Document 11364550
advertisement

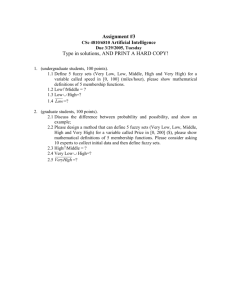
Int J CARS (2011) 6 (Suppl 1):S305–S366 DOI 10.1007/s11548-011-0613-1 COMPUTER ASSISTED RADIOLOGY - 25TH INTERNATIONAL CONGRESS AND EXHIBITION Quantification of periarticular demineralization in rheumatoid arthritis by digital X-ray radiogrammetry (DXR) and peripheral quantitative computed tomography (pQCT) D.M. Renz1, A. Pfeil2, A. Hansch3, G. Wolf 2, J. Böttcher4 1 Charité University Medicine Berlin, Department of Radiology, Berlin, Germany 2 Friedrich-Schiller-University Jena, Department of Internal Medicine III, Jena, Germany 3 Friedrich-Schiller-University Jena, Institute of Diagnostic and Interventional Radiology, Jena, Germany 4 SRH Waldklinikum Gera, Institute of Diagnostic and Interventional Radiology, Gera, Germany Keywords DXR Rheumatoid arthritis Peripheral quantitative computed tomography Bone mineral density Purpose Rheumatoid arthritis as a chronic and inflammatory disease of the hand is associated with a periarticular bone loss [1, 2]. Advances in established techniques and the implementation of new computer-aided diagnosis (CAD) methods in the field of osteodensitometry have widened the spectrum of diagnostic tools available for assessing bone mineral density (BMD) in different body regions. The most established techniques used for estimating BMD in the routine clinical setting include quantitative computed tomography, quantitative ultrasound, and dual-energy X-ray absorptiometry (DXA). Digital X-ray radiogrammetry (DXR) is a recently developed CAD tool for automatically assessing cortical mineralization. The aim of this study was to evaluate changes of bone mineral density using the radiogrammetrically based densitometric technology (DXR) in patients suffering from rheumatoid arthritis and to compare this technique with findings of peripheral quantitative computed tomography (pQCT). Methods Ninety patients with a verified RA, following the criteria of the American College of Rheumatology [3], underwent a prospective analysis of their BMD. Bone mineralization was assessed using DXR and pQCT. Digital X-ray radiogrammetry (DXR, Pronosco X-Posure SystemTM, Version 2.0; Sectra, Linköping, Sweden) was applied to quantify bone mineral density (BMD in g/cm2) based on radiographs of the hand in an anterior-posterior projection. The radiographs were digitized by a scanner. CAD analysis was performed without user interaction. DXR-BMD was measured on the three middle metacarpals. To locate the diaphysis of the metacarpals in the radiographs, Pronosco X-posure used a well-established model-based algorithm known as the active shape model (ASM). After each diaphysis had been identified, the computer algorithm automatically defined regions of interest (ROIs) for measurements at the narrowest parts of the diaphysis of the index, middle, and ring finger metacarpals. PQCTBMD (Version 3.3; Stratec Medizintechnik GmbH, Pforzheim, Germany) was calculated of the distal radius and differentiated in total, trabecular, and cortical BMD. The clinical severity of RA was assessed using the Larsen Score. Results The mean value of DXR-BMD decreased from 0.57 g/cm2 ± 0.08 (Larsen Score 1) to 0.45 g/cm2 ± 0.11 (Larsen Score 5). The relative decrease of BMD measured by DXR between the highest and the lowest score was 20% (p \ 0.05). The relative decrease of BMD (pQCT) from Larsen Score 1 to Score 5 also showed a significant result regarding pQCT-BMD (trabecular; as the most metabolic active bone tissue) with 16% (p \ 0.05). No significant changes in the demineralization were confirmed for pQCT-BMD (total) with 12% and for pQCT-BMD (cortical) with 2%. Conclusion The development of computer-based techniques has promoted the precise quantification of metacarpal bone mineral density as measured by digital X-ray radiogrammetry [4]. The study highlights that DXR is able to exactly measure cortical differences of bone mineralization in patients suffering from rheumatoid arthritis. This CAD technique seems to be able to reliably quantify disease-related periarticular loss of bone mineral density dependent on the severity of rheumatoid arthritis. Furthermore, the consideration of DXR parameters seems to be an outcome measure in RA and seems to allow an optimal planning and monitoring of therapeutic strategies of the disease [5]. References [1] Gravallese EM. Bone destruction in arthritis. Ann Rheum Dis 2002; 61: 84–86. [2] Goldring SR. Periarticular bone changes in rheumatoid arthritis: pathophysiological implications and clinical utility. Ann Rheum Dis 2009; 68: 297–299. [3] Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fies FJ, Cooper NS. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988; 31: 315–324. [4] Böttcher J, Pfeil A, Rosholm A, Petrovitch A, Seidl BE, Malich A, Schäfer ML, Kramer A, Mentzel HJ, Lehmann G, Hein G, Kaiser WA. Digital X-ray radiogrammetry combined with semiautomated analysis of joint space widths as a new diagnostic approach in rheumatoid arthritis: a cross-sectional and longitudinal study. Arthritis Rheum 2005; 52: 3850–3859. [5] Pfeil A, Haugeberg G, Hansch A, Renz DM, Lehmann G, Malich A, Wolf G, Böttcher J. The value of digital X-ray radiogrammetry in the assessment of inflammatory bone loss in rheumatoid arthritis. Arthritis Care Res (Hoboken). 