ELECTROCARDIOGRAM
advertisement

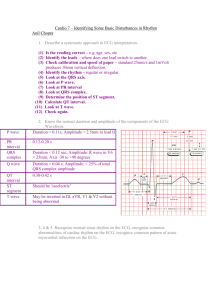
Generation of action potential ECG Graph paper Unipolar precordial leads Normal ECG Guide in Reading ECG • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias Standardization Heart rate bradycardia tachycardia PR interval QRS QRS axis QTc 60 - 100 beats/min < 60 > 100 0.12 – 0.20 sec < 0.12 sec - 30º to + 110º < 0.47 sec males < 0.48 sec females Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias Rhythm SA node – sinus AV node – junctional Ventricular rhythm Rhythm Are there p waves? sinus, atrial fibrillation Do they look similar? MFAT, wandering pacemaker Are they regular? AF Does a QRS complex follow each p wave? SVT, junctional rhythm, ventricular rhythm Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias Determination of Heart Rate Heart rate assessment by “rule of 300” Measurement of Rate • Formula 1: 300 # big squares between R-R • Formula 2: 1500 # small squares between R-R Determination of Heart Rate • Is the atrial rate same as ventricular rate? – PVC’s, PAC’s, 3rd degree AV block • Is there normal-looking QRS complex after each p wave? • What if there are no p waves? – Six second strip heart rate RATE 1. Sinus Bradycardia 2. Sinus Tachycardia 3. AV junctional rhythm - Inherent rate of 40-60/min No p waves Normal looking QRS complex 4. Ventricular rhythm - Inherent rate of 20-40/min No p waves Bizaare-looking QRS complex Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias Determination of Axis Hexaxial System QRS axis Vectorial Analysis Determination of Axis Axis = 90 x QRS in AVF QRS in [ I] + QRS in [AVF] Special cases: • negative QRS deflection in I – Add 90 to result Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias P wave morphology and duration • No p waves – Atrial fibrillation • Multiple p waves – Multifocal atrial tachycardia – Wandering pacemaker • Notched p wave – Left atrial enlargement • Peaked p wave – Right atrial enlargement Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias P-R Interval P-R interval • Prolongation – Hypokalemia – 1st degree AV block • Shortening – Wolff-Parkinson White Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias QRS morphology and duration • Normal looking – Supraventricular origin • Bizarre looking – Ventricular in origin – Paced rhythm Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias ST segment • Elevation – Infarction • >1mm in limb leads • >2 mm in chest leads • depression – Ischemia • >1 mm in all leads from the J point Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias T and U waves • T wave – Hypokalemia – 1st degree AV block • Shortening – Wolff-Parkinson White Guide in Reading ECG • • • • • • • • • • • • • Standardization & technique Rhythm Rate: atrial & ventricular Axis P wave morphology & duration P-R interval QRS complex morphology & duration ST segment T-wave U wave Q-T interval Hypertrophy and enlargement arrhythmias Determination of QT interval Corrected QT interval = QT (actual) R-R QT interval • prolongation – hypocalcemia • shortening – hypercalcemia Chamber Enlargement Atrial Enlargement (due to chronic lung disease or pulmonay embolus Atrial Enlargement (commonly seen in mitral valve disease) B V1 II V1 Ventricular Enlargement Ventricular Enlargement Right Ventricular Hypertrophy R in V1 + S in V5-V6 >11 mm R in V1 >7mm R:S in V1 >1 RAD > +90 degrees Ischemic Heart Disease Anatomy of Myocardial Infarction Infarction area ECG leads Coronary Artery Branch Extensive anterior Anteroseptal Anterolateral Inferior A, AVL, V1 – V6 Left, LM LAD, LCX V1 – V4 I, AVL, V3 – V6 II, III, AVF LAD LCX PDA True posterior V1 – V2 (reciprocal) V3 – V4 Left Left Right 80% Left 20% Variable left/right Left Anterior LCX PL LAD *LAD = left anterior descending aretery; LCX = left circumflex artery LM = left main artery; PDA = posterior descending artery; PL = posterolateral branches Evolution of Infarct 1. 2. 3. 4. 5. ST segment elevation Progressive decrease in ST segment elevation Q wave formation T wave flattening/inversion Q wave with upright T wave Significant Q wave RULES on Q waves • Not significant in aVR • Ignored in V1 unless with abnormalities in other precordial leads • Ignored in III unless with abnormalities in II, AVF more reliable if with St-T segment changes • Not significant if located in V1-V3 in LBBB • Significant in V1-V2 in the presence of RBBB • Pathologic if >= 0.04 sec and >25% of R wave amplitude RHYTHM DISORDERS ATRIAL Arrhythmias 1. 2. 3. 4. Atrial fibrillation Atrial flutter Wandering Pacemaker Multifocal Atrial tachycardia ATRIAL FIBRILLATION - - - Most common sustained arrhythmia associated with increased CV mortality and morbidity Prevalence increasing with age, doubling with each successive decade, 70% in ages 65-85 Multiplier effect on risk - - 3-5x stroke 3x CHF 1.5-3x death Associated with heart disease but ~30% are without underlying heart disease ATRIAL FIBRILLATION - Rapid and irregular atrial fibrillatory waves at a rate of 350 to 600/minute CRITERIA - - Absent P waves F waves vary in amplitude, morphology and intervals R-R intervals are irregularly irregular Ventricular rate usually ranges from 90-170 QRS complexes are narrow unless AV conduction is abnormal Hypothesized to be due to multiple wavelets in the atrium competing for the conduction to the AV node ATRIAL FIBRILLATION ATRIAL FLUTTER - Atrial