Ventilation Modes - Philippe Le Fevre
advertisement

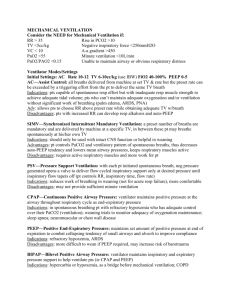
Mechanical Ventilation Overview • • • • • • • Intro NIV Basic Modes Settings Specific Conditions Ventilators Other modes Acute respiratory failure • Hypoxia (PO2 < 60mmHg) – Low inspired O2 – Hypoventilation – CNS, peripheral neuro, muscles, chest wall – V/Q mismatch • Shunt – pneumonia, APO, collapse, contusions – Alveoli perfused but not ventilated – Venous admixture • Anatomical shunt – cardiac anomaly • Increased dead space (hypercapnia) – hypovolaemia, PE, poor cardiac function – Diffusion abnormality – severe destructive disease of the lung – fibrosis, severe APO, ARDS • Hypercapnia (PCO2 >50mmHg) – Hypoventilation – Dead space ventilation – Increased CO2 production Shunt 0 mmHg 450 mmHg 100% 70% 85% Mechanical Ventilation • Pump gas in and letting it flow out • Function – Gas exchange – Manage work of breathing – Avoid lung injury • Physics – – – – – Flow needs a pressure gradient Pressure to overcome airway resistance and inflate lung Pressure (to overcome resistance) = Flow x Resistance Alveolar pressure = (Volume/Compliance) + PEEP Airway pressure = (Flow x Resistance) + (V/C) + PEEP Gas Exchange • Oxygenation – get O2 in – FiO2 – Ventilation (minor effect) – alveolar gas equation, CO2 effect – Mean alveolar pressure • Mean airway pressure – surrogate marker, affected by airway resistance • Pressure over inspiration + expiration • Set Vt or inspiratory pressure • Inspiratory time • PEEP – Reduce shunt • Re-open alveoli – PEEP • Prolonging inspiration – improve ventilation of less compliant alveoli • Ventilation – get CO2 out – Alveolar ventilation = RR x (Tidal volume – Dead space) Adverse Effects • Barotrauma – High alveolar pressure – High tidal volume – Shear injury – • Repetitive collapse + re-expansion of alveoli • Tension at interface between open + collapsed alveoli – Pneumothorax, pneumomediastinum, surgical emphysema, acute lung injury • Gas trapping – Insufficient time for alveoli to empty – Increase risk • Airflow obstruction – asthma, COPD • Long inspiratory time • High respiratory rate – Progressive • Hyperinflation • Rise in end-expiratory pressure – intrinsic-PEEP, auto-PEEP – Result – Barotrauma, Cardiovascular compromise (high intrathoracic pressure) • Oxygen toxicity – Acute lung injury due to high O2 concentrations • Cardiovascular effects – Preload – positive intrathoracic pressure reduces venous return – Afterload - positive intrathoracic pressure reduces afterload – Cardiac Output – depends on LV contractility • Normal – IPPV decreases CO • Reduced – IPPV increases CO – Myocardial O2 consumption - reduced Gas Trapping NIV • CPAP – Similar to PEEP – Splint alveoli open – reduce shunt – Spontaneous breathing at elevated baseline pressure • BiPAP – Ventilatory assistance without invasive artificial airway – Fitted face/nasal mask – Initial settings 10/5 NIV NIV • Indicator of success – – – – – – Known benefits Younger age Lower APACHE score Cooperative Intact dentition Moderate hypercarbia (pH<7.35, >7.10) – Improvement within first 2 hrs • Contraindications – – – – – – Cardiac/Resp arrest Non-respiratory organ failure Encephalopathy GCS <10 GIH Haemodynamically unstable Facial or neurological surgery, trauma or deformity – High aspiration risk – Prolonged ventilation anticipated – Recent oesophageal anastamosis NIV Benefits • • • • • • • • General COPD Cardiogenic pulmonary oedema Hypoxaemic respiratory failure Asthma Post-extubation Immunocompromised Other diseases What is a Mode? • 3 components • Control variable – Pressure or volume • Breath sequence – Continuous mandatory – Intermittent mandatory – Continuous spontaneous • Targeting scheme (settings) – Vt, inspiratory time, frequency, FiO2, PEEP, flow trigger Volume Control Ventilation • Set tidal volume • Minimum respiratory rate • Assist mode – both ventilator and patient can initiate breaths • Advantage – Simple, guaranteed ventilation, rests respiratory muscle • Disadvantages – – – – – Not synchronised – ventilator breath on top of patient breath Inadequate flow – patient sucks gas out of ventilator Inappropriate triggering