36x72 poster template
advertisement

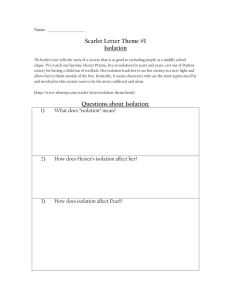
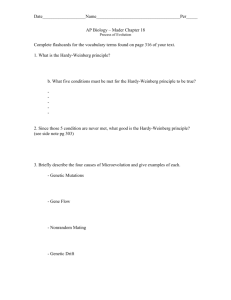
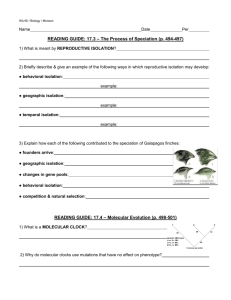
STANDARDIZATION OF ISOLATION PRACTICES IN THE PERIOPERATIVE CARE SETTING Lorrie Ingram, BSN, RN, Infection Control Practitioner; Susie (Treasa) Leming-Lee, MSN, RN, CPHQ, Director of Perioperative Quality Management; Vicki Brinsko, BSN, RN, CIC, Infection Control Practitioner, Dept. Coordinator; Jena Skinner, BSN, RN, CIC, Infection Control Practitioner; Ann H. Benco, MSTD, BSN, RN, CNOR, Perioperative Nurse Educator; Erin Kuhn, RN, MSN, CNOR, Perioperative Nurse Educator; Audrey H. Kuntz, EdD, RN, Director of Perioperative Education/Operative Services; Stephanie Randa, MHA, RN, Director of Operative Services; Thomas R. Talbot, III, MD, MPH, Hospital Epidemiologist, Infectious Disease, Titus L. Daniels, MD, MPH, Assistant Professor of Medicine-Infectious Disease, Associate Hospital Epidemiologist; Addison K. May, MD, FACS, FCCM, Associate Professor of Surgery and Anesthesiology ABSTRACT 2008 APIC Abstract Isolation Precautions Process Subject Category - Quality Management Systems/Process Improvement/Adverse Outcomes Standardization of Isolation Practices in the Perioperative Service Line Lorrie Ingram, BSN, RN, Infection Control Practitioner; Vicki Brinsko, BSN, RN, CIC, Infection Control Practitioner, Dept. Coordinator; Jena Skinner, BSN, RN, CIC, Infection Control Practitioner; Ann Benco, RN, Nurse Educator, Operative Services; Erin Kuhn, RN, MSN, CNOR, Perioperative Nurse Educator; Audrey H. Kuntz, EdD, RN, Director of Perioperative Quality Mgmt/Operative Services; Susie Leming-Lee, MSN, RN, CPHQ, Associate Director of Perioperative Quality Management/Operative Services, Thomas R. Talbot, III, MD, MPH, Hospital Epidemiologist, Infectious Disease, Assistant Professor of Medicine and Preventive Medicine, Titus L. Daniels, MD, MPH, Assistant Professor of Medicine-Infectious Disease, Associate Hospital Epidemiologist ISSUE: A cluster of Highly-resistant Acinetobacter baumannii (HR-ACBA) cases in the surgical critical care unit of a large tertiary care medical center provided the impetus for detailed scrutiny of isolation practices, particularly for patients requiring multiple trips to surgery. Noncompliance with aspects of isolation was observed for patients during transport between surgery and critical care. Further investigation revealed a systems approach to improvement would be needed, not only to prevent transmission during transport, but to enhance compliance for all areas of patient contact throughout the perioperative service line. PROJECT: A multidisciplinary team was formed with representatives from surgical critical care, perioperative education, operating room personnel and infection control, to review the existing practices used for handling patients in isolation and to map out an enhanced process (Figure 1) for improvement. System barriers to compliance were identified in all phases of the perioperative patient care process. System enhancements were identified and implemented to facilitate compliance. These included specific education and training modules developed for all levels of staff, including physicians. Perioperative isolation practice standards were formally incorporated into the departmental policy and procedure manual. RESULTS: A unified set of isolation practice standards throughout the perioperative service line was established, which mirrored the existing isolation guidelines practiced throughout the rest of the medical center. System changes included creating electronic case boarding prompts, (Figure 2) to actively inquire as to isolation status and type required, as well as electronic reminders to book airborne isolation cases at the end of the day. The management of operating room (OR) traffic, environmental cleaning, patient transport, supplies and appropriate signage were other key elements of concentration identified for practice change. Improved compliance with isolation practices was observed soon after implementation. While not directly attributable to the perioperative isolation enhancements (simultaneous interventions were introduced in the critical care areas) no