the A domains of integrins aM (Mac-1)30 and aL (LFA-1)31 were generously provided by Robert C. Liddington (University of Leicester, Leicester, UK) and Daniel J. Leahy (Johns Hopkins University, Baltimore, MD), respectively. The sequence for human vWF domain A1 (residues Cys509-Cys695) was aligned with the sequences of the homologous A domains of aM and aL using the three-dimensional profile method of HILLERY ET AL Bowie et al.32 Amino acids CSR and LC were added to the aminoterminus and carboxy-terminus, respectively, of the aM structure. The two cysteine residues were joined, and the new segment was subjected to molecular dynamics annealing using the program TINKER.33 Residues in aM were replaced by the corresponding aligned residues in vWF domain A1. Improper contacts were removed and the resulting structures were refined using the program WHAT IF.34,35 Small insertions or deletions in surface loops were modeled by adding or deleting residues, followed by local energy minimization with the program TINKER (steepest descent conjugate gradient or preconditioned truncated Newton methods).33 The model was evaluated for improper contacts and bond angles; where appropriate, segments with bad conformations underwent molecular dynamics annealing. The entire model was energy-minimized to RMS gradient ,0.01 kcal/mol (preconditioned truncated Newton method). The packing quality of the final model was –1.195 sigma.36 RESULTS Description of two family pedigrees. Figure 1 shows the pedigrees of Family A and Family B (Figs 1A and, B). Members from three generations of each family were available for study. The index case in Family A (AIII-1) presented in childhood with a lifelong history of increased bruising and moderately severe epistaxis; she required 1-desamino-8-D-arginine vasopressin (DDAVP) or vWF replacement therapy on multiple occasions. She also experienced bleeding 2 days posttonsillectomy despite perioperative vWF replacement therapy. The other affected members of Family A (AI-1 and AII-1) have an extensive history of increased bruising. The index case in Family B Fig 1. Family pedigree and analysis of plasma vWF from two families with type 2M vWD. (A and B) Three generations of the family pedigree are illustrated showing affected (shaded symbol) and unaffected (open symbol) family members for Family A (A) and Family B (B). vWF:RCo/vWF:Ag ratios determined from testing in a clinical laboratory are shown below selected symbols (U/dL). (C and D) Autoradiograms of plasma vWF multimer structure from Family A (C: AII-1, AIII-1), Family B (D: BII-1, BI-1, BIII-1, BIII-2), or normal pooled human plasma (NP) resolved by 0.65% SDS/agarose gel electrophoresis and detected with 125I–anti-vWF Ab as described in Materials and Methods. TYPE 2M VON WILLEBRAND DISEASE (BIII-2) presented in infancy with a history of prolonged bleeding from the umbilical cord stump; he subsequently developed increased bruising and frequent severe epistaxis. The epistaxis frequently requires DDAVP, vWF replacement therapy and/or cautery; he has been placed on prophylactic replacement therapy to control his bleeding on several occasions. The other affected individuals of Family B (BII-1 and BIII-1) have lifelong histories of increased bruising and moderately severe epistaxis during childhood; the bleeding symptoms of BII-1 have improved as an adult. Multimeric analysis of their vWF shows a normal distribution pattern of multimers in affected members of both families (Fig 1C and D). The ratio of the clinical assays for vWF:RCo and vWF:Ag of individuals from Family A and Family B were compared with the ratio of these assays in 681 individuals with low vWF:Ag and normal vWF multimers that were previously reported.13 As shown in Fig 2 and Table 1, the affected individuals from Family A and Family B, as well as the previously reported patients with type 2MMilwaukee-1, show vWF:RCo/vWF:Ag ratios that are more than 2 SD below the mean. While the vWF:RCo, vWF:Ag, and the vWF:RCo/vWF:Ag ratios all increase after treatment with DDAVP, the disproportionate ratio of vWF:RCo to vWF:Ag remains more than 2 SD below the normal range (Table 1 and Fig 2). The moderate increase in the vWF:RCo/ vWF:Ag ratio after DDAVP is similar to that seen in patients with type 1 vWD after DDAVP therapy (data not shown). In unaffected family members, the vWF:RCo/vWF:Ag ratio is 1575 Table 1. Family A and Family B vWF:RCo and vWF:Ag Levels Individual Condition vWF:RCo vWF:Ag Ratio Factor VIII Normal Range AI-1 AI-2 AII-1 AII-1 AII-2 AIII-1 AIII-1 AIII-2 AIII-3 