chest_imaging
advertisement

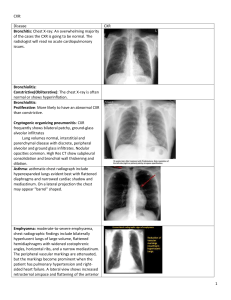
Chest imaging in pneumoconiosis NOTE In young persons or in asymptomatic patients a PA projection alone is generally used as a screening procedure. A lateral film should be obtained whenever chest disease is suspected and in screening examination of patients 40 years of age or older Male or female? Look for the presence of breast shadows (this will help you to notice a mastectomy too). Good inspiration? The diaphragms should lie at the level of the sixth ribs anteriorly. The right hemidiaphragm is usually higher than the left because the liver pushes it up Good penetration? You should just be able to see the lower thoracic vertebral bodies through the heart Is the patient rotated? The spinous processes of the thoracic vertebrae should be midway between the medial ends of the clavicles. PA films are better, particularly because the heart is not as magnified as on an AP film, making it easier to comment on the heart size. First look at the mediastinal contours - run your eye down the left side of the patient and then up the right. The trachea should be central. The aortic arch is the first structure on the left, followed by the left pulmonary artery; notice how you can trace the pulmonary artery branches fanning out through the lung Two thirds of the heart lies on the left side of the chest, with one third on the right. The heart should take up no more than half of the thoracic cavity. The left border of the heart is made up by the left atrium and left ventricle. The right border is made up by the right atrium alone (the right ventricle sits anteriorly and therefore does not have a border on the PA chest x ray film - a question that examiners love to ask. Above the right heart border lies the edge of the superior vena cava. The pulmonary arteries and main bronchi arise at the left and right hila. Enlarged lymph nodes can also occur here, as can primary tumours. These make the hilum seem bulky Now look at the lungs. Apart from the pulmonary vessels (arteries and veins), they should be black (because they are full of air). . Force your eye to look at the periphery of the lungs - you should not see many lung markings here; if you do then there may be disease of the air spaces or interstitium. Make sure you can see the surface of the hemidiaphragms curving downwards, and that the costophrenic and cardiophrenic angles are not blunted - suggesting an effusion. Check there is no free air under the hemidiaphragm Finally look at the soft tissues and bones. Are both breast shadows present? Is there a rib fracture? This would make you look even harder for a pneumothorax. Are the bones destroyed or sclerotic? There are only two spaces to look at on the later- al film. The heart lies antero-inferiorly. Look at the area anterior and superior to the heart. This should be black, because it contains aerated lung. Similarly the area posterior to the heart should be black right down to the hemidiaphragms. The blackness in these two areas should be equivalent; therefore you can compare one with the other. If the area anterior and superior to the heart is opacified, suspect disease in the anterior mediastinum or upper lobes. If the area posterior to the heart is opacified suspect collapse or consolidation in the lower lobes. normal Pneumoconiosis (Lung Dust) Refers to the pulmonary manifestations of exposure to a variety of dusts or aerosols Silicosis Coal workers pneumoconiosis Asbestosis Berylliosis Siderosis CXRPneumocon iosis- based on ILO classification standards The accepted means of quantifying dust exposure and retention-very important in evaluating disability claims Profusion of opacities categorized as 1, 2, or 3 with a second subclassification to indicate degree of certainty (1, 0/0, 0/1; 1/0, 1/1, 1/2, etc.,) Size Rounded/regular; p <1.5 mm , q 1.5-3 mm, or r >3 to 10 mm (these are more specific for dust exposure) Irregular opacities; s, t, or u based on the same sizes Larger opacities are classified as A (1-5 cm), B (>5 cm), or C (equivalent to the entire RUL zone) Progression of disease is usually associated with a change in profusion, and not size of opacities Presence/degree of pleural thickening classified as A (<5 mm), B (5-10 mm), C (>10 mm) silicosis Silica: active dusts .fibrogenic Silicosis has a progressive nature despite cessation of dust exposure X-ray picture is of multiple small rounded opacities Usually in the upper lobes May occasionally calcify (20%) Lymph node enlargement is common Large opacities are conglomerations of small opacities Progressive Massive Fibrosis (PMF) Cavitate from tuberculosis or ischemic necrosis Massive fibrosis and conglomerate mass formation in upper lobes with scarring and retraction of hila upwards Eggshell calcification of hilar nodes in 5% Caplan’s syndrome consists of large necrobiotic nodules superimposed on silicosis Silicosis predisposes to TB The radiologic findings of tuberculosis developed in the patients with silicosis include pleural effusion, newlydeveloped consolidation, bronchovascular infiltrations, cavitary change in pre-existing PMF, etc. C.W.P Coal dusts: A combination of active and inert material Coal dust is deposited in the alveolar macrophages which migrate to, and leave, coal dust deposits around the respiratory bronchiole Here a very small fibrous reaction occurs Complicated CWP occurs as large masses in either the upper lobes or the superior segments of the lower lobes Unlike silicosis, the large upper lobe lesions of CWP are single (rather than conglomerate) black masses with a liquid core, not a fibrous tissue core The masses may undergo cavitation either from TB or ischemia The rounded opacities of CWP, found predominantly in the upper lobes Massive fibrosis are round or oval and tend to migrate toward the hila creating peripheral areas of emphysema and bulla. Asbestosis Asbestos particles invoke a hemorrhagic response in the lung Fibers are then coated with a ferritin-like material resulting in ferruginous bodies Does its damage in respiratory bronchioles and alveoli Affects lower lobes first Opacities are small and irregularly shaped Cardiac silhouette may become shaggy Almost all patients have some pleural