8
advertisement

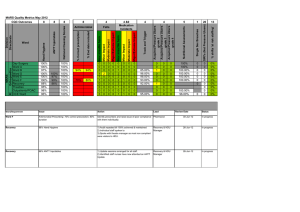
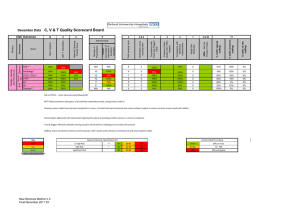
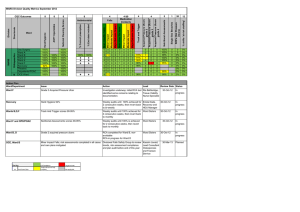
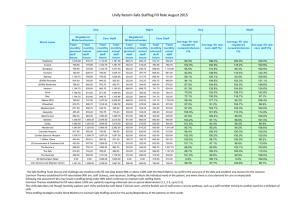
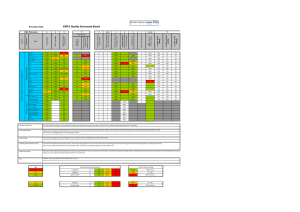
100% 6A * 100% 100% 5D* Theatres** 100% 100% 100% 98% 89% 69% 85% 90% 0 0 0 90% 0 0 0 1 0 0 100% 0 0 0 0 0 0 % shifts 'at risk staffing' 100% 85% 0 % shifts 'minimum staffing' CTW * 92% 0 13 % shifts 'agreed staffing' 96% 4 & 20 SIRIs Not Incl Pressure Ulcers 97% 91% 1 Single Sex Breaches 100% 100% 5 Compliance with Nutritional Assessments 100% CTCC / CCU** 4 Pressure Ulcers Grade 2/3/4 / Skin Integrity Cardiology * 4 Compliance with Track and Trigger / EWS 91% 4&9 Medication errors causing harm 100% Antimicrobial 4 Falls causing harm 100% Ward 8 % End date included National Cleaning Overall Score 8 ANTT Injectables 8 Hand Hygiene 8 CAS ** Directorate Medicine Surg & Vasc PP Cardiac, Vascular and Thoracic (3) Division CQC Outcomes C, V & T Quality Scorecard Board % Correct prescription July Data 0 0 14% 86% 0% 100% 0 0 70% 30% 0% 100% 0 0 50% 49% 1% 0 100% 0 0 25% 67% 8% 90% 0 100% 0 0 94% 1% 3% 100% 0 100% 0 0 0 41% 100% 56% 0% 3% 0% Action Plan National Cleaning scores: CAS - Re-audit by Matron and infection control. All failures related to Carillion with exception of BP cuffs. At the time of re-audit, no rectifications had been made so escalated through Carillion management structure and monitored by unit Sister. 6A: On re-audit almost all failures had been corrected. All failing items were Carillion responsibilities and may be due to the ward’s usual cleaner being on annual leave. The Matron has written to Carillion, highlighting the importance of this ward having a regular replacement cleaner. Antimicrobial prescribing: Discussion held at CSU Directorate and Divisional meeting and reinforced to new F1s during induction. Pressure Ulcers: Community acquired grade 2 pressure ulcer which developed into grade 3 in a high risk patient. At risk staffing: staff moved across the division and temporary staff used to ensure patient safety. National Cleaning Specification (%) Key 1 Antimicrobial Prescribing Poor V. High Risk ** >95 90-95 <90 Green Fair High Risk * >92 87-92 <87 Amber 80% or more 70 - 79% Good Significant Risk >85 80-85 <80 Red 69% and below July Data C & W Quality Scorecard Board % shifts 'minimum staffing' % shifts 'at risk staffing' 100% 0 0 93% 85% 85% 0 0 100% 0 95% 0 0 100% 0% 0% 100% 94% 0 0 91% 82% 82% 0 0 100% 0 90% 0 0 96% 4% 0% Childrens Ambulatory Care 95% 100% 0 0 92% 0 0 N/A 0 0 0 50% 50% 0% HGH Childrens W * Bel / Dray * Kamrans ** Melanies * NNU** SCBU** PHDU** PICU** 100% 95% 0 0 95% 92% 100% 0 0 90% Catheter on going care 100% Ward Catheter Insertion % shifts 'agreed staffing' 13 SIRIs Not Incl Pressure Ulcers 4 & 20 Single Sex Breaches 1 Compliance with Nutritional Assessments 5 Pressure Ulcers Grade 2/3/4 / Skin Integrity 4 Compliance with Track and Trigger / EWS 4 Total No of medication errors that did harm 4&9 Total No of Accidents that did harm 4 % End date included 8 % Correct prescription 8 National Cleaning Overall Score 8 C-Diff post 72 hrs 8 MRSA / MSSA post 48 hrs 8 Saving Lives Catheter