CHALLENGES_FACED_BY
advertisement

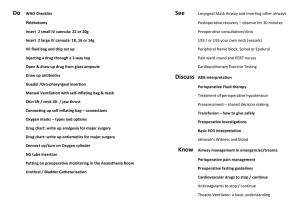
CHALLENGES FACED BY PRACTISING ANAESTHESIOLOGISTS DR.C.RATHNA KUMAR CONSULTANT ANAESTHESIOLOGIST NOTHING IN THE WORLD IS WITHOUT A CHALLENGE TO BE A SUCCESSFUL ANAESTHESIOLOGIST ONE SHOULD HAVE A HIGH DEGREE OF KNOWLEDGE , SKILL AND MENTAL AND PHYSICAL STAMINA TO FACE THE CHALLENGES OUR PROFESSION IS MANY A TIMES EQUATED TO THAT OF THE PILOTS. CLASSIFICATION OF CHALLENGES PROFESSIONAL HEALTH FAMILY LIFE & OTHER SOCIAL ACTIVITIES PROFESSIONAL WORKING SET UP PRIMITIVE SET UP - ATTRACTING MIDDLE CLASS POORLY EQUIPPED THEATRES LITTLE IMPORTANCE TO ANAESTHESIA & I C U FORCED TO WORK TAKING ALL RISKS & COMPROMISES ANYTHING GOES WRONG WE ARE BLAMED SET UP CONTINUES TO WORK WITHOUT ANY CHANGE BUT FOR THE ANAESTHESIOLOGIST THANKS TO THE C P A AND M C I MINIMUM MANDATORY REQUIREMENTS IN THE OPERATION THEATRE A WELL MAINTAINED ANAESTHESIA MACHINE MINIMUM 2 O2 AND N2O CYLINDERS ATTACHED TO THE MACHINE AND 1 EACH KEPT STANDBY TWO WORKING LARYNGOSCOPES WITH BLADES OF ALL SIZES AIRWAYS OF ALL SIZES ENDOTRACHEAL TUBES OF ALL SIZES SUCTION APPARATUS TILTABLE OPERATING TABLE DIFFICULT INTUBATION AIDS LIKE STYLET , MAGILL’S FORCEPS AN ANAESTHETIST’S ASSISTANT UNINTERRUPTED POWER SUPPLY FOR ESSENTIAL EQUIPMENTS ALL EMERGENCY DRUGS & AMBU BAG WITH O2 TUBINGS A STETHOSCOPE , SPHYGMOMANOMETER , PULSE OXIMETER , ECG MONITOR A DEFIBRILLATOR ESSENTIAL NARCOTICS & VAPOURIZERS N P O FOR ATLEAST 6 HOURS MAINTAINENCE OF ANAESTHESIA RECORD INFORMED & WRITTEN CONSENT A MECHANICAL VENTILATOR TIMING OF SURGERY UNLESS AN EMERGENCY,DISCUSS AND FIX DAY TIME IS BETTER VIGILANCE IS ESSENTIAL PREOPERATIVE EVALUATION OFTEN NEGLECTED EVALUATE AS EARLY AS POSSIBLE GOOD HISTORY RELEVANT INVESTIGATIONS SPECIALISTS OPINION AS REQUIRED IMPORTANT IN MEDICOLEGAL CASES FITNESS IS OUR DECISION OPTIMIZATION BEFORE SURGERY GOOD RAPPORT WITH THE PATIENTS AND FAMILIES IS THE CENTRE APPROPRIATE FOR A CASE? NO PROTOCOL ISA SHALL FORMULATE ONE CAREFUL PREOPERATIVE INSTRUCTIONS NO ANTIBIOTICS JUST BEFORE ANAESTHESIA NO DRUG WITHOUT OUR KNOWLEDGE TO BE GIVEN IN THE PERIOPERATIVE PERIOD ANAESTHETIC MANAGEMENT CHOICE OF ANAESTHESIA SHOULD BE OURS PERFECT COCKPIT DRILL ENSURE GOOD I/V LINES ASSURE THE SAFETY OF PTS POSTOP AND LEAVE MOST RISKY PERIOD-WHILE SHIFTING TO POSTOP WARD FOR ICU CARE GOOD NETWORK IS REQUIRED INSTITUTE AND FREELANZING PRACTICE SCHEDULE CONTOL OF OT CONTROL OF STAFFS OPTIMIZATION REPLACEMENT RISK OFFS FROM DUTY INCOME HEALTH PROBLEMS STRESS HYPERTENSION-HR>100/MT, DBP>1OOMM HG INSOMNIA AND OTHER SLEEP DISTURBANCES IRRITABLITY ANXIETY HEADACHE ASTHMA LACK OF CONCENTRATION ACIDITY BODYACHE DEPRESSION AND OTHER CHANGES IN BEHAVIOUR SUICIDAL TENDENCY SUBSTANCE ABUSE CAUSES OF STRESS SENSE OF INSECURITY CHANGING WORKING ENVIRONMENT LACK OF CONTROL OVER WORKING TIME LACK OF CONTROL OVER OT MANAGEMENT UNSATISFIED EGO MANAGEMENT OF STRESS A BREAK FROM ROUTINE MENTAL RELAXATION TECHNIQUES LIKE YOGA MAINTAIN PHYSICAL FITNESS SOME LEISURE ACTIVITY DISCIPLINED ANAESTHETIC PRACTICE FAMILY AND OTHER SOCIAL ACTIVITIES PLANNING OF HOLIDAYS RISE IN PRACTICE COMPETITION CATASTROPHES ILLNESS AND DISABILITY INVESTING IN EQUIPMENTS ALLOTING TIME FOR SELF & FAMILY ATTENDING CME AND CONFERENCES PRACTICE PRESSURES-UNETHICAL METHODS INCREASED RISKS OF ACCIDENTS TAKE HOME MESSAGE DO A DIGNIFIED & SAFE PRACTICE OF ANAESTHESIA FACE CHALLENGES WITH A BRAVE HEART BE CONTENDED OUR SPECIALITY HAS THE POTENTIAL TO DO GREAT BENEFIT & HARM TO THE PATIENT