File
advertisement

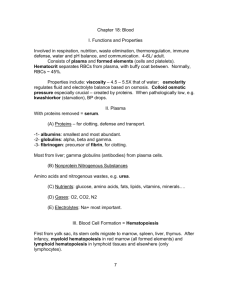
Lecture 16 • RBC (Erythrocytes). Are circular, biconcave and non-nucleated. RBC being biconcave allows alteration in cell volume so it can resist hemolysis. If there is any change in osmotic pressure, it can resist hemolysis. • Easy folding of RBCs to pass through capillaries (minute blood vessels); haemoglobin seen in RBC is distributed evenly so that the exchange of gases can take place. Exchange of oxygen and carbon dioxide. • The mature RBCs (reticulocytes) has no nucleus and has no mitochondria but it can live for 120 days. How does it survive? This RBC depends totally on glucose metabolism = facilitated diffusion across the cell membrane. It is carrier mediated process. • Although RBC has no metabolism, it has cytoplasmic enzymes to metabolize and use oxygen. • There are pores that allow access for water and electrolytes. Below CM you can see a layer of contractile protein called spectrin. Spectrin maintains the flexibility and shape of RBC.Some blood group specific substances called antigens. • Proteins such as glutathiones and albumin-like insoluble proteins can be seen in RBC; prevent damage to haemoglobin. Some enzymes – carbonic anhydrase and catalase. • Function of carbonic anhydrase is CO2 transport. Catalase decomposes hydrogen peroxide to water and oxygen. • Derivatives ions can be seen in this composition. • Osmotic fragility of RBC with respect to solution: isotonic solution is 0.9% NaCl, 5% glucose, 10% mannitol and 20% urea. Nothing happens with the RBC. Osmotic pressure in isotonic solution = osmotic pressure within RBC. • Hypotonic solution: burst. Hypertonic solution: shrinkage of RBC. • Variation in size, shape and structure of RBCs (in notes). • The tumor of the bone marrow -> polycythemia vera/ erythrocemia. RBC > 6 million/ccm (7-8 million/cmm). • When RBCs are lead poisoned, 1) punctuate basophilic – basophilic granules. 2) Cabots ring – ‘8’ like ring in cytoplasm. 3) Howell-jolly – nuclear fragments in cytoplasm. • Haemopoesis: development of RBCs and blood cells. It includes erythropoiesis, leukopoeisis, thrombopoesis/megakaryocytopoesis (big, multi-nucleated cell). • Theories to explain haemopoesis: 1) monophyletic theory. 2) polyphyletic theory. Monophyletic theory: according to theory, a single ancestral cell is responsible to give rise to all three blood cells (RBCs, WBCs, platelets). That single ancestral cell is pleuripotent stem cell, seen in bone marrow. 75% of cells in bone marrow are WBCproducing myeloid series. Another 25% are RBCS producing erythoid series. • Pleuripotent stem cell/multipotent stem cell/haemocytoblast. • Something has to act on multipotent stem cell to commit it to a specific type of cell: whats acts on it is interleukins. Interleukins convert multipotent to unipotent committed stem cell. Interleukins are hormone-like chemical messengers with known amino acid sequences. Interleukins are produced by lymphocytes, macrophages and endothelial cells, neurons, glial cells... • Interleukins are the same as cytokines, functionally same as cytokines. Within cytokines theres a single factor whose amino acid is not known yet. • Early cytokines are termed as lymphokines. Later when they further researched, some cells produced messengers. Thats why its termed cytokines. • Interleukins act on IL-1, IL-6, IL-3 sequence, convert them to committed stem cell. RbC , WBC and platelets. • The colony stimulating factors are growth factors/hormones that cause an appropriate single stem cell to proliferate in culture medium; to give rise to colonies of daughter cells = RBCs, WBCs and platelets. • Polyphyletic – The RBC, WBC all have their own stem cells. • Erythropoesis: development of RBCs. During intra-uterine life: includes 3 stages – mesoblastic, hepatic and myeloid. Mesoblastic stage: up to 3 months of fetal life, developed from mesoderm of yolk sac -> area vasculosa. “Intravascular erythropoeisis” erythropoeisis can be seen within the blood vessels. Hepatic: liver and spleen would be sites for development of erythrocytes. Nucleated RBCs, undifferentiated cells, develop into various connective tissues. Myeloid: now the bone marrow is the site of RBC formation. This is extravascular erythropoesis. • is active. In children: the red marrow is the site of red cell production = red marrow • In 18-20 years -> end of long bone, shaft converted into yellow marrow. Yellow marrow -> fat cells, which is inactive. • During the maturation of RBCs, some changes...the cell size decreases as it attains maturity. Initially in hemocytoblast, nucleus is very big with open chromatin, many nucleoli. As cells attains maturity nucleus disappears, chromatin degenerates, no more nucleus. Cytoplasm amount increases as cell attains maturity. The stain of the cytoplasm starts from deep basilic to polychromatophilic and later it ends up acidophilic. The reason for that staining change is due to reduction in total RNA amount. •