involvementpleural plaque, diffuse pleural thickening, calcification or effusion Pleural involvement without parenchymal disease is common Parietal pleural plaques in the mid lung are the most common asbestos-related disorder and are usually bilateral Pleural calcification occurs in about 50% with asbestos-related disease, especially diaphragmatic pleura Diffuse pleural thickening involves diaphragmatic pleura, blunting of costophrenic sulci and lateral chest wall thickening Effusion alone may occur early in the disease (first 20 years) in about 3% of cases Asbestos-related lung cancer is either squamous cell or adenocarcinoma Bronchogenic ca is almost always associated with cigarette smoking In contrast to silicosis, hilar lymph nodes are rarely affected HRCT:thickend interlobular septal lines,curvilinear subpleural lines,parenchymal bands and honycombing. Asbestos and Cigarette Smoking Interaction on Chest X-ray ILO Category Asbestos causes pulmonary fibrosis, while smoking usually causes emphysema (destruction of alveolar surface area). In those with asbestosis who have also been heavy smokers, there is (on average) an increase in the profusion of small linear opacities on chest x-ray. A smoker may have one half category higher profusion than a non-smoker with equivalent asbestos exposure Egg shell PMF(silicosis) normal This picture shows complicated coal workers pneumoconiosis. There are diffuse, massive light areas that run together in the upper and middle parts of both lungs. These are superimposed on a background of small and poorly distinguishable light areas that are diffuse and located in both lungs. Diseases which may explain these X-ray findings include, but are not limited to: complicated coal workers pneumoconiosis (CWP), silico-tuberculosis, and metastatic lung cancer Pneumoconiosis (Radiographic type p) normal Routine torax X-ray(PA and Lateral) from a 52 yo male assymptomatic patient with asbestosis HRCT scan (left) shows thickened intra- and interlobular lines (A). HRCT (right) shows subpleural curvilinear density. (B) This PA radiograph shows some of the typical findings of asbestosis including a "shaggy heart", pleural plaques and diaphragm calcification This picture shows complicated coal workers pneumoconiosis. There are diffuse, small, light areas (3 to 5 mm) in all areas on both sides of the lungs. There are large light areas which run together with poorly defined borders in the upper areas on both sides of the lungs. Diseases which may explain these X-ray findings include complicated coal workers pneumoconiosis (CWP), silico-tuberculosis, disseminated tuberculosis, metastatic lung cancer, and other diffuse infiltrative pulmonary diseases. Caplan Description: X-ray showing lung nodules in a patient with RA (note differential diagnosis: Wegener's granulomatosis, metastatic cancer (eg kidney)TB) Small rounded opacity Small rounded opacity caplan 55 year old man who was pensioned early from his job as a coal worker. Features in the image There are well defined nodules in both lungs with a mid-zone predominance. The nodules appear more confluent in the left upper zone, where larger ill-defined masses are present, distorting and elevating the left hilum. Both hila appear enlarged and lobulated. Although the overlying nodules may make the hila look large, the present appearance suggests hilar lymphadenopathy. In addition to the slightly prominent basal segment lower lobe bronchial markings, there is the appearance of additional perihilar strands. A horizontal line, crossing the basal vessels, is probably a linear fibrotic scar. DX: Pneumoconiosis,silicosis developing massive fibrosis not pure anthracosis,which produces less fibrotic reaction This chest X-ray shows coal workers pneumoconiosis -. There are diffuse, small (2 to 4 mm) light areas on both sides of the lungs. Diseases which may explain these X-ray findings include simple coal workers pneumoconiosis (CWP) simple silicosis, disseminated tuberculosis, metastatic lung cancer, and other diffuse infiltrative pulmonary diseases. Carcinoma brounchus,arising in old tuberculosis with pleural effusion Clinical presentation: 53 year old man working as a heating engineer/fitter cutting asbestos templates. He smokes 10 cigarettes a day. There was a history of tuberculosis treated 25 years earlier. Recently, he complains of a slowly increasing pain on the left side of his chest. Features in the image The right lung is large volume, but the left lung has reduced volume. The left hemidiaphragm silhouette has been lost. There is pleural shadowing that blunts the left costo-phrenic angle and extending a 'meniscus' into the left axilla. There is scattered calcific shadowing at both lung apices. The upper lobe vessels are crowded, implying some fibrotic shrinkage of the upper lobes. On the right side the visible hilum is drawn up, but the left hilar point is depressed. A poorly defined soft tissue density is projected behind the left first rib and another larger density behind the heart. Calcified pleural plaques are seen in profile above the right hemidiaphragm and some are partly obscured by the pleural shadowing on the left side. Elderly male, former pottery maker There are multiple fairly dense nodules, mostly in both mid and lower zones. The right hilum appears bulky with some lobulation lateral to the main bronchi. This resembles hilar lymphadenopathy, despite the enlarging effect that overlying nodules have on the hilar appearance. There are additional radiating strands, extending from the right hilum, perhaps too thick for 'Kerley B' lines, but not corresponding to dilated bronchi alone. The vessel count in the left upper lobe is reduced and there is amorphous calcific shadowing at the left apex. The left hilum is distorted, undersized and is associated with a horizontal strand of fibrosis in the left mid-zone. Dx:silicosis,with perihilar interstitial shadowing. Old tuberculosis of the left upper lobe.possible early bronchiectasis. Chest X-ray of retired coal miner demonstrates Coalworker’s Pneumoconiosis with Progressive Massive Fibrosis Normal Chest ( X-Ray ILO Category 0/0) Interaction of Asbestos and Cigarette Smoking to Increase X-ray Markings (Asbestosis, ILO Category 2/2)