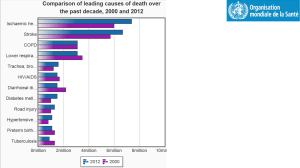
stroke_htn1

Proposed Institutional Guidelines for Managing Hypertension in Patients with
Stroke Based on AHA/ASA Guidelines
Ischemic Stroke, No Reperfusion Therapy
BP Level
Target BP
Recommended IV antihypertensive options
SBP > 220 mm Hg or DBP>120 mm Hg
Reduce BP by 15% - 25% within 24 hours
Nicardipine 5 mg/hr; titrate up by 2.5 mg/hr every 5-15 minutes to a maximum of 15 mg/hr until desired BP achieved.
Labetolol, 10 mg followed by continuous infusion at 2-8 mg/min
Consider nitroprusside if resistant. Start at 0.3 mcg/kg/min and titrate slowly.
Ischemic Stroke with Reperfusion Therapy
BP Level
Target BP
Recommended IV antihypertensive options
BP Level
Target BP
Recommended IV antihypertensive options
SBP > 185 mmHg or DBP > 110 mmHg
SBP > 185 mmHg or DBP > 110 mmHg
Nicardipine 5 mg/hr; titrate up by 2.5 mg/hr every 5-15 minutes to a maximum of 15 mg/hr until desired BP achieved.
Labetolol, 10 mg followed by continuous infusion at 2-8 mg/min
Other agents (hydralazine, enalapril) when appropriate
Hemorrhage Stroke with ICH
SBP > 200 mmHg or MAP > 150 mmHg: Aggressive reduction with continuous IV therapy
If increased ICP suspected and SBP > 180 mm Hg or MAP > 130 mmHg: Intermittent or continuous IV therapy while maintaining CPP at ≥ 60 mmHg
SBP > 180 mmHg or MAP > 130 mmHg and no evidence of elevated
ICP: Consider intermittent or continuous IV therapy to achieve moderate BP reduction
BP < 160/90 mm Hg or MAP < 110 mmHg
Nicardipine or Labetolol
BP Level
Target BP
Recommended IV antihypertensive options
SAH
Unclear
One prehospital study suggested SBP > 160 mmHg
Unclear
Administer short acting continuous intravenous infusions of
Nicardipine, Labetolol, Esmolol