Decreased compliance – high airway pressure Requires sedation for synchrony VCV Pressure Control Ventilation • • • • • Set inspiratory pressure Constant pressure during inspiration High initial flow Inspiratory pause – built in Advantages – Simple, avoids high inspiratory pressures, improved oxygenation • Disadvantages – Not synchronised – Inappropriate triggers – Decreased compliance – reduced tidal volume PCV Pressure Support • • • • Set inspiratory pressure Patient initiates breath Back-up mode – apnoea Cycle from inspiration to expiration – Inspiratory flow falls below set proportion of peak inspiratory flow • Advantages – Simple, avoids high inspiratory pressure, synchrony, less sedation, better haemodynamics • Disadvantages – Dependent on patient breaths – Affected by changes in lung compliance PS Synchronised Intermittent Mandatory Ventilation • Mandatory breaths – VCV, PCV • Patient breaths – depends on SIMV cycle – Synchronised mandatory breath – Pressure support breath • Advantages – Synchrony, guaranteed minute ventilation • Disadvantages – Sometimes complicated to set SIMV VCV vs PCV VCV vs PCV VCV vs PCV - Advantages • PCV + PS – Variable flow – Reduced WOB – Max Palveolar = Max Pairway (or less) – Palveolar controlled – Variable I-time & pattern (PS) – Better with leaks • VCV – Consistent TV • changing impedance • Auto-PEEP – Minimum min. vent. (f x TV) set – Variety of flow waves VCV vs PCV - Disadvantages • PCV + PS – Variable tidal volume • Too large or too small • No alarm/limit for excessive TV (except some new gen. vents) – Some variablity in max pressures (PC, expir. effort) • VCV – Variable pressures • airway • alveolar – Fixed flow pattern – Variable effort = variable work/breath – Compressible vol. – Leaks = vol. loss Settings • • • • • FiO2 – start at 1.0 RR – average 12, higher for those with sepsis/acidosis Tidal volume – 500ml, 8ml/kg, smaller volumes in ARDS Inspiratory pressure - <30cmH2O, sum of PEEP + Pinsp Inspiratory time – I:E – normally 1:2, simulates normal breathing – synchrony – PCV – easy to set – VCV – complicated, Time = Volume/Flow • PEEP – Start at 5cmH2O – Higher – APO, ARDS – Lower – asthma, COPD • Triggering – Flow triggering – more sensitive, synchrony, -2cmH2O – Pressure triggering – Inappropriate triggering – triggering when no patient effort • Oxygenation • Ventilation – FiO2, PEEP, Insp Time, InspP, Insp pause – Problems – CVS effects, gas trapping, barotrauma – Tidal volume, RR, eliminate dead space – Problems – barotrauma, gas trapping (reduced minute ventilation) Troubleshooting Airway pressure – – – – – Tidal volume – – – – • • • Minute ventilation – determined by RR + Vt Apnoea – important in PS Intrinsic PEEP (gas trapping) – • Expiratory pause hold Hypotension – after initiating IPPV – – – – • Reduced – respiratory acidosis Monitor in PCV/PS Changes in compliance – anywhere in system Expired Vt – more accurate Hypovolaemia/Reduced VR Drugs Gas trapping – disconnect Tension pneumothorax Dysynchrony – – – Patient factors Ventilator – settings, eg I:E PS > SIMV > PCV/VCV Total PEEP PEEPe • Ventilator – settings, malfunction Circuit – kinking, water pooling, wet filter ETT – kinked, obstructed, endobronchial intubation Patient – bronchospasm, compliance (lungm, pleura, chest wall), dysynchrony, coughing Inspiratory pause pressure - Estimate of alveolar pressure Pressure • PEEPi Time Troubleshooting • Desaturation – Patient causes • All causes of hypoxic respiratory failure • Endobronchial intubation, PTx, collapse, APO, bronchospasm, PE – – – – Equipment causes FIO2 1.0 Sat O2 waveform Chest moving? • Yes – Examine patient, treat cause • No – Manually ventilate – No – ETT/Patient problem – Yes – Ventilator problem – setting, failure, O2 failure Ventilators • Maquet – – – – – – – – – VCV PCV PRVC PS/CPAP SIMV (VC) + PS SIMV (PC) + PS SIMV (PRVC) + PS MMV NAVA • Evita – – – – – PS PCV+ SIMV PCV+A Autoflow Adaptive Modes - PRVC • PCV unable to deliver guaranteed minimum minute ventilation • Changing lung mechanics + patient effort • Pressure controlled breaths with target tidal volume • Inspiratory pressure adjusted to deliver minimum target