A study of the humidification performance of Heat and Moisture
advertisement

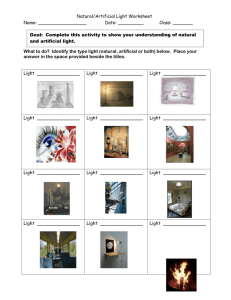
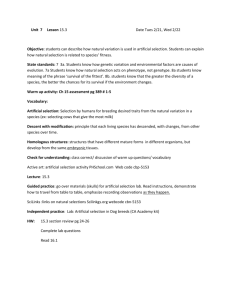
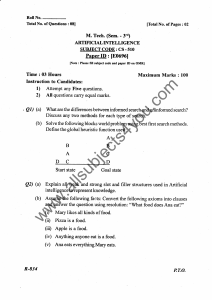
A study of the humidification performance of Heat and Moisture Exchanging Filters in Semi-Closed Circle Anaesthesia Karen Kendall Karen Wilkins Scientific & Laboratory Services Pall Europe ______________________________________________________________________________ Introduction Humidification of dry medical gases has long been recognized as important for preventing damage to the respiratory tract and for decreasing the extent of post operative hypothermia [1], Humidification of inspiratory gases has also been shown to be necessary in semi-closed anaesthesia, despite the humidity levels otherwise generated in such circuits [2]. Heat and moisture exchangers (HME’s) have been used to provide this humidification because they are more economical and convenient to use than hot water bath humidifiers. Heat and moisture exchanging filters (HMEF’s) have the added advantage of reducing circuit and ventilator contamination [3]. Several studies have been performed to evaluate the heat and moisture exchanging properties of HMEF’s [3 - 8]. They have mostly involved the use of laboratory models (artificial patients) designed to simulate lung function by producing saturated water at or near body temperature. Several methods have been used to monitor humidity levels including use of hygrometer probes, collection of expired water vapour and gravimetric techniques which determine water loss from the articial patient [9]. The current ISO Standard for heat and moisture evaluation, ISO 9360 [10], is a gravimetric method. It also recognizes that the articial patient water vapour output is of critical importance and thus specifies that the test apparatus must produce fully saturated water vapour at 34°C. Whilst welcoming the aims and principles of ISO 9360, at least two eminent working groups in this area have listed various practical problems encountered when trying to run the test apparatus [9, 11]. Such problems have mainly focused on the design of the artificial patient, points which have been addressed in the test apparatus used in this study. The test methodology given in ISO 9360 evaluates HME performance in an open circuit, dry gas situation typical of intensive care environments. It does not address the issue of HME performance in other circuit configurations. In this study, HME performance was assessed using a test apparatus designed to simulate semi-closed circle anaesthesia systems whilst maintaining the essential principles of ISO 9360. Materials Ventilators Two ventilators were utilized; a Blease 8100S anaesthesia ventilator obtained from Blease Medical Equipment Limited, Chesham and a Servo 900C obtained from Siemens plc, Sunbury on Thames. Artificial Patient The artificial patient was constructed using a Bennett Cascade Mk II water bath humidifier obtained from Puritan Bennett UK Limited, Hounslow; standard breathing system flutter valves, connectors and tubing; and a one way valve obtained from Abacus Valve Manufacturers Limited, Alton. These were assembled as Figure 1. Apparatus The following pieces of equipment were obtained from the manufacturers listed. Circle absorber and Durasorb (self indicating soda lime) – M & IE, Dentsply, Exeter; Relative humidity / temperature probe – Solomat, Devon; Total airflow meter – British Gas Sothern, Portsmouth; Datex CO2 monitor – Datex Instrumentation Corp., Helsinki, Finland. Test Devices The following devices were tested. Device 1 – Pall BB25 pleated hydrophobic membrane filter (lot 101210) Device 