BI-1 BII-1 BII-1 BII-2 BIII-1 BIII-1 BIII-2 BIII-2 Baseline Baseline Baseline DDAVP Baseline Baseline DDAVP Baseline Baseline Baseline Baseline DDAVP Baseline Baseline DDAVP Baseline DDAVP 45-200 13 102 9 70 68 4 33 74 98 86 16 84 108 22 70 11 37 45-200 36 110 19 128 73 13 54 72 97 80 48 122 101 62 144 36 71 0.72-1.26 0.36 0.93 0.47 0.55 0.93 0.31 0.61 1.03 1.01 1.08 0.33 0.69 1.07 0.35 0.49 0.31 0.52 55-170 49 32 181 82 34 96 90 107 95 58 188 110 73 185 43 117 The vWF:RCo (U/dL), vWF:Ag (U/dL), vWF:RCo/vWF:Ag ratio and factor VIII:C activity (U/dL) of three generations of Family A and Family B were determined from testing in a clinical laboratory. The identity of each individual is defined in the pedigree in Fig 1. For selected affected family members only, the vWF:RCo and vWF:Ag levels were also measured 1 hour after treatment with DDAVP. normal (Fig 2). In contrast to the marked reduction in the vWF:RCo/vWF:Ag ratio, there was minimal reduction in the ristocetin-induced platelet binding of plasma vWF from affected individuals of both families (Table 2). Plasma vWF from affected members of both families had normal botrocetininduced binding to fixed platelets (Table 2). Identification of unique missense mutations in the vWF A1 binding domain for both families. The site of vWF interaction with platelet GPIb receptor has been localized to the A1 domain of the mature vWF glycoprotein37-39 that is encoded by exon 28 of the vWF gene.8 Therefore, vWF exon 28 was amplified by PCR from genomic DNA from two patients in each family and subcloned into plasmids for DNA sequencing. In Family A, a single T = A missense mutation at nt 4105 was detected for both patient AII-1 and patient AIII-1, resulting in the substitution of Ile for Phe606 (F606I, Fig 3A). The normal allele was Table 2. Ristocetin- and Botrocetin-Induced Binding of Plasma vWF to Platelets Fig 2. Decreased vWF:RCo/vWF:Ag ratios in individuals with type 2M vWD. Depicted are the vWF:RCo/vWF:Ag ratios of individuals with low vWF:Ag and normal vWF multimers (Type 1 vWD, X), type 2MMilwaukee-1 vWD (D629-639, W), affected (M) or unaffected (N) members of Family A and affected (Q) or unaffected (S) members of Family B studied at The Blood Center of Southeastern Wisconsin. The change in vWF:RCo/vWF:Ag ratios of affected members of Family A and Family B 1 hour after DDAVP therapy is also shown (DDAVP 1). The data for the individuals with type 1 vWD and type 2MMilwaukee-1 vWD has been previously reported.13 Agonist NP Family A (F606I) Family B (I662F) Ristocetin Botrocetin Control 73.1 (6 1.6) 87.3 (6 0.7) 20.9 (6 3.0) 50.0 (6 21.6) 84.4 (6 0.1) 1.1 (6 6.5) 64.8 (6 5.2) 85.8 (6 1.6) 2.1 (6 0.1) Plasma labeled with 125I-AvW-1 vWF MoAb was incubated with formalin-fixed platelets in the presence of ristocetin (1.2 mg/mL, Ristocetin), botrocetin (2 µg/mL, Botrocetin) or control buffer (Control) as described in Materials and Methods. After pelleting platelets and associated bound vWF, bound and unbound 125I–AvW-1 were detected by gamma counting, and percent bound 125I–AvW-1 calculated as described in Materials and Methods. The percent 125I–AvW-1 bound from normal pooled plasma (NP), affected Family A member AIII-1 plasma (F6061), or affected Family B member BII-1 plasma (I662F) are shown as the mean (6 SD) of two separate experiments. 1576 HILLERY ET AL A B C D Fig 3. Sequence of normal and mutant alleles of vWF DNA and PCR analysis of patient DNA. (A and B) PCR products containing vWF exon 28 sequence were amplified from genomic DNA and subcloned as described in Materials and Methods. Representative sequences of clones containing the normal allele and mutant allele for Family A (A) and Family B (B) are shown in the region of the point mutation in the mutant allele. As indicated in the translated sequence below, the missense point mutation in nt 4105T = A results in a Phe606Ile amino acid substitution for Family A (A) and the missense point mutation in nt 4273A = T results in a Ile662Phe amino acid substitution for Family B (B). (C) In Family A, a restriction site for Bcl I was introduced only in the mutant allele by PCR using specially-constructed primers (Vs4067 and Va4398) that flank the point mutation. The PCR products were amplified from genomic DNA from a normal control (N) or Family A patients (AIII.1 and AII.1). When the PCR product (336 bp) is digested with Bcl I, only the mutant vWF allele is cut into two fragments, 302 and 34 bp long. (D) In Family B, a native restriction site for BstYI is lost in the mutant allele. Genomic DNA from a