How does the management differ?
advertisement

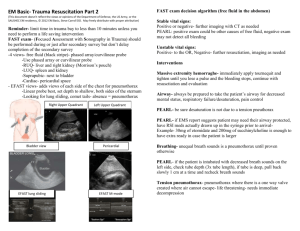
Lesson 5 Breathing, Ventilation, and Oxygenation Anatomy (1 of 3) • Ribs –12 pairs • 10 pairs attach to sternum and spine • 2 pairs (floating ribs) attach only in back –An intercostal nerve, artery, and vein are found along the inferior border of each rib Anatomy (2 of 3) • Lungs • Mediastinum –Trachea –Esophagus –Main bronchi Anatomy (3 of 3) • Mediastinum –Heart –Major arteries • Aorta and branches • Pulmonary arteries –Veins • Superior vena cava • Pulmonary veins Physiology of Life Review • Oxygen is transported across the alveolar–capillary membrane • It then attaches to hemoglobin in red blood cells for transport to the rest of the body • At the same time, CO2 moves from the blood plasma into the alveoli Breathing • The mechanical act of moving air into the lungs and alveoli • Controlled by the respiratory center of the brain • Chemoreceptors located in the aorta and carotid arteries stimulate the respiratory center • Rate and depth of ventilation are continuously adjusted to maintain normal PaCO2 levels Breathing Assessment (1 of 7) • Normal breathing is not a noticeable process • If the patient’s breathing draws your attention, then there is a problem until proven otherwise – Some examples include: • Breathing you can hear from across the room • Inability to speak in complete sentences • Patient positioning to ease breathing (e.g., tripoding) Breathing Assessment (2 of 7) • Look (observe) • Listen (auscultate) • Feel (palpate) © Jones & Bartlett Learning. Courtesy of MIEMSS. Breathing Assessment (3 of 7) • Look (observe) – Increased respiratory effort • Positioning • Use of accessory muscles • Retractions • Nasal flaring in children Courtesy of Health Resources and Services Administration, Maternal and Child Health Bureau, Emergency Medical Service for Children Program Breathing Assessment (4 of 7) • Look (observe) (cont’d) – Visible signs of trauma • • • • • Contusions Hematomas Lacerations Sucking chest wound Paradoxical movement of the chest wall Breathing Assessment (5 of 7) • Listen (auscultate) for breath sounds – Presence • Equality (right and left) • Asymmetric – Decreased on one side – Absent © Jones & Bartlett Learning. Courtesy of MIEMSS. Breathing Assessment (6 of 7) • Listen (auscultate) for breath sounds (cont’d) – Abnormal sounds • • • • Wheezing Rales Rhonchi Crepitus (bony or subcutaneous emphysema) Breathing Assessment (7 of 7) • Feel (palpate) the chest for: – Bony crepitus – Subcutaneous emphysema – Abnormal movement of the chest wall – Bony tenderness Common Injuries That Affect Breathing • Pneumothorax – Simple – Tension – Open • Hemothorax • Rib fractures – Simple – Flail chest Pneumothorax • Present in up to 20% of severe chest injuries • Classified as either: – Simple – Tension – Open • A simple pneumothorax may progress to a tension pneumothorax as air continues to accumulate within the affected hemithorax – Tension pneumothorax is life-threatening – Needle decompression may be required • May be associated with a hemothorax Simple Versus Tension Pneumothorax • Simple – Blunt or penetrating injury – Breath sounds decreased or absent – Mild to moderate ventilatory distress – May progress to tension • Tension – Blunt or penetrating injury – Breath sounds decreased or absent – Marked ventilatory distress – Hemodynamic compromise How does the management differ? Open Pneumothorax • Penetrating mechanism – May be “sucking” or “bubbling” chest wound • Respiratory distress – Mild to severe • May be associated with a hemothorax • Optimal method of field management has not been demonstrated Hemothorax • • • • Blunt or penetrating mechanism Bleeding into the pleural cavity May be associated with a pneumothorax Air or blood in the pleural space compromises lung capacity Simple Rib Fractures • • • • Most common thoracic injury Usually involves ribs 4 through 8, laterally Most common cause of hemothorax Common complaints are chest pain and shortness of breath • May be associated with injuries to liver and spleen Flail Chest (1 of 2) • Two or more adjacent ribs fractured in more than one place • Compromises the structural integrity of the chest, causing paradoxical movement while breathing Flail Chest (2 of 2) • Associated with underlying injury –Pneumothorax –Hemothorax –Pulmonary contusion Treatment of Chest Injuries • The goal is to maintain or restore adequate oxygenation and ventilation – Administer supplemental oxygen – Assist ventilations as necessary – Seal open chest wounds – Recognize and decompress tension pneumothorax • Continuous assessment of breathing is essential Supplemental Oxygen • Can be administered by nonrebreathing mask, a bag-mask device, or an oxygen-powered ventilator • Never withhold oxygen from a patient in respiratory distress • Monitor oxygen saturation – Target SpO2 greater than 95% • Increasing the levels of inspired oxygen assists in maintaining aerobic metabolism When to Assist Ventilations • Ventilatory rate – Greater than 30 – Less than 10 • Insufficient spontaneous tidal volume: – Poor chest rise – Use of accessory muscles • Decreased SpO2 • Increased ETCO2 • Consider the need for airway management Assisting Ventilations Bag-Mask Devices Manually-Triggered Devices Automatic Devices Courtesy of Impact Instrumentation, Inc. Courtesy of AAOS Ventilatory Rates and Tidal Volumes • Adult – 10 to 12 breaths per minute (bpm) – 500 to 800 ml • Child – 16 to 20 bpm – 100 to 500 ml or until good chest rise • Infant – 25 bpm – 6 to 8 ml/kg tidal volume • Inadvertent hyperventilation may lead to poor outcomes in patients with traumatic brain injury Monitoring Ventilations • Capnometry and capnography – Can monitor: • • • • Spontaneously breathing patient Bag-mask device Endotracheal tube Supraglottic airways – Maintain between 35 to 45 mm Hg – May give false reading in hypotension but can be used to monitor trends Needle Decompression • Used to relieve tension pneumothorax • Appropriate placement is essential: – Second intercostal space, midclavicular line, over the rib (preferred site) – Fifth intercostal space, midaxillary line, over the rib (alternate site) Summary • Caring for a trauma patient experiencing respiratory difficulty includes: – Maintaining a patent airway – Administering supplemental oxygen – Supporting and monitoring ventilations – Recognizing and decompressing tension pneumothorax Questions?