2 – composite device consisting of electret filter media with hygroscopic element Device 3 – composite device consisting of electret filter media with hygroscopic element Methods Evaluation of Artificial Patient Performance The performance of the artificial patient was evaluated at the start of each experimental run to confirm that it produced exhaled air fully saturated with water vapour at 34 °C ie, 100 % relative humidity (RH). The artificial patient was assembled as in Figure 1. New flutter valves were used for each experimental run due to their short life at elevated temperatures. The artificial patient was filled to the ‘maximum’ mark with deionised water. It was connected to a standard non-recirculating circuit as Figure 2 using a Siemens Servo 900C ventilator set at 6 l/min and 12 breaths/min. The ventilator dry gas supply had a humidity not exceeding 0.88 mg/l and a temperature of 23 ± 2 °C. The room ambient temperature was 23 ± 2 °C. The airflow patient exhaled temperature was set at 34 ± 1 °C as measured at the T piece. During a 30 minute stabilisation period (necessary to allow the artificial patient exhaled temperature to reach 34 °C) the circuit was leak tested using the inspiration pause hold function on the ventilator. Testing was only continued if no leaks were apparent. At the end of the stabilization period, the ventilator was switched off and the weight of the artificial patient and the total air flow meter reading recorded. The circuit was reconnected and run for one hour before the artificial patient weight and total airflow meter reading were recorded again. The water loss (mg/l) from the artificial patient was calculated by dividing the difference in weight of the artificial patient (mg) by the total airflow (l). Testing was only continued if the water loss from the artificial patient was 37.6 ± 3.0 mg/l. Evaluation of HME Performance in Semi-Closed Circle Anaesthesia The pre-warmed, pre-weighed artificial patient was connected to an anaesthesia circuit as Figure 3. The ventilator tubing, water traps, airflow meter and absorber canister had been dried in a laminar flow cabinet for at least 12 hours prior to use to eliminate any moisture residues. Fresh Durasorb was added to the dry absorber as per the manufacturer’s instructions (The Durasorb was discarded at the end of each experimental run regardless of whether it was totally or partially exhausted). The humidity and temperature of the room air was measured and recorded. This was compared to the initial humidity reading from the circuit to confirm the lack of moisture residues. If moisture residues were indicated, the equipment was re-dried in the laminar flow cabinet for a further 12 hours. The Blease 8100S ventilator was set at 6 l/min and 12 breaths/min. The total airflow meter reading was recorded. Fresh gas was introduced at the absorber at either 1 or 3 l/min. Carbon dioxide was introduced into the expiratory limb of the artificial patient at a level sufficient to produce a peak exhaled breath reading of 5 % as measured via the monitoring port of the HMEF or via a T piece positioned in place of the HMEF (control). At 1, 2, 3 and 4 hours the ventilator was switched off and the artificial patient disconnected from the circuit at the Y piece. To prevent leakage from the circuit the Y piece was capped. The artificial patient weight, HMEF and catheter mount weight, total airflow meter reading and circuit humidity and temperature were recorded. The water loss (mg/l) from the artificial patient was calculated by dividing the difference in weight of the artificial patient (mg) by the total air flow (l). This was repeated for each of the devices and also