volume • Not VCV - average minimum tidal volume guaranteed • Like PCV – constant airway pressure, variable flow (flow as demanded by patient) Adaptive Modes - PRVC • • • • Consistent tidal volumes Promotes inspiratory flow synchrony Automatic weaning Inappropriate – increased respiratory drive, eg severe metabolic acidosis • Evidence – lower peak inspiratory pressures VCV vs PRVC Adaptive Modes - Autoflow • First breath uses set TV & I-time – Pplateau measured • • • • Pplateau then used V/P measured each breath Press. changed if needed (+/- 3) Dual mode similar to PRVC – Targets vol., applies variable press. based on mechanics measurements – Allows highly variable inspiratory flows – Time ends mandatory breaths • Adds ability to freely exhale during mandatory inspiration (maintains pressure) PCV + Assist • Like PCV, flow varies automatically to varying patient demands • Constant press. during each breath variable press. from breath to breath • Mandatory + patient breaths the same Inverse Ratio Ventilation • Increased mean airway pressure • Prolonged I:E ratio • Improved oxygenation – Reduced shunting – Improved V/Q matching – Decreased dead space • Heavy sedation, paralysis • Preferred PCV • Benefit – no effect in mortality in ARDS Other Modes • Adaptive support ventilation – Mandatory minute ventilation – Adaptive pressure control • Proportional assist ventilation – Pressure support (spontaneous breaths) – Pressure applied function of patient effort • Automatic tube compensation – adjusts its pressure output in accordance with flow, theoretically giving an appropriate amount of pressure support Airway Pressure-Release Ventilation • High constant PEEP + intermittent releases • Unrestricted spontaneous breaths – reduced sedation • Extreme form of inverse ratio ventilation • E:I – 1:4 • Spontaneous breaths – 10-40% total minute ventilation APRV • Settings – 2 pressure levels, 2 time durations • Uses – ALI, ARDS • Caution – COPD, increased respiratory drive APRV • Increase mean airway pressure – Alveolar recruitment, improve oxygenation • Promote spontaneous breathing – Improved V/Q match, haemodynamics • Improved synchrony • Evidence – no difference in mortality, decreased duration of ventilation High-Frequency Ventilation • 4 types – High frequency jet ventilation • Ventilation by jet of gas • 14-16G cannula, specialised ventilator • 35 psi, RR100-150, Insp 40% – High frequency oscillatory ventilation – High frequency percussive ventilation • HFV + PCV • HFOV – oscillating around 2 pressure levels • Less sedation, better clearance of secretions – High frequency positive pressure ventilation • Conventional ventilation at setting limits High Frequency Oscillatory Ventilation • Ventilator delivers a constant flow (bias flow) • Valve creates resistance – maintain airway pressure • Piston pump oscillates 3-15Hz (RR160-900) • “Chest wiggle” – assess amplitude • Tidal volumes – less than dead space • Ventilation – achieved by laminar flow • Deep sedation, paralysis HFOV • CO2 clearance – Decrease oscillation frequency, increase amplitude, increase inspiratory time, increase bias flow (with ETT cuff leak) • Oxygenation – Mean airway pressure, FiO2 • Settings – – – – – Airway pressure amplitude Mean airway pressure % inspiration Inspiratory bias flow FiO2 HFOV • Applications – ARDS – Lung protection – highest mean airway pressure + lowest tidal volumes – Ventilatory failure – FiO2>0.7, PEEP>14, pH <7.25, Vt >6ml/kg, plateau pressure >30) • Contraindicated – Severe airflow obstruction – Intracranial hypertension • Evidence – Animal models – less histologic damage + lung inflammation – Better oxygenation as rescure therapy in ARDS – No difference in mortality Mean Airway Pressure • Main factor in recruitment and oxygenation • Increased surface area for O2 diffusion • Problems – Barotrauma – Haemodynamic instability – Contraindicated patients – Deep sedation, paralysis Specific Conditions • ARDS – Definition • Diffuse bilateral pulmonary infiltrates • No clinical evidence of Left Atrial Hypertension (CWP<18mmHg) • PaO2/FiO2 of 300 or less – Exclusions • • • • – – – – – – – Unilateral lung disease Children (wt less