further HRACBA cluster outbreaks were identified (Figure 3). LESSONS LEARNED: Although most staff understood the institution’s isolation mandates for contact, droplet and airborne precautions, problems were identified with communication between departments on patient isolation status and proper practices for transporting patients between perioperative areas and critical care. The concept that the OR environment, with respect to routine practices of sterile and aseptic technique, would inherently prevent cross transmission of organisms from patients in isolation was deficient as it did not include appropriate practice patterns prior to and after surgery. This intervention project served to increase awareness and education of the perioperative staff regarding infection prevention and control practices with their isolated patient population. Behavioral changes reflecting improved compliance were influenced by staff collaboration, use of new electronic case boarding prompts and creative methods of communication and education. In addition, providing a new, concentrated and standardized process algorithm to guide the units/OR staff in preparing for and organizing the isolation patient’s transport, equipment handling and environment, was a vital tool for quality improvement. These concepts are reproducible for other service areas with similar clinical challenges. INTRODUCTION A multidisciplinary team was formed with representatives from surgical critical care, perioperative education, operating room personnel and infection control to review the existing practices used for handling patients in isolation and to map out an enhanced process for improvement. System barriers to compliance were identified in all phases of the perioperative patient care process. System enhancements were identified and implemented to facilitate compliance. These included specific education and training modules developed for all levels of staff, including physicians. Perioperative isolation practice standards were formally incorporated into the departmental policy and procedure manual. RESULTS IMPLEMENTATION: DESIGN: FLOW OF WORK PROCESS SCHEDULING Surgeon or surgical resident boards the surgical case Is the pt. on isolation precautions? Yes Thursday October 18TH 2007 PHASE PRE-SURGERY & Patient Unit PHASE: PREPARATION AND TRANSPORT OF PT. TO OR Does Scheduler know the pt.’s type of isolation precautions? Yes No Scheduler calls Pt. Care Unit to ascertain type of pt. isolation precaution No Is pt. on air borne isolation? Is pt. on isolation precautions? Yes Yes Scheduler schedules surgical case for end of day if possile Charge Nurse reviews E-Board and assigns outside runner to operating room Continue current surgical care process Anesthesia provider assesses pt’s condition and equipment needed for transport No No Scheduler selects from computer program one of the following pt. precaution status: · None · Contact · Droplet · Airborne Anesthesia provider arrives in pt’s room Anesthesia provider performs hand hygiene & dons PPE before entering pt.’s room Anesthesia provider and pt’s bedside nurse conduct a handoff which includes: Verification of isolation precautions status a Does MR Know the type of isolation precautions the pt. is under? PATIENT UNIT PHASE: PREPARATION AND TRANSPORT OF PT. TO OR CTI performs hand hygiene & dons PPE before entering pt’s room a CTI arrives in pt’s room and verifies pt. on isolation precaution status CTI, Anesthesia provider, and or Nurse · place a clean sheet on patient · place all pt. monitoring equipment, O2 tank, chart/s (in clear plastic bag) on pt.’s bed · place isolation signs on pt.’s bed · assigns “Clean Person” to assist in transporting pt. to open doors, push elevator buttons, etc. CTI assist Anesthesia provider and or Nurse with the preparation to transport pt. to OR No No Is pt. on droplet Isolaton? Is pt. on airborne isolation ? Yes Bedside Nurse places surgical mask on pt. Yes Bedside nurse places surgical mask on pt. CTI , Anesthesia provider, and or Nurse transport pt. directly to operating room if coming from ICU or on airborne precautions b Circulator in OR calls receiving unit charge nurse to inform that pt is ready to be transported back and