without any device in place at both 1 and 3 l/min fresh gas flow. Results The data for water loss from the artificial patient when evaluating the three devices are shown in Tables 1 - 2. At 1 l/min fresh gas flow, the mean water loss for hour 1 was 8.38, 8.00 and 8.12 mg/l for device 1, device 2 and device 3 respectively. This value fell steadily over the four hour test period until during hour 4, the mean water loss was measured as 6.64, 8.79 and 5.26 mg/l for device 1, device 2 and device 3 respectively. No significant difference was observed between the three test devices during each hour period (p < 0.05) using conventional analysis of variance [12]. With no HMEF in the circuit, the mean water loss was 15.44 and 16.08 mg/l for hour 1 and hour 4 respectively. At 3 l/min fresh gas flow, the mean water loss for hour 1 was 9.26, 8.47 and 8.56 mg/l for device 1, device 2 and device 3 respectively. This again fell steadily until at hour 4, the mean water loss was measured as 7.34, 7.90 and 6.87 mg/l for the device 1, device 2 and device 3 respectively. No significant difference was observed between the three test devices during each hour period (p < 0.05). With no HMEF in the circuit, the mean water loss was measured as 17.06 and 15.53 mg/l for hour 1 and hour 4 respectively. The data obtained for circuit humidity measurements are shown in Tables 3 - 4. At both 1 and 3 l/min, the circuit humidity was shown to increase over time and reached 100 % RH (at 23 ± 2 °C) by hour 2. This supports the findings from the water loss experiments which demonstrate that all three HMEF’s performed similarly. Discussion The current ISO Standard for heat and moisture evaluation, ISO 9360, specifies that the test apparatus (artificial patient) must produce fully saturated water vapour at 34 °C. This was confirmed in this study at the beginning of each experimental run. The water loss from the artificial patient was demonstrated to be 37.6 ± 3.0 mg/l (The predicted water loss is 37.6 mg/l for air fully saturated with water vapour at 34 °C but it must be recognized that the unavoidable dead space within the patient model will have some influence on water loss results obtained). Confirmation of the consistency of artificial patient performance also ensured that any differences in subsequent test results obtained were due to changes in test parameters and not due to artificial patient variability. The semi-closed circle anaesthesia test circuit incorporated a canister containing soda lime. The mechanism of action of soda lime is to produce water as a product of carbon dioxide absorption. This results in an increasing circuit humidity level with time. Water loss from the artificial patient will vary depending on the humidity of the inspired air. Thus, if the inspired air is dry, a large amount of moisture is required from the artificial patient to humidify the air and produce exhaled gas at 100 % RH. Conversely, if the inspiratory air is already partially humidified, less moisture is required from the patient and the measured water loss will be less. It was therefore essential in the experimental protocol followed to standardize the humidity level in the semi-closed anaesthesia circuit at the beginning of each test run. This was achieved by the use of fresh soda lime for each run and ensuring that there were no moisture residues in the circuit prior the start of each test. Results from this study demonstrate that in a semi-closed circle anaesthesia system, there is no significant difference in the water loss from an artificial patient when using device 1, device 2 or device 3, ie, there is no difference in measured HME performance. Although HMEF’s have