Bone ossification
Bone formation has two methods – intramembraneous (skull bones and clavicle) and endochontral
(most bones) ossification. These form the bones of the body.
Around the time of birth, secondary ossification sites appear, which further grow the bone. Even
into early adulthood, when the bone stops growing in length, they can still respond to stress and
grow in diameter by appositional growth.
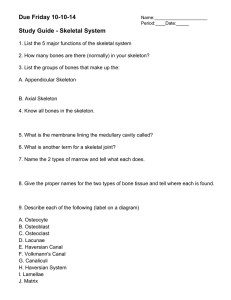
Intramembraneous ossification (involves the replacement of sheet like connective tissue membrane
to bone tissue)
Starts when some embryonic connective tissue (mesenchyme) condense into a sheet of soft
tissue with a dense blood supply.
The cells of this sheet enlarge and differentiate into osteogenic cells, whilst some
differentiate to form a soft network of trabeculae.
Osteogenic cells gather on these trabeculae and form osteoblasts, and deposit organic
matrix called osteoid tissue (similar to bone, but lacking minerals).
Minerals are deposited, and some osteoblasts become trapped in lacunae (then
differentiate into osteocytes).
Some of the calcified trabeculae form permanent spongy bone.
Osteoclasts work on these trabeculae, remodelling them in areas to form marrow cavities.
At the surface trabeculae continue to calcify until they become compact bone.
NB: this gives typical structure of cranial bone – spongy bone, sandwiched by compact bone.
Mesenchyme at the surface become increasingly fibrous, until they give rise to the
periosteum.
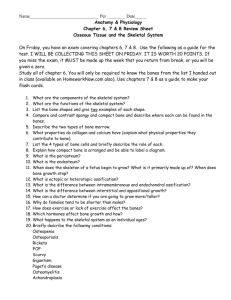
Endochondral Ossification (involves a hyaline cartilaginous model of bone first that is ossified into
bone) – has primary and secondary ossification regions.
Primary ossification centre:
Starts with the multiplication and swelling of chondrocytes near the centre of the model,
forming the primary centre.
As the lacunae enlarge, the matrix b/w them is reduced to thin walls, making the whole
model weak.
But then some cells of the perichondrium (the periosteum of the cartilaginous bone model)
become osteoblasts and form a bony supporting collar around the model.
NB: once this collar has formed, the fibrous sheath is now considered to be periosteum,
instead of perichondrium.
Buds of connective tissue grow from this periosteum and invade into the thin walls b/w the
enlarged lacunae.
They break down the lacunae and transform the primary ossification centre into a cavity
called the primary marrow space.
Osteogenic cells then invade the model by the connective tissue buds that came in
previously, transform into osteoblasts and line the marrow space.
Osteoblasts deposit osteoid tissue (like bone matrix without the toughening minerals),
which soon is calcified to form trabeculae.
As bone develops, these regions are broken down and modelled by osteoclasts to form the
medullary cavity.
At the metaphysis, b/w the cartilaginous head and the shaft, there are 5 regions in which
(from the furthest from bone centre) cartilage is resting, chondrocytes are proliferating,
getting larger (pushing the bone to make its ends longer), its surrounding matrix is being
calcified, they are dying and being replaced by bone.
NB: in an osteon, the outer rings of lamellae are deposited first, so they inner most ones are
the youngest.
Secondary ossification centre:
Around the time of birth, secondary ossification centres begin to form in the epiphysis.
Similarly, there the chondrocytes enlarge, the walls of the matrix dissolve and it dies.
Vascular buds arise from the perichonrium and grow into the cartilage, bringing osteogenic
cells and osteoclasts.
The cartilage is eroded away from the centre of the epiphysis outward in all directions.
Hyaline cartilage is retained b/w the ephiphysis and the diaphysis – epiphyseal plate, and on
the ends of the bone.
Bone Growth and Remodelling
Interstitial growth lengthens the bone by growing the epiphyseal plate.
However in mature bone, only appositional growth occurs – growth on the surface, usually
to increase bone diameter.
Clinical Features
Achondroplastic Dwarfism: where the long bones of the body stop growing during childhood, whilst
other bones grow normally. So patients have shortened limbs, but normal portion of head and trunk.
This occurs due to the failure of cartilage growth, which helps lengthen bone. This occurs due to a
spontaneous mutation (no history is required to get it). However, this mutant gene is dominant, so
heterozygous dwarf has 50% chance of having a child who is also a dwarf.
Bone maintenance
Mineral deposition
Process by which Ca and phosphate ions are deposited in bone from blood. Osteoblasts produce
helical rings of collagen, onto which calcium phosphate and other minerals get deposited onto.
However, calcium phosphate doesn’t mineralize out of solution unless its tissue fluid
concentration reaches a critical level called the solubility product. Once some crystallization starts,
more continue – it’s a positive feedback. Most tissue have inhibitors to prevent unwanted
calcification. Osteoblasts apparently neutralize these inhibitors.
Ectopic ossification is abnormal ossification in the lungs, brain, eyes, muscles, tendons, arteries or
other organs i.e. calcification in arteries = atherosclerosis.
An ossified mass in an otherwise soft organ (e.g. lung) is called a calculus.
 0
0