normal control (N) or Family B patients (BII.1, BIII.1, and BIII.2) is amplified by PCR with primers VsI27-3 and Va5040-5020 followed by a second round of PCR with primers Vs3673:Nsi I and Va4488-4462:Nco I. When PCR product (815 bp) is digested with BstYI, only the normal allele is cut into two fragments, 598 and 217 bp long. Molecular weight standards (bp) are shown on the side. also identified in both of these patients. These patients were also heterozygous for a commonly occurring A/G polymorphism at nt 4141,40 and a T/C polymorphism at nt 4641,40 with the 4141A and the 4641T polymorphisms occurring in association with the missense mutation (data not shown). In Family B, an A = T missense mutation at nt 4273 was detected in both patient BII-1 and patient BIII-2, resulting in the substitution of Phe for Ile662 (I662F, Fig 3B). Again, both normal and mutant alleles were identified, showing that the affected individuals were heterozy- gous for the missense mutation. The patients were also heterozygous for a commonly occurring G/A polymorphism at nt 4196, with the G polymorphism occurring in association with the missense mutation (data not shown). Detection of vWF missense mutation in affected family members by restriction digestion of PCR products. A Bcl I restriction site unique to the mutation in Family A was created using additional base changes in a PCR primer. Figure 3C illustrates the selective cutting of PCR products by Bcl I only in TYPE 2M VON WILLEBRAND DISEASE the affected Family A members, AIII-1 and AII-1, but not in a normal individual. Both Family A members were heterozygous for the full-length (336 bp) and cut (302 bp) PCR products after Bcl I digestion, showing that the affected individual had both normal and mutant alleles. In Family B, the new mutation 4273A = T results in the loss of a restriction site for BstYI. Figure 3D illustrates the selective retention of full-length PCR product after BstYI digestion only in the affected Family B members, BII-1, BIII-1, and BIII-2, but not in the normal individual. Again, both full-length and cut PCR products were observed in affected family members, providing further evidence that affected members of Family B are heterozygous for the missense mutation. Expression and structural characterization of recombinant mutant F606I and I662F vWF. To determine the effect of the missense mutation on vWF structure and function, restriction fragments containing the 4105T = A mutation from Family A and the 4273A = T mutation from Family B were inserted into the full-length expression vector pvW198.1. Wild-type (wt) and both mutant vWFs were transiently expressed in COS-7 cells. As shown in Fig 4, both recombinant F606I and I662F mutant vWFs and wt vWF formed multimer patterns containing similar amounts and proportions of all multimer sizes. Fig 4. Multimer analysis of recombinant expressed vWF mutant missense mutations. Recombinant vWF was immunoprecipitated from conditioned media of transfected COS-7 cells, resolved by SDS/agarose gel electrophoresis and detected with 125I–anti-vWF Ab as described in Materials and Methods. Pictured are autoradiograms of recombinant vWF (14 ng) containing the point mutation from Family A (F606I), Family B (I662F), wt recombinant vWF (WT) or immunoprecipitated conditioned medium from mock transfected cells (Mock). 1577 Fig 5. Ristocetin- and botrocetin-induced binding of recombinant vWF to platelets. Conditioned media from transfected COS-7 cells labeled with 125I–AvW-1 were incubated with formalin-fixed platelets in the presence of ristocetin (1.2 mg/mL, Ristocetin, shaded bars), botrocetin (2 mg/mL, Botrocetin, hatched bars), or control buffer (Control, open bars) as described in Materials and Methods. After pelleting platelets and associated bound vWF, bound and unbound 125I–AvW-1 was detected by gamma counting, and percent bound 125I–AvW-1 calculated as described in Materials and Methods. The percent 125I–AvW-1 bound from normal pooled plasma (NP, n 5 3), wt recombinant vWF (WT, n 5 4), recombinant vWF containing the mutation from Family A (F606I, n 5 5), Family B (I662F, n 5 5), type 2MMilwaukee-1 vWD (D629-639, n 5 2) or conditioned medium from mock-transfected cells (Mock, n 5 4) are plotted as the mean 6 SD. Ristocetin- and botrocetin-induced binding of recombinant mutant vWF to platelets. To test the functional characteristics of the missense mutations, platelet binding assays were performed with the recombinant mutant and wt vWF expressed by the transfected COS-7 cells.19,26 The binding of vWF to