been shown to perform to varying degrees of efficiency in a nonrecirculating circuit [3], this was not found to be the case in this study. Therefore, with individual manufacturers’ products providing equivalent heat and moisture exchanging ability, it is important to consider the other characteristics when choosing a HMEF. The danger of cross contamination through anaesthesia and ventilator circuits is well known (due to a number of case reports) and the importance of taking measures to avoid such cross-contamination is generally accepted [13]. Recently the Australian New South Wales Health Department issued a Public Health bulletin [14] detailing the likely patient-to-patient transmission of hepatitis C in a private hospital. It was proposed that patient A had coughed at some stage of an anaesthetic procedure and that respiratory secretions were consequently introduced into the reusable part of the anaesthetic circuitry. This acted as a reservoir for the virus, which was able to be transmitted to four subsequent patients (patients B, C, D and E). HMEF’s do not perform equally with regard to filtration capabilities. In various studies only Pall pleated hydrophobic membrane HMEF’s have consistently been shown to prevent the passage of both aqueous and airborne suspensions of bacteria and viruses [15 - 17] . In conclusion, the HME performance of three HMEF devices was found to be similar in a semi-closed anaesthesia circuit. Other characteristics, such as filtration capability, have been shown to vary considerably between devices and should be carefully considered when choosing a HMEF for use in anaesthesia. TABLE 1: EVALUATION OF HME PERFORMANCE IN SEMI-CLOSED CIRCLE ANAESTHESIA SYSTEM AT 1 l/min FRESH GAS FLOW Device Device 1 Device 2 Device 3 No Device ARTIFICIAL PATIENT WATER LOSS (mg/l) HOUR 1 Hour 2 Hour 3 Hour 4 6.29 6.38 6.31 8.89 8.29 6.82 8.14 9.09 6.24 6.23 7.83 7.78 5.73 5.75 7.39 7.75 χ = 6.64 χ = 6.29 χ = 7.42 χ = 8.38 8.04 10.21 6.45 8.36 7.76 6.46 8.77 7.71 14.66 5.69 9.94 7.15 7.17 6.99 7.44 7.96 6.32 6.90 5.51 8.84 χ = 8.79 χ = 7.25 χ = 7.62 χ = 8.00 4.16 7.06 7.32 8.73 5.85 6.28 7.77 7.78 6.07 4.22 6.17 9.66 4.95 5.08 5.59 6.32 χ = 5.26 χ = 5.66 χ = 6.71 χ = 8.12 16.65 16.32 15.34 16.08 14.23 17.02 16.44 16.08 χ = 15.44 χ = 16.67 χ = 15.89 χ = 16.08 TABLE 2: EVALUATION OF HME PERFORMANCE IN SEMI-CLOSED CIRCLE ANAESTHESIA SYSTEM AT 3 l/min FRESH GAS FLOW Device Device 1 Device 2 Device 3 No Device ARTIFICIAL PATIENT WATER LOSS (mg/l) HOUR 1 Hour 2 Hour 3 Hour 4 5.44 7.24 7.89 9.34 11.10 7.72 9.50 9.29 5.31 4.85 8.64 9.53 7.52 7.37 8.21 8.89 χ = 7.34 χ = 6.79 χ = 8.56 χ = 9.26 5.72 5.61 7.78 8.53 5.96 6.79 6.05 9.95 9.07 7.91 8.43 10.87 4.50 5.79 6.99 χ = 7.90 χ = 6.20 χ = 6.54 χ = 8.47 8.52 8.49 7.60 8,78 6.35 5.69 7.80 5.86 5.54 6.94 9.63 6.76 6.44 9.58 8.04 χ = 6.87 χ = 6.54 χ = 8.04 χ = 8.56 15.10 15.12 17.36 18.23 15.96 15.70 15.00 16.09 χ = 15.53 χ = 15.41 χ = 16.18 χ = 17.06 TABLE 3: RELATIVE HUMIDITY (%) MEASURED IN SEMI-CLOSED CIRCLE ANAESTHESIA CIRCUIT – 1 l/min FRESH GAS FLOW* RELATIVE HUMIDITY (%) MEASURED IN CIRCUIT AT TIME 0 HOUR 1 Hour 2 Hour 3 Hour 4 HOUR Device 1 25 86 100 100 100 33 100 100 100 100 39 95 100 100 100 45 99 100 100 100 Device 2 43 100 100 100 100 49 100 100 100 100 20 87 100 100 100 36 77 100 100 100 Device 3 27 73 100 100 100 36 68 100 100 100 46 100 100 100 100 40 100 100 100 100 *Note: Circuit temperature = 23 ± 2 °C Device TABLE 4: RELATIVE HUMIDITY (%) MEASURED IN SEMI-CLOSED CIRCLE ANAESTHESIA CIRCUIT – 3 l/min FRESH GAS FLOW* RELATIVE HUMIDITY (%) MEASURED IN CIRCUIT AT TIME 0 HOUR 1 Hour 2 Hour 3 Hour 4 HOUR Device 1 42 100 100 100 100 47 100 100 100 100 34 100 100 100 100 24 100 100 100 100 Device 2 37 100 100 100 100 39 73 100 100 100 42 74 100 100 100 29 51 100 100 100 Device 3 43 84 100 100 100 43 73 100 100 100 40 62 100 100 100 33 69 96 100 100 *Note: Circuit temperature = 23 ± 2 °C Device References 1. Bengtson, J.P., Bengtson, A., Svengvist, O. (1989). The circle system as a humidifier. British Journal of Anaesthesia 63, 453 – 457. 