than 25kg) Severe obstructive lung disease (asthma, COPD) Raised intracranial pressure High PEEP, low volumes + pressure SIMV(PRVC) + PS Vt 6ml/gk – check plateau pressure Pins >30cmH2O – reduce Vt Lowest plateau pressure possible RR 6-35, aim pH 7.3-7.45 Evidence – improved mortality FiO2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1.0 PEEP 5 5-8 8-10 10 10-14 14 14-18 18-22 Ventilator Induced Lung Injury • Excessive inflation pressure • Mechanical tissue damage • Inflammation – mechano-signaling due to tensile forces • Overstretching of lung units • Shear force at junction of open and collapsed tissue • Repeated opening and closing of small airways under high pressure Pathways to VILI End-Expiration Extreme Stress/Strain Tidal Forces Moderate Stress/Strain (Transpulmonary and Microvascular Pressures) Rupture Signaling Mechano signaling via integrins, cytoskeleton, ion channels inflammatory cascade Cellular Infiltration and Inflammation Marini / Gattinoni CCM 2004 Spectrum of Regional Opening Pressures (Supine Position) Opening Pressure Superimposed Pressure Inflated 0 Small Airway Collapse 10-20 cmH2O Alveolar Collapse (Reabsorption) Consolidation = Lung Units at Risk for Tidal Opening & Closure 20-60 cmH2O Lung Protection Strategies • • • • Heterogenous lung units PEEP Tidal volume Keep the lung as open as possible without generating excessive regional tissue stresses is a major goal of modern practice Prone Ventilation • Homogenise transpleural pressure • Compression – reduced compression from heart + abdomen • Improved recruitment • Increase in FRC • Decreased shunt • Benefit – Improved oxygenation in 60-80% patient, even on return to supine position – No change mortality Recruitment Manoeuvres • Open collapsed lung tissue so it can remain open during tidal ventilation with lower pressures and PEEP, thereby improving gas exchange and helping to eliminate high stress interfaces • Although applying high pressure is fundamental to recruitment, sustaining high pressure is also important • Methods of performing a recruiting maneuver include single sustained inflations and ventilation with high PEEP Three Types of Recruitment Maneuvers Specific Conditions • Unilateral lung disease – Similar approach to ARDS – Increase Insp time – improve gas distribution – Lateral position – normal lung down • Reduce shunt • Reduce normal lung compliance • Risk of contamination – Independent lung ventilator • Asthma – – – – – Maximise expiratory time, low RR – permissive hypercarbia Short inspiratory time High airway pressure - ?significance Expiratory hold Aim – PEEPi < 10cmH20, Pplat <20cmH2O • COPD – Similar to asthma – Bronchospasm not as great, reduced lung compliance Airway Obstruction • Aim – relieve work of breathing, minimise auto-PEEP • Gas trapping – – – – Increases work of breathing Haemodynamic compromise Predisposes to barotrauma Decreases ventilation • PEEP – Effects Depend on Type and Severity of Airflow Obstruction – Generally Helpful if PEEP Original Auto-PEEP – Potential Benefits • Decreased Work of Breathing • Increased VT • Improved Distribution of Ventilation NAVA • Neurally adjusted ventilatory assist • Controls ventilator output by measuring the neural traffic to the diaphragm • NAVA senses the desired assist using an array of esophageal EMG electrodes positioned to detect the diaphragm’s contraction signal • Flexible response to effort • Improves synchrony and weaning Neuro-Ventilatory Coupling Neural Control of Ventilatory Assist (NAVA) Central Nervous System Phrenic Nerve Diaphragm Excitation Diaphragm Contraction Chest Wall and Lung Expansion Airway Pressure, Flow and Volume Ideal Technology New Technology Current Technology Ventilator Unit • References – – – – Cleveland clinic journal of medicine 2009; 76(7): 417-430 UpToDate BASIC course notes Wests Respiratory Essentials • Links – – – – – – http://emedicine.medscape.com/ http://www.anaesthetist.com/anaes/vent/Findex.htm#index.htm http://en.wikipedia.org/wiki/Mechanical_ventilation http://www.merck.com/mmpe/sec06/ch065/ch065b.html http://www.ccmtutorials.com/rs/index.htm http://www.aic.cuhk.edu.hk/web8/mechanical_ventilation.htm