platelets was quantitated by a radiolabeled, noninhibitory, vWF MoAb AvW-1 that bound to vWF and was cosedimented with platelets through platelet-associated vWF. As shown in Fig 5, normal plasma vWF and wt recombinant vWF bound to fixed platelets in the presence of ristocetin (1.2 mg/mL) to similar levels. No appreciable binding of AvW-1 to platelets was seen when conditioned media from mock transfected cells was used. In the presence of ristocetin, expressed recombinant F606I and I662F vWF had decreased binding to platelets compared with wt recombinant vWF and normal plasma vWF. However, both mutant proteins showed normal levels of botrocetin-induced binding to platelets. This is in contrast to another recently described type 2M variant caused by an in-frame deletion within the A1 domain (DR629-Q639), type 2MMilwaukee-1 vWD, that has both decreased ristocetin- and botrocetin-induced platelet binding (see Fig 5).13 The reduced ristocetin-induced vWF binding and normal botrocetin-induced binding observed for the F606I and I662F variants is similar to, but more severe in magnitude, than that observed for the native plasma vWF in the affected family members. This is likely because the plasma of these heterozygous affected individuals contains both mutant vWF and normal vWF. In contrast, the expressed multimers contained only the mutant vWF. These data support the conclusion that the F606I and the I662F missense mutations are responsible for deficient vWF activity in the affected individuals in Family A and B, respectively. Both the blocking anti-GPIb 1578 HILLERY ET AL MoAb, AP-1,24 and the blocking A1 domain vWF MoAb, AvW-3,27,29 inhibited recombinant mutant vWF binding to platelets in the presence of either ristocetin or botrocetin indicating that the variant vWF binds to platelets via GPIb, similar to wt vWF (data not shown). Binding of recombinant vWF to collagen. While the A3 domain of vWF is the putative major binding site for collagen,41 the A1 domain of vWF may also contribute to vWF interactions with collagen.42 Recombinant F606I and I662F vWF both bound to collagen under static conditions to levels similar to wt vWF (Fig 6A). In contrast, the type 2MMilwaukee-1 variant, DR629-Q639,13 had reduced levels of binding to collagen (Fig 6A). This suggests that the A1 domain of vWF can significantly contribute to the interaction between vWF and collagen. Binding of recombinant vWF to AvW-3. Because vWF MoAb AvW-3 inhibits the binding of vWF to GPIb,27,29 the binding of this MoAb to wt, F606I, I662F, and DR629-Q639 vWF was determined. As shown in Fig 6B, AvW-3 bound the wt, F606I, and I662F vWF to similar levels, while AvW-3 binding to DR629-Q639 vWF was absent. In addition, AvW-3 immunoprecipitates the wt, F606I, and I662F mutant vWF, but does not immunoprecipitate the type 2MMilwaukee-1 mutant vWF, DR629-Q639 (data not shown). DISCUSSION Two lines of evidence support the conclusion that the vWF missense mutations F606I in Family A and I662F in Family B are responsible for the functional characteristics of the type 2M vWD. First, both missense mutations and the low vWF:RCo/ vWF:Ag ratio are coinherited in an autosomal dominant manner through two or three generations of the affected families. Second, similar to patient plasma vWF, recombinant vWF containing each missense mutation is deficient in ristocetinmediated vWF binding to platelets, yet retains normal multimer structure, botrocetin-mediated platelet binding, collagen binding, and AvW-3 binding. We speculate that the more severe ristocetin-mediated binding defect observed for mutant recombinant vWF compared with the same patient’s plasma vWF is due to expression of only the defective vWF in transfected cells versus heterozygous expression of mutant and normal vWF in the plasma of the affected patients. Interestingly, the missense mutation in Family A (4105T = A) is also present in the vWF pseudogene.22 However, no other pseudogene specific sequences were present in exon 28 of Family A. Additionally, Meyer et al43 recently reported a French family with a type 2M phenotype that also had the I662F mutation; the genomic nt mutation was not reported and the mutation has not been expressed. However, this preliminary data further supports our conclusion that the I662F mutation is responsible for the type 2M phenotype described in this report. Both of these two new type 2M vWD variants are characterized by normal multimer structure, low vWF:RCo/vWF:Ag ratio, but normal botrocetin-mediated platelet binding, collagen binding, and AvW-3 