Care ANTT Injectables 8 Hand Hygiene 8 Toms * Robins * Directorate Paediatrics Paediatric Critical Children's Division CQC Outcomes Antimicrobial 87% 87% 0 0 80% 0 100% 0 0 100% 1% 0% 0 0 100% 0 100% 0 0 96% 4% 0% 98% 99% 0 0 95% n/a n/a 0 0 100% 0 90% 0 0 84% 16% 0% 100% 97% 0 0 92% 100% 100% 0 0 80% 0 100% 1 0 94% 6% 0% 100% 99% 0 0 91% 100% 100% 0 0 n/a 0 0 0 99% 1% 0% 100% 100% 0 0 96% 100% 100% 0 0 n/a 0 0 0 100% 0% 0% 95% 98% 100% 100% 0 0 0 0 95% 95% 100% 100% 100% 100% 0 0 0 0 n/a n/a 0 0 0 0 0 0 100% 100% 0% 0% 0% 0% Action Plan Staffing : Ambulatory Care - staffing optimal for 50% of the time and staff moved from other areas in CHOX as part of Summer Plans to manage safety at all other times Key Poor Fair Good National Cleaning Specification (%) V. High Risk High Risk Significant Risk Page 2 of 9 ** * >95 >92 >85 Antimicrobial Prescribing 90-95 87-92 80-85 <90 <87 <80 Green Amber Red 80% or more 70 - 79% 69% and below % shifts 'agreed staffing' % shifts 'minimum staffing' % shifts 'at risk staffing' SIRIs Not Incl Pressure Ulcers 13 Single Sex Breaches 4 & 20 Compliance with Nutritional Assessments 1 Compliance with Track and Trigger / EWS 5 Total No of medication errors that did harm 4 Total No of Falls That did harm 4 % End date included 4&9 % Correct prescription 4 National Cleaning Overall Score 8 ANTT Injectables 8 Hand Hygiene 8 JR Gynae* 100% 100% 89% 100% 100% 0 0 100% 100% n/a 100% 0% 0% HGH Gynae* 100% 96% 0 0 n/a 100% 0% 0% Gynae Scrub 87% 94% 0 0 n/a 100% 0% 0% Gynae A & R Maternity Theatres 91% 94% 94% 0 0 0 0 n/a 100% 100% 0% 0% 0% 0% Delivery Suite / Obs 100% 94% 0 0 100% 0% 0% 95% 0 0 100% 0% 0% 0 0 100% 0% 0% 0 0 100% 0% 0% 0 0 100% 0% 0% 0 0 0 0 100% 100% 0% 0% 0% 0% Directorate Gynae 8 Ward Spires Midwifery Led Maternity Gynae and Maternity Division CQC Outcomes Pressure Ulcers Grade 2/3/4 / Skin Integrity Gynae and Maternity Quality Scorecard Board July Data 100% Level 5 66% 96% Level 6 100% 93% Level 7 Antimicrobial NA NA 93% HGH Delivery Suite HGH Post Natal Ward 90% Action Plan JR Gynae: fortnightly cleaning and inspection rounds have commenced with Carillion fully engaged in the process. Supervisor presence has been increased. Women's Theatres: great improvement in hand hygiene but still under target. Daily audits are to continue. Falls: One recorded fall (but no harm) occurred at the HGH and was the partner of the patient who was taking painkillers and had not eaten. Hand hygiene audit on Level 5 - Small number of staff involved [ 1 midwife] this was addressed with individual concerned Key Poor Fair Good New Structure Metrics V.2 Final November 2011 SY V. High Risk High Risk Significant Risk National Cleaning Specification (%) ** * >95 >92 >85 90-95 87-92 80-85 <90 <87 <80 Green Amber Red Antimicrobial Prescribing 80% or more 70 - 79% 69% and below EMTA Quality Scorecard Board 4&9 4 4 5 1 4 & 20 0 0 100% 0 100% 0 0 100% 0 100% 91% 1 0 100% 94% 82% 82% 1 0 91% 80% 80% 0 100% ND 91% 82% 100% 92% 85% 69% 100% na PAU * 100% Oak * 0 93% 7% 0% 0 0 73% 27% 0% 0 0 100% 0% 0% 100% 0 0 68% 32% 0% 0 100% 0 0 57% 37% 6% 100% 1 100% 0 0 72% 27% 1% 0 100% 0 100% 0 0 71% 19% 10% 1 0 100% 0 100% 0 0 63% 27% 10% 0 0 100% 0 