rate of 220 to 350/minute CRITERIA - Absent p waves Biphasic saw-toothed flutter waves, fairly regular F waves vary in amplitude, morphology and intervals R-R intervals are irregularly irregular Ventricular rate usually ranges from 90-170 QRS complexes are narrow unless AV conduction is abnormal Hypothesized to be due to multiple wavelets in the atrium competing for the conduction to the AV node ATRIAL FLUTTER Escape Rhythm/Beat 1. Atrial - Sinus arrest causing escape rhythm With p’ waves 2. Junctional - No P waves 40-60/min inherent rate Produces a series of lone QRS complexes 3. Ventricular - may occur in complete AV block Escape Rhythm/Beat Sinoatrial block - Complete failure of a P wave to appear A cycle appears which is twice the anticipated P-P interval Transient doubling of P-P interval - SA exit block - No visible P-QRST complex for more than 1 cycle Normal P wave morphology, before and after the pause Pause is preceded and followed by a normal PP cycle P-P interval is a mutliple of the normal P-P interval SA block SINUS ARREST vs SINUS PAUSE Wandering Pacemaker - - Impulses originate from different foci in the atrium and even AV node Sinus node may still be dominant >= 3 P wave morphologies, with varying P-R intervals, resulting in varying R-R intervals Heart rate <100 May be seen in - Increased vagal tone Digitalis effect Organic heart disease Wandering Pacemaker Multifocal Atrial Tachycardia - Irregular atrial rate > 100 P wave shows >= 3 different morphologic patterns and varying PR intervals Varying P-P and P-R intervals result in avrying R-R intervals Multifocal Atrial Tachycardia HEART BLOCKS 1. 1st degree 2. 2nd degree - Type 1 Wenkeboch Type 2 Mobitz II 3. Complete AV block 4. Bundle Branch Block - Right bundle branch block Left bundle branch block 5. Hemiblocks - Left anterior hemiblock Left posterior hemiblock • 1st degree – PR interval > 0.20s • 2nd degree (type1 and 2) – Type 1 – PR interval becomes longer until depolarization is not conducted anymore – Type 2 – AV conduction is blocked • 3rd degree – AV dissociation – Variable PR and RP intervals – QRS rate is usually constant and lies within the range of 1570 beats /min Trifascicular Conduction System Right Bundle Branch Block • Lead V1 pattern) • Lead V6 • Lead I late intrinsicoid, M-shaped QRS (RSR early intrinsicoid, wide S wave wide S wave Right Bundle Branch Block • Associated with – – – – – – – RHD Cor pulmonale/RVH Myocarditis IHD Degenerative disease of the conduction system Pulmonary embolus ASD Right Bundle Branch Block Left Bundle Branch Block • Lead V1 • Lead V6 R • Lead I QS or rS late intrinsicoid, no Q waves, monophasic monophasis R, no Q wave Left Bundle Branch Block • Associated with – CAD – HHD – Dilated cardiomyopathy -- unusual for LBBB to exist in the absence of organic disease Left Bundle Branch Block Left Anterior Hemiblock • • • • • LAD (usually -30 to -60 degrees) Small Q in leads I and aVL, small R in II, III and aVF Usually normal QRS duration Late intrinsicoid deflection in aVL Increased QRS voltage in limb leads Left Anterior Hemiblock • Usually benign in the absence of apparent organic heart disease and not associated with block in the other fascicles • Can also occur in – – – – – CAD Chagas disease Infiltrative and inflammatory diseases CHDs Sclerodegenerative disorder Left Anterior Hemiblock Left Posterior Hemiblock • • • • • • RAD (usually + 120 degrees) Small R in leads I and aVL, small Q in II, III and aVF Usually normal QRS duration Late intrinsicoid deflection in aVF Increased QRS voltage in limb leads No evidence of RVH Left Posterior Hemiblock • Can occur in – – – – – Cardiomyopathies Myocarditis Hyperkalemia Acute cor pulmonale chronic degeneerative and fibrotic processes of the conducting system – Aretriosclerotic cardiovascular disease Left Posterior Hemiblock Bifascicular Block • Complete LBBB • RBBB with either LAHB or LPHB • Duration of QRS complex is prolonged to 0.12s Bifascicular Block Trifascicular Block • Bifascicular block associated with 1st degree AV block Trifascicular Block Premature Complexes 1. Premature Atrial Complex 2. Junctional Premature Beats 3. Ventricular Premature Beats Premature Complexes - PACs - Premature atrial activation arising from a site other than the sinus node P wave occuring relatively early in the cardiac cyle - with a different morphology from the sinus P wave - PR interval different from that during the sinus rhythm Premature Complexes - PACs - Not life-threatening by themselves But may also start a VT May be asymptomatic or cause a sensationof “skipping” or palpitations May be associated with normal conduction or aberrant conduction Premature Complexes - PACs Premature Complexes – Junctional Premature Beats - Arise from the AV node or in the His bundle A premature normal QRS complex is closely accompanied by an “upside down” P wave Premature Complexes – Ventricular Premature Beats - Duration of more than 0.12s Bizarre morphology T wave in the opposite direction from the QRS vector A fully compensatory pause Ventricular bigeminy, trigeminy, quadrigeminy, couplet Premature Complexes – Ventricular Premature Beats - May be present in - Normal individuals MVP Hypertension and LVH Chronic HD Acute MI cardiomyopathy Miscellaneous • Poor R wave progression – < 3mm R wave in V3 • Low QRS – < 5mm QRS amplitude in limb leads – <10mm QRS amplitude in chest leads