binding. Only two other type 2M mutations have been described and confirmed by recombinant expression of mutant vWF: subtype B vWD14 and type 2MMilwaukee-1 vWD (DR629-Q639).13 Subtype B vWD is due to the missense mutation Gly561Ser (G561S) that causes decreased ristocetinmediated platelet binding, but normal botrocetin-mediated platelet binding and a normal multimer pattern.14 The two new variant forms of vWD described in this study are similar to G561S vWF and type 2MMilwaukee-1 vWF with regard to the normal multimer structure, decreased ristocetin-induced platelet binding and amino acid modifications localized within the Cys509-Cys695 loop. However, in contrast to the type 2MMilwaukee-1 vWD that has reduced botrocetin-mediated platelet binding and minimal clinical bleeding symptoms, the G561S vWF and the two new missense mutations described in this study have normal botrocetin-induced platelet binding, yet significant clinical bleeding symptoms. These data suggest a lack of clinical correlation between botrocetin-induced vWF reactivity and in vivo function of vWF. Furthermore, the difference in type III collagen binding between type 2MMilwaukee-1 vWF (decreased collagen binding) and the clinically symptomatic type 2M F606I and I662F vWF variants described in this study (normal collagen binding) suggest that the effect of these mutations on collagen binding as measured in these static assays do not significantly alter the interaction of vWF with collagen or other subendothelial components during primary hemostasis. However, this data does suggest that the A1 domain can specifically Fig 6. Recombinant vWF binds type III collagen and vWF MoAb AvW-3. Conditioned media from transfected COS-7 cells containing recombinant vWF from wt vWF (WT), Family A mutation (F606I), Family B mutation (I662F), or type 2MMilwaukee-1 vWD (D629-639) were incubated in microtiter wells coated with type III collagen (0.3 mg/well) or AvW-3 (0.25 mg/well). Bound vWF was detected by ELISA as described in Materials and Methods. The amount of vWF bound to collagen (A) or AvW-3 (B) is shown as the ratio of vWF bound (ng/mL) divided by the amount of vWF added to the well (ng/mL). The graph depicts the mean 6 SD of two experiments. TYPE 2M VON WILLEBRAND DISEASE affect the interaction of vWF with type III collagen. In contrast to the profound reduction in the vWF:RCo/vWF:Ag ratio in affected individuals from the type 2M vWD families described in this study, there was only minimal reduction in the ristocetininduced binding of plasma vWF to fixed platelets. This suggests that the vWF:RCo/vWF:Ag ratio is more sensitive than the direct platelet-binding assay in the detection of clinically important deficiencies in the interaction of vWF with platelet GPIb. To facilitate understanding of vWF A1 domain structurefunction relationships, a molecular model of the domain was constructed based on the crystallographic structures of the homologous domains of aM (Mac-1)30 and aL (LFA-1)31(Fig 7). These domains consist of a central 5-stranded parallel b-sheet with a short sixth antiparallel strand on one edge. This core is surrounded by amphipathic a-helices in a typical open a/b sheet or dinucleotide-binding fold.44 Amino acid residues that coordinate metal ions at the top of the aM and aL domains are 1579 not conserved in vWF, and this is consistent with the observation that binding functions of the vWF A1 domain do not require divalent cations. The organization of this domain predicted by computer modeling appears to agree with that determined directly by x-ray crystallography, as described in a recent preliminary report,45 and the model provides a useful framework for understanding the structure-function relationships of the vWF A1 domain. The locations of residues known to be mutated in patients with type 2M vWD and type 2B vWD are shown within the modeled A1 loop of vWF in Fig 7. Type 2B vWF mutations, which result in enhanced affinity of vWF for the platelet GPIb/IX complex, cluster between Met540 and Arg578 within the amino-terminal half of the disulfide loop.46 In the molecular model, all the vWD type 2B gain-of function mutations map to a patch of 30x20 Å near the ‘‘base’’ of the globular A1 domain. In contrast, the vWD type 2M mutations, G561S, DR629-Q639, I662F, and F606I, appear to cluster at the top of the domain Fig 7. Location of vWD type 2M and type 2B mutations in the vWF A1 domain. The a-carbon trace is shown for the vWF A1 domain, modeled on the crystallographic structures of the homologous aM and aL A domains as described in Materials and Methods. The locations are shown of residues known to be mutated in patients with vWD type 2M (G561, I662, F606, and DR629-Q639) and vWD type 2B (R543, R545, W550, V551, V553, R574, and R578). 