100% 0 0 70% 30% 0% 94% 0 0 0 0 78% 14% 8% 0% 92% 0 0 0 0 80% 15% 5% 100% 89% 93% 93% 93% 1 0 96% 0 100% 0 0 93% 7% 0% Laburnam * 100% 100% ND 90% 80% 0 0 92% 0 100% 0 0 88% 12% 0% Juniper * 100% 100% ND 0 0 100% 0 100% 0 0 69% 31% 0% Level 4 * 100% 100% 95% 0 100% 0 100% 0 0 85% 15% 0% ASU * 92% 100% 91% 0% John Warin ** 95% 100% Geoffrey Harris * 100% Treatment Centre Dermatology National Cleaning Overall Score 0 100% ANTT Injectables % shifts 'at risk staffing' 0 % shifts 'minimum staffing' 0 100% % shifts 'agreed staffing' 100% 0 SIRIs Not Incl Pressure Ulcers 0 1 Single Sex Breaches 0 13 Compliance with Nutritional Assessments Hospital acquired Pressure Ulcers Grade 2/3/4 / Skin Integrity 4 Compliance with Track and Trigger / EWS 8 Total No of medication errors that did harm 8 Total No of Falls that did Harm 8 JR ED ** 86% 75% 96% JR EAU * 100% 100% ND HGH ED ** 92% 100% 94% HGH MAU * 100% 100% ND 100% 7A * 100% 100% 93% 7B * 100% 100% 7C * 100% 100% 7D * 100% 7F* 100% 5A * % End date included Ward Antimicrobial % Correct prescription Directorate Emergency Medicine Ambulatory, Chest, ID Division Emergency Medicine, Therapies & Ambulatory (7) 8 Hand Hygiene July Data CQC Outcomes 82% 45% 100% 94% 0 0 0 92% 0 94% 2 0 95% 5% 95% 100% 86% 0 0 100% 0 96% 0 0 57% 34% 9% 100% 92% 100% 100% 0 0 80% 0 100% 0 0 10% 75% 15% 100% 100% 83% 0 0 0 100% 0% 92% 0 0 0 0 Immunology 100% 100% NA 0 0 0 0 OCDEM Endocrine 100% 0% NA 0 0 0 0 OCDEM Diabetes N/A 0% NA 0 0 0 0 Sleep Physiology N/A 0% NA 0 0 0 0 GUM Genetics 0 0 100% 0% NA 0 0 0 0 N/A 0% NA 0 0 0 0 Action Plan Clinically Justifiable Single sex breachs: Stroke Unit (5B) - 2 single sex breaches affecting 8 patients to ensure patients received care in appropriate environment to receive specialist care care. Antimicrobial: EAU JR, Antimicrobial medical prescribing issue low end date data - To be reviewed in medical directorate and at medical governance, that ward manager has identified an audit error that would account for low scoring. 7F -This issue will be highlighted to the Clinical Lead and the next Unit meeting. Pressure ulcers: 7B - 1 patient developed a pressure ulcer, grade 2 despite all pressure relief management in place Key Poor Fair Good New Structure Metrics V.2Final November 2011 SY National Cleaning Specification (%) ** >95 V. High Risk * >92 High Risk >85 Significant Risk 90-95 87-92 80-85 <90 <87 <80 Green Amber Red Antimicrobial Prescribing 80% or more 70 - 79% 69% and below 5 1 4 & 20 13 % shifts 'minimum staffing' 4 94% 100% 100% 0 0 100% 0 100% 1 0 100% 0% 0% 100% 84% 100% 100% 1 0 100% 0 100% 0 0 82% 15% 3% not done % shifts 'at risk staffing' 100% 100% % End date included 80% Neurosciences IP * Ward % Correct prescription % shifts 'agreed staffing' National Cleaning Overall Score 4 SIRIs Not Incl Pressure Ulcers ANTT Injectables 4&9 Single Sex Breaches Hand Hygiene Combined 4 Compliance with Nutritional Assessments 8 Antimicrobial Pressure Ulcers Grade 2/3/4/ Skin Integrity 8 Compliance with Track and Trigger / EWS 8 Total No of medication errors that did harm 8 NICU ** Directorate Neuro Trauma Specialist Surgery Neuro, Trauma, Specialist Surgery (3) Division CQC Outcomes Total No