OP ID* ______________ CERNER SECURITY REQUEST FORM o
advertisement

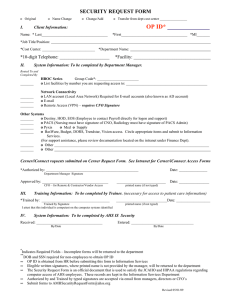
CERNER SECURITY REQUEST FORM I. OP ID* ______________ Client Information: Type: o Original o Add o Change o Transfer o Name Change Name: Last___________________________________ First___________________________________ MI_______ Job Title/Position: ________________________________ Cost Center: ____________________________ Credentials: __________ (e.g. RN, COTA; required for Cerner) Department Name: 10-digit Telephone: ______________________ DOB: ________________________ (required for Cerner) Home Entity: ___________________________ SSN: ____________________________ (required for Cerner) Access needed to the following Entities (check all that apply): o Adventist Bolingbrook II. o Adventist Hinsdale o Adventist GlenOaks o Adventist La Grange Memorial System Information: To be completed by Department Manager. Application: ____________________________ Position:___________________________ Toggle Requests: If this user needs access to more than one position, please list any additional position/s here: _________________________________________________________________________________________ Please indicate if any of the following are required: □ □ □ □ Outreach Organizations FirstNet Properties SurgiNet Properties Scheduling Keys A list of the available positions is available by selecting the Clinical/Medical section on the Intranet (under iConnect Resources/Cerner Security Positions List) III. Authorization and Training Information: Legible Signatures are REQUIRED for Cerner Access Authorized by: _________________________________________________ Date: ______________________ Department Manager (print name and then sign) Approved by: ___________________________________________________ Date: ______________________ CFO – for Remote & Contractor/Vendor Access Trained by: ___________________________________________________ Date: ______________________ I attest that this individual is competent on the computer systems identified. Please submit last page of completed competency with this form. ∞ ∞ ∞ This document is official and provides verification of compliance with state and federal laws governing privacy and security. Illegible signatures and incomplete forms will be returned to the department. Authorized by and Trained by signatures can be typed and then sent via e-mail if sent by the department manager, department assistant, or the departmental trainer. For Office Use Only: Date Request Received: ________________ Received By: ______________________________________ Date Access Initiated/Modified: _____________ Date of Termination from System: ____________________ Send Completed Form to Becky Rossi in Corporate Compliance; Fax: 630.856.4522; Email: Rebecca.Rossi@ahss.org