2011 Jan 4 [Epub ahead of print]. Respiratory motion prediction by evolving connectionist system (ECOS) framework M. Kakar Oslo University Hospital, Division of Surgery and Cancer Medicine, Institute for Cancer Research, Department of Radiation Biology, Oslo, Norway Keywords Respiratory Motion prediction Evolving EFuNN DENFIS Purpose Respiratory motion prediction is a chaotic time series prediction problem. In this study, respiratory motion predictability from 10 123 S306 Int J CARS (2011) 6 (Suppl 1):S305–S366 traces from a lung cancer patient is examined by using two evolving fuzzy neural architectures. The main objective has been to test algorithms which can evolve with the breathing characteristics of the patient for online implementation. Methods Previous studies [1] have shown that popular Neural network models including Multilayer Percepron (MLP) and Adaptive Neuro Fuzzy Inference System (ANFIS) are good for modeling and predicting respiratory motion, however, they lack in on line learning and capability to evolve. These models operate on a fixed size connectionist structure, which limits its ability to accommodate new data, and may require much iteration for learning. In addition, it is required that the initialization parameters of the network be tested with multiple initial values. Such an approach is cumbersome and renders impractical especially for online implementations. As an alternative, evolving fuzzy neural architectures are becoming popular for online training [2]. These require much larger dataset for modeling and emphasizes on learning specific/local characteristics of the process rather than global characteristics. Breathing data curves were obtained from Real Time Position Management system (RPM system) from 10 traces from a single patient at different time intervals [3]. Two different methods in the evolving connectionist’s system framework (ECOS) including Dynamic Evolving neuro fuzzy inference system (DENFIS) and Evolving fuzzy neural network (EFuNN) were tested on our dataset for a 200 ms prediction interval. EFuNN is a five layered fuzzy neural network. EFuNN evolves according to ECOS principles. ECOS evolves structurally and functionally by interacting with the environment thereby better adapting to the incoming data. The nodes and connections in the layers in EFuNN are created or connected based upon the data samples being presented. In our simulations, we chose sensitivity threshold as 0.9 and Table 1 Average RMSE values for learning and validation for different architectures (1 step ahead prediction i.e. 200 ms) Average RMSE DENFIS EfuNN Training 21.15 8.66 Testing 21.51 4.84 error threshold as 0.4. Number of membership functions was taken to be 3. Learning rate for weights w1 and w2 was 0.1. DENFIS uses Takagi–Sugeno type fuzzy inference engine[4]. The inference engine here is composed of m rules. The learning mechanism relies on dynamically creating and updating fuzzy rules during the learning process. The fuzzy rules that participate in the inference for each of the existing input vector are dynamically chosen from the existing fuzzy rule set depending upon the position of the current input vector in the input space. In this study, after experimenting with different combinations, we found the best choices for Dthras 0.1 and number of epochs for training as 2. The number of nodes which are referenced to estimate the output of the current sample was chosen to be 3. Results EFuNN and DENFIS algorithms were tested on 10 traces of a respiratory motion sequences. Interval of the signal was chosen to be random in order to introduce generality for testing. Results obtained from simulation over 10 traces of data are listed in table 1.Results reveal root mean square error (RMSE) values to be 21.51 and 4.84 for prediction by DENFIS and EFuNN, respectively. Figure 1 shows a sample for prediction by EFuNN (continuous line) w.r.t. desired (dashed) output for a single trace with 1558 breathing samples. Conclusion EFuNN was found to have better performance than DENFIS on this dataset. References [1] Kakar M., Nystrom H., Aarup L.R., Nottrup T.J., and Olsen D.R., ‘‘Respiratory motion prediction by using the adaptive neuro fuzzy inference system (ANFIS),’’ Phys. Med. Biol., vol. 50, no. 19, pp. 4721–4728, 2005. [2] Watts M.J., ‘‘A decade of Kasabov’s evolving connectionist systems: A Review’’ IEEE Trans. on Systems, Man, and Cybernetics, vol. 39, no. 3, pp. 253–269. [3] Nøttrup T.J., Korreman S. S., Pedersen A. N., Aarup L. R., Nystrom H., Olsen M., and Specht L., ‘‘Intra- and interfraction breathing variations during curative radiotherapy for lung cancer,’’ Radiotherapy and Oncology, vol. 84, no. 1, pp. 40–48, July2007. [4] Takagi T. and Sugeno M., ‘‘Fuzzy identification of systems and its application to modeling and control,’’ IEEE Trans. on Systems, Man, and Cybernetics, no. 116, p. 132, 1985. A framework for real-time target tracking in IGRT using threedimensional ultrasound R. Bruder1, F. Ernst1, A. Schlaefer1, A. Schweikard1 1 University of Lübeck, Institute for Robotics and Cognitive Systems, Lübeck, Germany Keywords 3D ultrasound IGRT Radio surgery Tracking Template matching Fig. 1 Desired (dashed line) and EFuNN predicted (continuous line) for 1,558 breathing samples from a Lung patient 123 Purpose Motion compensation is a well-known practice for radiation therapy [1, 2]. As the target is usually not directly measurable or the sampling rate is limited, surrogate signals are sampled with higher rates and correlated to the internal target movement [3]. This method works well for regular, periodic target motion and surrogate signals, which reflect a high amount of this internal motion. For irregular or changing motion patterns the results of this method are limited. Especially in areas, where multiple motion sources overlap into one target movement, e.g. in proximity of the heart or blood vessels, correlation is nearly impossible or requires a high sampling rate of the target region. We concentrate on using three-dimensional ultrasound as tracking modality for target localization. This method offers the possibility to