verifies pt.’s isolation precautions status Anesthesia provider calls pt. report to unit bedside nurse or unit charge nurse and verifies pt.’s isolation precautions status # of ACBA Clusters Outbreaks INTRAOPERATIVE PHASE OF CARE CTI and OR staff move pt. from bed/ stretcher to OR table 2 Do not remove pt. chart from plastic bag unless needed CTI moves pt. bed into hallway and follow the requirements for bed cleaning below: Circulator in OR conducts “rolling call” to pt. destination as pt. leaves OR Pt. unit receives rolling call and notifies charge nurse and bedside nurse that pt. is in transit and verifies pt.’s isolation precautions 3 No Is pt. under air borne isolation precautions? Surgery starts Surgery ends Cleaning Process: · Don appropriate PPE · Remove sheets from bed and place in linen bag · Spray germicidal disinfectant agent on bed rails, springs, head board & wipe down bed · Place isolation type sign on bed during drying phase · Wait 10 mins · Dress bed with clean sheets · Drape bed with clear plastic sheet · Place isolation signs on pt’s bed OR PREP AFTER PT LEAVES OPERATING ROOM INTRAOPERATIVE CARE PHASE CONTINUES CTI, Anesthesia provider, & Surgical resident don new PPE for transport of pt. to receiving unit Charge Nurse reviews EBoard and orders Hepafilter OR PREP BEFORE PT. ENTERS OPERATING ROOM MR calls bedside nurse to determine type of isolation precaution The management of operating room (OR) traffic, environmental cleaning, patient transport, supplies and appropriate signage were other key elements of concentration identified for practice change. Improved compliance with isolation practices was observed soon after implementation. While not directly attributable to the perioperative isolation enhancements (simultaneous interventions were introduced in the critical care areas) no further HR-ACBA cluster outbreaks were identified (Fig. 3). 8 Place clean sheet over pt. before leaving OR b Blue = New Step Pt. arrives in receiving unit Imp l e me n t a t i o n o f N e w Is o l a ti o n P r e c a uti o n P r o c e s s e s 4 Anesthesia provider recovers non ICU pt. for 30-50 mins in OR ICU patient may be recovered in negative pressure room on their assigned unit 2 0 July POST-OPERATIVE CARE PHASE OR TO PATIENT UNIT CTI, Anesthesia provider, Surgical Resident and assigned “Clean Person” transport pt. to receiving unit 6 ACB A Outbr e a ks , J ul y 2 0 0 7 6 Yes Anesthesia provider and bedside nurse conduct handoff verifying pt.’s isolation precaution status CTI wipes down all transport monitors and other equipment with a germicidal disinfectant agent before leaving the patient’s room CTI, Anesthesia Provider and Surgical Resident remove PPE and perform hand hygiene before leaving pt.’s room Aug Sept Oct Nov Dec Jan Feb March April May June Months-2007-2008 (8 months with no ACBA out breaks) Fig. 3 Red = Verification of Isolation Precaution status Fig. 1 CONCLUSION & LESSONS LEARNED METHODOLOGY/TRAINING Although most staff understood the institution’s isolation mandates for contact, droplet and airborne precautions, problems were identified with communication between departments on patient isolation status and proper practices for transporting patients between perioperative areas and critical care. The concept that the OR environment, with respect to routine practices of sterile and aseptic technique, would inherently prevent cross transmission of organisms from patients in isolation was deficient as it did not include appropriate practice patterns prior to and after surgery. Isolation Precautions Process-Before Pt. Enters OR Key Fundamental Infection Control Concepts Applied: 1. Strict Hand Hygiene adherence 2. Strict/Consistent use of PPE for specific precautions 3. Appropriate Environmental cleaning/disinfection processes 4. Special indications (i.e. for air handling/exchanges for TB) Airborne, Droplet, & Contact Isolation ProcessEnd of Surgical Case “booking” process, 5. Continuous good communication during surgery between the referral/transferring dept.; the Periop Services regarding patients isolation status 6. Highlights and education pertaining to very specific and highly transmittable organisms in the healthcare environment reviewed 2 