Abnormal EKG study guide comp
advertisement

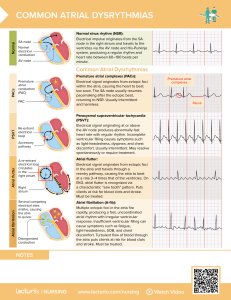
Normal Sinus Rhythm Sinus Arrhythmia Variable rates. Usually asymptomatic Sinus Bradycardia Normal in athletes Beta blockers, Decreased function of SA Node Generally asymptomatic unless pathologic condition exists (may be in the presence of 2nd or 3rd degree block May c/o dizziness, syncope, angina Sinus Tachycardia Generally benign (SA node automaticity increased and pts asymptomatic Fear, anxiety, caffeine, nicotine, amphetamines, or demands of O2 are higher (exercise, infection, MI, hemorrhage T-wave might blend into P wave in tachycardia Sinus exit block block in conduction of impulse from SA node to atria Sinus Exit Block: pause equal to two complete cardiac cycles; overall heart rate, 70. Premature Atrial Contraction Ectopic focus in either atria initiates an impulse before the next impulse initiated by the SA node Causes: emotional stress, nicotine, caffeine, alcohol, infection, hypoxemia, MI, atrial damage Asymptomatic and if frequency is low, no treatment required, and pt should be able to participate in activity When frequency increased, atrial tachy or a-fib may result P wave comes earlier than usual. P wave is usually a little bit larger. Atrial Tachycardia HR may be 100-200bpm Same causes as PAC but also includes pulmonary HTN, altered pH, and COPD Q (cardiac output) compromised if prolonged Dizziness, fatigue and SOB Atrial Flutter Caused by pathologic conditions: mitral valve disease, CAD, infarction, stress, renal failure, pericarditis, rheumatic heart disease, MI Rapid rate d/t the firing of an ectopic source in the atria AV-node is crucial- blocks the signal from getting to ventricles Unless ventricular rate becomes too high, Q is not compromised Asymptomatic Atrial flutter-1-2 areas causing atria to contract but signal is not getting thru to QRS. QRS is on normal rhythm Atrial Fibrillation Erratic quivering of atria Multiple ectopic foci emit electrical impulses No true depolarization of the atria AV Node acts to control ventricles Causes: Advanced age, CHF, ischemia or infarction, cardiomyopathy, digoxin toxicity, drug use, stress/pain, renal failure QRS are not regular rhythm either; AV node tries to pace ventricles. Compromised response to exercise Problems associated with a-fib No atrial “kick” Responsible for forcing out the last amount of volume from atria to ventricles Accounts for 30% of Q If ventricular rate is less than 100bpm at rest, should monitor with exercise for Q compensation If ventricular rate is greater than 100bpm at rest, monitoring should be assessed during all activities and engaged in with caution (a-fib with RVR) Likely to have Q compensation Missing p-wave then SA node in not pacing the heart; av node initiated rhythm but not p-wave . Look at 5th QRS complex. Asymptomatic if infrequent Faster; inverted p wave or retrograde p wave depolarization. SOB and not feeling well, possible fluttering in chest, losing atrial kick; wide qrs comple They look the same and coming from same place. They look different. Diminished cardiac output due to decreased systolic filling time. AV node is like a police officer sometimes not letting signal conduct through resulting in block. V-tach is likely from this point. Stop all activity. Decreased stroke volume, and cardiac output. PVC bigemony is every other beat a PVC. Flat line or agonal rhythm is next step Looks similar to v tach. Unclear if it is from a single site or multiple sites. Unlike v tachy the wave amplitude of torsaes begins close to the baseline, gradually increasing and decreasing in a repeating pattern. Resembles a twisting and turning mpotion along the baseline . Need to differentiate because treated differently. Starts suddenly, frequently preceded by a prolonged QT interval. Might be caused by low Potassium. Translated as “Twisting of Points” Coming from ventricle, 20-40 bpm, wide qrs, ventricle is pacing. Very slow rhythm. Cardiac output is severely compromised Beginning p-wave to beginning of r wave or longer pr interval longer than 0.2 seconds Has p wave and normal qrs, rate will be a little slower 2nd degree block, 1st type is Wenckebach and 2nd type. Wenckebach PR interval is getting longer each beat then drops QRS. Pr interval but missing qrs LAE can be caused by mitral valve stenosis Right bundle block the right side is conducting slower typically seen in V1 Left bundle block more prominent in R-wave in V5-6