1580 despite their significant separation based on the linear sequence location. While the type 2M mutation G561S is sequentially near the region where most of the type 2B gain-of function mutations are clustered,46 the three-dimensional molecular model clearly places the Gly561 spatially closer to the other 2M mutations and distant from the 2B mutations. Although the type 2M mutations I662F and G561S are located near proposed sites for botrocetin binding to vWF as identified by peptide inhibition studies (Asp539-Val553, Lys569Gln583, and Arg629-Lys643)47 or scanning mutagenesis (Arg663-Lys667)48, neither residue is directly within the proposed botrocetin binding segments. Additionally, while a recently proposed model for the regulation of vWF binding to GPIb based on studies of mutants generated by scanning alanine mutagenesis places F606I within one of several discontinuous segments that likely contributes to the interaction of vWF with platelet GPIb,48 the results of this study show that F606 is not a critical residue for GPIb binding within this segment. Consequently, the type 2M mutations G561S, F606I, and I662F that retain normal botrocetin-induced binding to platelet GPIb do not appear to directly affect residues identified as essential for binding to botrocetin or GPIb. The type 2M mutations G561S, F606I, and I662F have decreased vWF:RCo yet retain normal botrocetin-induced binding to platelet GPIb. In addition, charged-to-alanine mutations at Glu626 and Asp520-Lys534,48 and at Lys534, Lys569, and Lys642-Lys64549 of vWF resulted in reduced ristocetin-induced binding, but not botrocetin-induced binding of vWF to platelets. These results are consistent with ristocetin and botrocetin each having independent structural requirements or mechanisms for mediating the interaction of vWF with the platelet GPIb/IX complex.50 The ability of these mutant vWF proteins to bind platelet GPIb in the presence of botrocetin support the conclusion that the GPIb binding site remains intact, while the ristocetin-mediated allosteric regulation of vWF binding is disrupted. Furthermore, these results suggest that discontinuous regions and/or a major portion of the 509-695 disulfide loop are involved in modulation of ristocetin-mediated binding of vWF to platelet GPIb. These two new type 2M families provide further support for the hypothesis that defects for other vWD variants with a low vWF:RCo/vWF:Ag ratio in the setting of normal multimer structure may be localized to exon 28 of the vWF gene. The clustering of mutations for other similar vWD variants within exon 28 will facilitate the rapid genetic diagnosis of these variants. In addition, identification and characterization of genetic defects for these families with variant vWD will provide further insight into the role of the Cys509-Cys695 loop in the interaction of vWF with the platelet GPIb/IX complex and a better understanding of the structural and functional characteristics of vWF in general. Furthermore, an improved classification of vWD, based on known structural and functional characteristics and genetic mutations of vWF, may result for this heterogeneous disorder. An improved classification for vWD based on genotypic analysis should better predict phenotypic expression and therefore aid in diagnosis and management of this disease. HILLERY ET AL ACKNOWLEDGMENT The authors thank Drs Robert C. Liddington (University of Leicester) and Daniel J. Leahy (Johns Hopkins University) for providing coordinates of Mac-1 and LFA-1, respectively. We also thank Elizabeth A. Vokac, Naomi Blankenburg, Ming C. Du, and Todd Schroeder for assistance with the platelet- and collagen-binding studies, Thomas J. Barbour and Xio Liu for technical assistance with recombinant studies, and Amy Frey for assistance with the multimer analysis. In addition, we would like to thank Janet L. Endres for expert technical advice and Philip A. Kroner for critical review of the manuscript. REFERENCES 1. Montgomery RR, Coller BS: von Willebrand Disease, in Colman RW, Hirsh J, Marder VJ, Salzman EW (eds): Hemostasis and Thrombosis: Basic Principles and Clinical Practice. Philadelphia, PA, Lippincott, 1994, p 134 2. Mayadas TN, Wagner DD: von Willebrand factor biosynthesis and processing. Ann N Y Acad Sci 614:153, 1991 3. Santoro SA: Adsorption of von Willebrand factor/factor