of Falls that did harm NTSS Quality Scorecard Board July Data Neurosciences OPD 100% 0 100% 0% 0% 2A * 100% 100% not done 100% 100% 0 0 100% 2 96% 0 0 59% 32% 9% 3A * 100% 100% 92% 100% 100% 0 0 100% 4 90% 0 0 56% 42% 2% Trauma OPD 98% 0 80% 20% 0% F Ward * 95% 100% 96% 70% 90% 0 0 96% 5 90% 0 0 81% 17% 2% SSIP * 100% 100% 97% 100% 100% 0 0 100% 0 90% 0 0 96% 4% 0% Lichfield * 100% n/a 88% 0 98% 2% 0% SSOPD 100% no audit 0 90% 10% 0% OPD Eye OMFS OPD 100% 100% 90% not done 0 0 80% 14% 20% 36% 0% 50% not done Action Plan Neurosciences - Fall - this is being investigated as an orange incident and a meeting has been arranged to review the case and this will be reported to the September Clinical Governance Committee. Pressure Ulcers Trauma wards - 1 category 4 ulcer which patient was admitted with. All other ulcers were category 2, of which 5 were discovered on admission and 5 developed whilst admitted. Trauma Tissue Viability Nurse has reviewed the cases and is incorporating them as case studies into the Trauma teaching Schedule. Staffing OMFS OPD - this is a small team, whilst they are waiting for recruited staff to start Sister is monitoring closely and will report back any concerns to Matron. Cleaning audits are discussed in the infection control section of the quality paper. The Divisional Nurse attended the latest audit on neurosciences and is monitoring closely with Carillion and infection control. Matron is addressing concerns with Carillion managers regarding Lichfield. One clinically justified single sex breach on NICU due to delay in discharge to the ward and patient acutiy improved Key Poor Fair Good Metrics V.2 Final SYNov 11 National Cleaning Specification (%) V. High Risk High Risk Significant Risk ** * >95 >92 >85 Antimicrobial Prescribing 90-95 87-92 80-85 <90 <87 <80 Green Amber Red 80% or more 70 - 79% 69% and below Directorate Division Metrics V.2 Final SYNov 11 8 8 National Cleaning Overall Score Antimicrobial 4&9 4 4 5 1 4 & 20 Total No of medication errors that did harm Compliance with Track and Trigger / EWS Pressure Ulcers Grade 2/3/4/ Skin Integrity Compliance with Nutritional Assessments Single Sex Breaches SIRIs Not Incl Pressure Ulcers % shifts 'at risk staffing' % shifts 'minimum staffing' % shifts 'agreed staffing' 4 Total No of Falls that did harm % End date included % Correct prescription 8 ANTT Injectables Ward 8 Hand Hygiene Combined CQC Outcomes 13 0 0 93% 6% 1% 60% 0 0 73% 27% 0% 0 100% 0 0 55% 45% 0% 100% 1 90% 0 0 87% 4% 9% 100% 0 100% 0 0 87% 13% 0% 0% 100% 97% 96% 100% 85% 0 0 100% 93% 100% 95% 98% 94% 0 0 100% Sobell * 100% N/A 91% 91% 100% 0 0 100% SEU D & Triage* 90% 95% 92% 100% 100% 1 0 SEU E 98% 77% 86% 100% 100% 0 0 Hand Hygiene Compliance with Track and Trigger / EWS 100% Total No of medication errors that did harm 1 Oncology Ward ** % End date included 13 % shifts 'at risk staffing' 4 & 20 % shifts 'minimum staffing' 1 % shifts 'agreed staffing' 5 SIRIs Not Incl Pressure Ulcers 4 Single Sex Breaches 4 Compliance with Nutritional Assessments 4&9 Pressure Ulcers Grade 2/3/4/ Skin Integrity 4 Total No of Falls that did harm 8 Antimicrobial National Cleaning Overall Score In Patient Wards 8 Haematology ** Division Clinical Areas 8 % Correct presciption Ward Surgery & Oncology (6) 8 ANTT Injectables S & O Quality Scorecard Board July Data CQC Outcomes SEU F * 87% 95% 91% 100% 100% 0 0 100% 0 100% 0 0 87% 13% 5F * 100% 95% 90% 100% 100% 0 0 100% 0 95% 0 0 69% 27% 4% HGH E Ward * 96% 95% 91% 100% 70% 0 0 100% 0 100% 0 0 90% 8% 2% 1% UGI * 92% 80% 92% 100% 100% n/a 0 100% 0 80% 0 0 77% 22% Colorectal * 100% 75% 92% 73% 100% 0 0 100% 0 80% 0 0 99% 0% 1% Jane Ashley * 100% 100% 92% 100% 100% 0 0 100% 0 100% 0 0 85% 13% 2% Urology * 90% 100% 94% 90% 90% 0 0 80% 0 100% 0 0 90% 7% 3% Transplant ** Renal Ward ** 88% 89% 97% 80% 93% 91% 100% 100% 96% 90% 0 0 0 0 100% 90% 0 0 90% 89% 0 0 0 0 93% 58% 4% 37% 3% 5% Oxford Man Unit* 100% 100% 94% 0 0 0 0 Oxford Tarver Dialysis* 100% 100% 90% 0 0 0 Stoke Mandeville * 89% 100% 0 0 0 0 90% 10% 0% Milton Keynes * 98% 90% 0 0 0 0 50% 45% 5% 0% 95% 5% 0% 100% 0% 0% Swindon * 100% 100% 0 0 0 0 95% 5% Wycombe * 85% 100% 0 0 0 0 100% 0% 0% Th Churchill ** Th TDA / DCU * 85% 92% 87% 0 0 0 0 0 0 1 0 85% 95% 13% 5% 2% 0% 99% 83% 1% 14% 0% 3% 91% 94% Oncology Treatment 90% 100% 91% 0 0 0 0 Brody Centre HGH 90% 100% 93% 0 0 0 0 0 Triage 90% 100% 92% 0 0 N/A Research 100% 100% 92% 0 0 0 0 JR Endoscopy ** HGH Endoscopy ** 96% 100% 93% 100% 89% 95% 0 0 0 0 0 0 0 0 Action Plan Nutritional Assessments: An improvement on last month however the Matrons continue to work closely with ward sisters and nursing teams by auditing results weekly and feeding back results and actions via team meetings. Ward cleaning scores: An improvement this month. Action: Matrons continue to attend each ward audit and feeds back immediately to staff all issues raised. Cleaning on wards being monitored weekly. Hand hygiene results have improved however matrons recognise need to monitor ANTT results which are variable again this month. Focus now on challenging unacceptable practice to educate staff. There were two pressure ulcers that developed whilst patients were in-patients last month. RCA has been undertaken in both cases and the need to document inspection of skin on admission has been highlighted in both cases. This learning has been shared throughout the Division. Key Poor Fair Good New Structure Metrics V.1Final August 2011 SY National Cleaning Specification (%) ** >95 V. High Risk * >92 High Risk Significant Risk >85 90-95 87-92 80-85 <90 <87 <80 Green Amber Red Antimicrobial Prescribing 80% or more 70 - 79% 69% and below 5 1 4 & 20 Pressure Ulcers Grade 2/ 3/4 / Skin Integrity 13 % shifts 'minimum staffing' 4 75% 96% 100% 100% 0 0 1 100% 10 0 100% 0% 0% 81% 75% 97% 100% 100% 0 0 2 100% 2 0 100% 0% 0% HGH CICU ** 86% 100% 94% 0 0 0 100% 13 0 100% 0% 0% HGH DCU * N/A N/A 0 0 0 100% 0 0 100% 0% 0% Th West Wing ** 78% N/A 96% 0 0 0 0 0 100% 0% 0% Th JR ** Th HGH ** 77% N/A 74% N/A 95% N/A 0 0 0 0 0 0 0 0 0 0 100% 100% 0% 0% 0% 0% % Correct % End date presciption included Action Plan Deputy Matron attending new medical staff induction to highlight importance of hand hygiene in critical care. ANTT low due to agency staff not being aware of the equired best practice. ANTT demonstrated and taught to all new agency staff on unit. Pressure ulcers : two