2. Tontschev, G., Luder, M., Benson, Ch. (1979). Humidity and temperature of breathing gas in semi-closed and closed anaesthesia circle systems. Anaesthesia U Reanniat H2, 78 – 86. 3. Shelly, M., Bethune, D. W., Latimer, R. D. (1986). A comparison of five heat and moisture exchangers. Anaesthesia 41, 527 – 532. 4. Walker, A. K. Y. and Bethune, D. W. (1976). A comparative study of condenser humidifiers. Anaesthesia 31, 1086 – 1093. 5. Mebius, C. (1983). A comparative evaluation of disposable humidifiers. Acta Anaesthesiology Scandinavia 27, 403 – 409. 6. Weeks, D. B. (1986). A laboratory evaluation of recently available heat-andmoisture exchangers. Anaesthesiology Review 13, 33 – 36. 7. Kugimiya, T., Phuc, T. G. Numata, K. (1989). Laboratory evaluation of heat and moisture exchangers. Journal of Anaesthesia 3, 80 – 85. 8. Eckerbom, B. and Lindholm, C. E. (1990). Laboratory evaluation of heat and moisture exchangers. Assessment of the draft international standard (ISO/DIS 9360) in practice. Acta Anaesthesiology Scandinavia 34, 291 – 295. 9. Bethune, D. W. (1991). Evaluation of test methods used to determine moisture conservation. Italian Hospitals Anaesthesia / Intensive Care Association Update Meeting on Mechanical Ventilation: Aspects of Thermoregulation, Humidification and Bacterial / Viral Protection. Are 330 15 June 1991 10. ISO 9360 1992(E) 1st edition. Anaesthetic and respiratory equipment – heat and moisture exchangers for use in humidifying respired gases in humans. 11. Heat and moisture exchanger (HME). Pall BB22-15F (1991). Medical Devices Directorate Evaluation 93. 12. Altman. D. G. (1991). Practical statistics for medical research. Chapman and Hall. 13. Wille, B. (1989). Hygiene measures for anaesthesia and ventilator equipment. Krankenhaus-Hygiene und Infektionsverhütung 11, 17 – 21. 14. Chant, K., Kociuba, K., Munro, R., Crone, S., Kerridge, R., Quinn, J., Wyland, M., Miller, G., Turner, I., Brown, J., Baird, L., Locarni, S., Bowden, S., Kenrick, K. G., Maidment, C. (1994). Investigation of possible patient-to-patient transmission of hepatitis C in a hospital. New South Wales Public Health Bulletin 5, 47 – 51. 15. Hedley, R. M. and Allt-Graham, J. (1992). A comparison of the filtration properties of heat and moisture exchangers. Anaesthesia 47, 414 – 420. 16. Lee, M. G., Ford, J. L., Hunt, P. B., Ireland, D. S., Swanson, P. W. (1992). Bacterial retention properties of heat and moisture exchanging filters. British Journal of Anaesthesia 69, 522 – 525. 17. Lloyd, G., Howells, J., Benbough, J. (1995). Efficacy of a pleated hydrophobic filter as a barrier to hepatitis C transmission within breathing systems. Centre for Applied Microbiology and Research. Ventilator tubing Low resistance check valve Flutter valve Independent temperature probe 2 litre rubber lung Bennett Cascade humidifier Water level kept to maximum mark Tubing between dotted lines insulated to prevent rain out FIGURE 1: ARTIFICIAL PATIENT Temperature control box Total flow meter Ventilator Artificial patient FIGURE 2: STANDARD NON-RECIRCULATING CIRCUIT Humidity and Temperature Probe CO2 Analyser Water Trap Ventilator Total flow meter Soda Lime Canister Test device Water Trap Artificial patient CO2 Temperature Probe FIGURE 3: CIRCLE ANAESTHESIA TEST RIG Gas to Drive Ventilator Fresh Gas Flow