VIII by the genetically distinct interstitial collagens. Thromb Res 21:689, 1981 4. Weiss HJ: von Willebrand factor and platelet function. Ann N Y Acad Sci 614:125, 1991 5. Ruggeri ZM, De Marco L, Gatti L, Bader R, Montgomery RR: Platelets have more than one binding site for von Willebrand factor. J Clin Invest 72:1, 1983 6. Nachman RL, Jaffe EA, Weksler BB: Immunoinhibition of ristocetin-induced platelet aggregation. J Clin Invest 59:143, 1977 7. Fujimura Y, Holland LZ, Ruggeri ZM, Zimmerman TS: The von Willebrand factor domain-mediating botrocetin-induced binding to glycoprotein IB lies between Val449 and Lys728. Blood 70:985, 1987 8. Fujimura Y, Titani K, Holland LZ, Russell SR, Roberts JR, Elder JH, Ruggeri ZM, Zimmerman TS: von Willebrand factor. A reduced and alkylated 52/48-kDa fragment beginning at amino acid residue 449 contains the domain interacting with platelet glycoprotein Ib. J Biol Chem 261:381, 1986 9. Andrews RK, Gorman JJ, Booth WJ, Corino GL, Castaldi PA, Berndt MC: Cross-linking of a monomeric 39/34-kDa dispase fragment of von Willebrand factor (Leu-480/Val-481-Gly-718) to the N-terminal region of the alpha-chain of membrane glycoprotein Ib on intact platelets with bis(sulfosuccinimidyl) suberate. Biochemistry 28:8326, 1989 10. Marti T, Rosselet SJ, Titani K, Walsh KA: Identification of disulfide-bridged substructures within human von Willebrand factor. Biochemistry 26:8099, 1987 11. Sadler JE: A revised classification of von Willebrand disease. For the Subcommittee on von Willebrand Factor of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost 71:520, 1994 12. Ruggeri ZM: Structure and function of von Willebrand factor: Relationship to von Willebrand’s disease. Mayo Clin Proc 66:847, 1991 13. Mancuso DJ, Kroner PA, Christopherson PA, Vokac EA, Gill JC, Montgomery RR, Gill, JC: Type 2M:Milwaukee-1 von Willebrand disease: An in-frame deletion in the Cys509-Cys695 loop of the von Willebrand factor A1 domain causes deficient binding of von Willebrand factor to platelets. Blood 88:2559, 1996 14. Rabinowitz I, Tuley EA, Mancuso DJ, Randi AM, Firkin BG, Howard MA, Sadler JE: von Willebrand disease type B: A missense mutation selectively abolishes ristocetin-induced von Willebrand factor binding to platelet glycoprotein Ib. Proc Natl Acad Sci USA 89:9846, 1992 15. Abildgaard CF, Suzuki Z, Harrison J, Jefcoat K, Zimmerman TS: Serial studies in von Willebrand’s disease: Variability versus ‘‘variants’’. Blood 56:712, 1980 16. Zimmerman TS, Hoyer LW, Dickson L, Edgington TS: Determi- TYPE 2M VON WILLEBRAND DISEASE nation of the von Willebrand’s disease antigen (factor VIII-related antigen) in plasma by quantitative immunoelectrophoresis. J Lab Clin Med 86:152, 1975 17. Ruggeri ZM, Zimmerman TS: Variant von Willebrand’s disease: Characterization of two subtypes by analysis of multimeric composition of factor VIII/von Willebrand factor in plasma and platelets. J Clin Invest 65:1318, 1980 18. Ruggeri ZM, Zimmerman TS: The complex multimeric composition of factor VIII/von Willebrand factor. Blood 57:1140, 1981 19. Kroner PA, Kluessendorf ML, Scott JP, Montgomery RR: Expressed full-length von Willebrand factor containing missense mutations linked to type IIB von Willebrand disease shows enhanced binding to platelets. Blood 79:2048, 1992 20. Bonthron D, Orr EC, Mitsock LM, Ginsburg D, Handin RI, Orkin SH: Nucleotide sequence of pre-pro-von Willebrand factor cDNA. Nucleic Acids Res 14:7125, 1986 21. Mancuso DJ, Tuley EA, Westfield LA, Worrall NK, SheltonInloes BB, Sorace JM, Alevy YG, Sadler JE: Structure of the gene for human von Willebrand factor. J Biol Chem 264:19514, 1989 22. Mancuso DJ, Tuley EA, Westfield LA, Lester-Mancuso TL, Le Beau MM, Sorace JM, Sadler JE: Human von Willebrand factor gene and pseudogene: Structural analysis and differentiation by polymerase chain reaction. Biochemistry 30:253, 1991 23. Felgner PL, Gadek TR, Holm M, Roman R, Chan HW, Wenz M, Northrop JP, Ringold GM, Danielson M: Lipofection: A highly efficient, lipid-mediated DNA transfection procedure. Proc Natl Acad Sci USA 84:7413, 1987 24. Montgomery RR, Kunicki TJ, Glode LM: Use of monoclonal antibody to increase the sensitivity and specificity of precipitating immunoassays and cell surface binding immunoassays. Methods Enzymol 121:702, 1986 25. Raines G, Aumann H, Sykes S, Street A: Multimeric analysis of von Willebrand factor by molecular sieving electrophoresis in sodium dodecyl sulphate agarose gel. Thromb Res 60:201, 1990 26. Scott JP, Montgomery RR: The rapid differentiation of type IIb von