in AICU/CICU from patients admitted with grade 2 sores. One in CICU grade 2 sore in corner of mouth due to Endo Tracheal Tube (ETT). Staff reminded of importance in changing sides of ETT during change of tapes. Clinically Justified single sex breaches are reported internally and to the PCT- due to short delays in transferring from a specialised environment to a ward environment Key Poor Fair Good New Structure Metrics V.2Final November 2011 SY National Cleaning Specification (%) V. High Risk High Risk Significant Risk ** * >95 >92 >85 Antimicrobial Prescribing 90-95 87-92 80-85 <90 <87 <80 Green Amber Red 80% or more 70 - 79% 69% and below % shifts 'at risk staffing' 84% Antimicrobial % shifts 'agreed staffing' AICU ** Ward Hand Hygiene SIRIs Not Incl Pressure Ulcers 4 Single Sex Breaches 4&9 Compliance with Nutritional Assessments 4 Total No of medication errors that did harm 8 Total No of Falls that did harm 8 National Cleaning Overall Score 8 ANTT Injectables 8 CICU ** Directorate Anaes / CC / Th Critical Care, Theatres, Diagnostics & Division CQC Outcomes Compliance with Track and Trigger / EWS CCTDP Quality Scorecard Board July Data 1 4 & 20 SIRI's (Not Pressure Ulcers) 13 % shifts 'at risk staffing' 5 Single Sex Breaches Acquired Pressure Ulcers grade 4 Acquired Pressure Ulcers grade 3 4 Acquired Pressure Ulcers grade 2 Track and Trigger 4 Major/Extreme Impact Moderate Impact Minor Impact Medication Incidents Near miss/ No harm Falls Major/Extreme Impact Antimicrobial Moderate Impact 4 &9 Minor Impact 4 Near miss/No harm 8 % End date included 8 % Correct presciption Hand Hygiene Ward 8 National Cleaning Scores 8 ANTT Injectables Directorate Orthopaedics Re MARS Division CQC Outcomes Nutritional Assessments MARS Quality Metrics July 2012 Day Surgery 100% 100% 0 0 0 0 1 0 0 0 0 0 0 100% 0 0 0% Ward A Ward B 100% 93% 96% 100% 100% 0 3 0 0 0 0 0 0 0 3 0 0 0 0 0 0 90.00% 0 0 0 0 0 0 100% 88.00% 0 0 0 0 0% 0% Ward D Ward E 100% 100% 100% 100% 100% 100% 1 1 0 1 0 0 0 0 1 1 0 0 0 0 0 0 92.00% 93.00% 0 0 0 0 0 0 100.00% 90.00% 0 0 0 0 0% 0% Ward F 87% 100% 100% 3 0 0 0 0 0 0 0 89.00% 1 0 0 86.00% 0 0 0% Recovery 100% 98% 100% 0 0 0 0 1 1 0 0 97.00% 0 0 0 0 0 0% 100% 81% 80% 80% Theatres 93% 100% 0 0 0 0 1 0 0 0 0 0 0 Outpatients/POAC 100% 100% 0 0 0 0 0 1 0 0 0 0 0 92.00% OCE Ward 80% 100% 0 2 0 0 0 0 0 0 0 0 0 88.00% Action Plan Ward/Department Issue 95.00% Action Lead 0 Review Date 0 0% 0 0% 0 0% Status Ward F 87% Overall Hand Hygiene compliance; this includes:100% Discuss poor compliance in the medical and Vicky Wren, Ward F compliance for nursing staff; 73% compliance for doctors; therapy teams with the Clinical Director and Sister 83% compliance for AHP. therapy team leaders; try to obtain names of individual involved; re-audit weekly until 100 achieved and maintained for 2 consecutive weeks 31-Aug-12 In progress OCE Ward 80% Overall Hand Hygiene compliance; this includes:80% Raise poor compliance at ward meetings and compliance for nursing staff; 100% compliance for doctors; NRS Governance; weekly audits until 100% 100% compliance for AHP. compliance achieved and maintained for 2 consecutive weeks 31-Aug-12 In progress Sue Hunt, Ward Sister