Circulating Nurse calls the board who assigns “clean person” to aid in transporting pt. back to ICU Circulating Nurse pulls up Whiteboard and confirms Pt.’s isolation status Yes 3 Is pt. under air borne isolation precautions? No Anesthesia provider recovers non ICU pt. in OR for 30-50 minutes ICU ICU pt. may be recovered in negative pressure room on assigned unit · · Circulating Nurse or designee post: “No Traffic” Sign on OR Door “Isolation type precaution” sign on OR Door Anesthesia Technician cleans Anesthesia machine according to standard cleaning methods OR Staff removes any unnecessary equipment from OR · · · · CTI: Don N95 Respirator Bring Hepafilter into OR Place Hepafilter in center of room away from return air vent Plug Hepafilter into electrical outlet and turns Hepafilter on OR Staff closes all cabinet doors in OR Hepafilter runs for one hour Circulating Nurse ensures all surgical case supplies and equipment are in the OR OR Cleaning Staff cleans OR according standard cleaning procedures *No N95 Respirator needed after hepafilter has run for one hour* All OR Staff dons PPEs prior to pt. entering OR CTI wipes outside of isolation cart with a germicidal disinfectant and sends Isolation Cart to Central Supply for cleaning and restocking Yes Is pt. under droplet or contact isolation precautions? No OR Staff cleans OR according to standard cleaning methods OR Staff don appropriate PPE Cleans OR according to standard cleaning methods CTI wipes outside of isolation cart with a germicidal disinfectant and sends Isolation Cart to Central Supply for cleaning and restocking INTRODUCTION METHODOLOGY/TRAINING A unified set of isolation practice standards throughout the perioperative service line was established, which mirrored the existing isolation guidelines practiced throughout the rest of the medical center. System changes included creating electronic case boarding prompts (Fig. 2) to actively inquire as to isolation status and type required, as well as electronic reminders to book airborne isolation cases at the end of the day. The management of operating room (OR) traffic, environmental cleaning, patient transport, supplies and appropriate signage were other key elements of concentration identified for practice change. Simultaneous interventions were introduced in the critical care areas. Key Fundamental Infection Control Concepts Applied: 1. Strict Hand Hygiene adherence 2. Strict/Consistent use of PPE for specific precautions 3. Appropriate Environmental cleaning/disinfection processes 4. Special indications (i.e. for air handling/exchanges for TB) 5. Continuous good communication during surgery “booking” process, between the referral/transferring dept.; the Periop Services regarding patients isolation status 6. Highlights and education pertaining to very specific and highly transmittable organisms in the healthcare environment reviewed This intervention project served to increase awareness and education of the perioperative staff regarding infection prevention and control practices with their isolated patient population. Behavioral changes reflecting improved compliance were influenced by staff collaboration, use of new electronic case boarding prompts and creative methods of communication and education. with similar clinical challenges. Lessons Learned Include: 1. Ensure need for support of project by visible leadership. 2. Provision of a standardized process algorithm to guide staff adherence and education was a vital component of this quality improvement process. These concepts are reproducible for other service areas. 3. Early Solicitation of staff input in the development of this process, as were the specific tools, was vital to overall success. 4. Education of all perioperative staff and faculty was critical to the ownership of the process, and for its continued success. NEW ISOLATION PRECAUTION PROCESS IN ACTION www.mc.vanderbilt.edu/infectioncontrol Fig. 2 Acknowledgements Daniel Beauchamp, MD, Chair of Surgical Sciences Mike Higgins, MD, MPH, Executive Medical Director of Perioperative Services Nancye Feistritzer, MSN, RN Associate Hospital Administrator, Director of Perioperative Services Surgical Site Infection Prevention Collaborative Committee