Willebrand disease from platelet-type (pseudo-) von Willebrand disease by the ‘‘neutral’’ monoclonal antibody binding assay. Am J Clin Pathol 96:723, 1991 27. Schullek J, Jordan J, Montgomery RR: Interaction of von Willebrand factor with human platelets in the plasma milieu. J Clin Invest 73:421, 1984 28. Andrews RK, Booth WJ, Gorman JJ, Castaldi PA, Berndt MC: Purification of botrocetin from Bothrops jararaca venom. Analysis of the botrocetin-mediated interaction between von Willebrand factor and the human platelet membrane glycoprotein Ib-IX complex. Biochemistry 28:8317, 1989 29. Kawai Y, Montgomery RR: Endothelial cell processing of von Willebrand proteins. Ann N Y Acad Sci 509:60, 1987 30. Lee JO, Rieu P, Arnaout MA, Liddington R: Crystal structure of the A domain from the alpha subunit of integrin CR3 (CD11b/CD18). Cell 80:631, 1995 31. Qu A, Leahy DJ: Crystal structure of the I-domain from the CD11a/CD18 (LFA-1, alpha L beta 2) integrin. Proc Natl Acad Sci USA 92:10277, 1995 32. Bowie JU, Luthy R, Eisenberg D: A method to identify protein sequences that fold into a known three-dimensional structure. Science 253:164, 1991 33. Dudek MJ, Ponder JW: Accurate modeling of the intramolecular electrostatic energy of proteins. J Comp Chem 16:791, 1995 1581 34. Vriend G: WHAT IF: A molecular modeling and drug design program. J Mol Graph 8:52, 1990 35. Vriend G, Sander C: Detection of common three-dimensional substructures in proteins. Proteins 11:52, 1991 36. Vriend G, Sander C: Quality control of protein models: Directional atomic contact analysis. J Appl Cryst 26:47, 1993 37. Ruggeri ZM, Ware J: The structure and function of von Willebrand factor. Thromb Haemost 67:594, 1992 38. Sadler JE: von Willebrand factor. J Biol Chem 266:22777, 1991 39. Berndt MC, Ward CM, Booth WJ, Castaldi PA, Mazurov AV, Andrews RK: Identification of aspartic acid 514 through glutamic acid 542 as a glycoprotein Ib-IX complex receptor recognition sequence in von Willebrand factor. Mechanism of modulation of von Willebrand factor by ristocetin and botrocetin. Biochemistry 31:11144, 1992 40. Sadler JE, Ginsburg D: A database of polymorphisms in the von Willebrand factor gene and pseudogene. Thromb Haemost 69:185, 1993 41. Cruz MA, Yuan H, Lee JR, Wise RJ, Handin RI: Interaction of the von Willebrand factor (vWF) with collagen. Localization of the primary collagen binding site by analysis of recombinant vWF a domain polypeptides. J Biol Chem 270:10822, 1995 42. Denis C, Baruch D, Kielty CM, Ajzenberg N, Christophe O, Meyer D: Localization of von Willebrand factor binding domains to endothelial extracellular matrix and to type VI collagen. Arterioscler Thromb 13:398, 1993 43. Meyer D, Fressinaud E, Gaucher C, Lavergne JM, Hilbert L, Ribba AS, Jorieux S, Mazurier C, the INSERM Network on Molecular Abnormalities in von Willebrand Disease: Gene defects in 150 unrelated French cases with type 2 von Willebrand disease: From the patient to the gene. Thromb Haemost 78:451, 1997 44. Brandeen CI: Relation between structure and function of alpha/ beta-proteins. Q Rev Biophys 13:317, 1980 45. Celikel R, Varughese KI, Madhusudan A, Yoshioka A, Ware J, Ruggeri ZM: Crystal structure of von Willebrand factor A1 domain in complex with the function blocking NMC-4 Fab. Thromb Haemost 769:HI-9, 1997 (abstr) 46. Ginsburg D, Sadler JE: von Willebrand disease: A database of point mutations, insertions, and deletions. For the Consortium on von Willebrand Factor Mutations and Polymorphisms, and the Subcommittee on von Willebrand Factor of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Thromb Haemost 69:177, 1993 47. Sugimoto M, Mohri H, McClintock RA, Ruggeri ZM: Identification of discontinuous von Willebrand factor sequences involved in complex formation with botrocetin. A model for the regulation of von Willebrand factor binding to platelet glycoprotein Ib. J Biol Chem 266:18172, 1991 48. Matsushita T, Sadler JE: Identification of amino acid residues essential for von Willebrand factor binding to platelet glycoprotein Ib. Charged-to-alanine scanning mutagenesis of the A1 domain of human von Willebrand factor. J Biol Chem 270:13406, 1995 49. Kroner PA, Frey AB: Analysis of the structure and function of the von Willebrand factor A1 domain using targeted deletions and alaninescanning mutagenesis. Biochemistry 35:13460, 1996 50. Girma JP, Takahashi Y, Yoshioka A, Diaz J, Meyer D: Ristocetin and Botrocetin involve two distinct domains of von Willebrand Factor for binding to platelet membrane glycoprotein Ib. Thromb Haemost 64:326, 1990