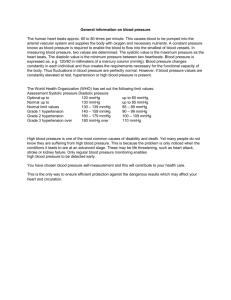
Heart Disease and Stroke Prevention
advertisement

Dr. Yoga Nathan Public Health UL 160/95 mm Hg? 140/90 mm Hg? How can we define `Hypertension’ or `High blood pressure’? BY DEFINING THE BP LEVEL ABOVE WHICH IT IS BENEFICIAL TO REDUCE BP This the definition generally used Arbitrary definition, changing over time 1950s DBP 120 1960s DBP 110 1980s DBP 100 SBP 160 Now DBP 90 SBP 140 A small proportion of individuals with high blood pressure have a specific medical cause (secondary hypertension): <1% in general population <5% in medical clinics The rest have no specific medical cause (primary or essential hypertension) a) b) c) d) e) f) g) h) -Coarctation of aorta -Renal and renal vascular disease -Adrenal disease cortical 1 hyperaldosteronism, Cushing’s syndrome medulla phaeochromocytoma -Pregnancy -Drugs esp OCP, HRT Rural communities in less developed settings Hunter gatherer, subsistence diet low in fat, salt, alcohol Low mean body mass index High physical activity Low stress levels (?) -Generally show that blood pressure patterns change (increase) to those of the host population: * * * Change generally occurs within 6 months Strong evidence for ENVIRONMENTAL influence on population BP May be exceptions – high BP in AfricanCaribbeans may have genetic basis -High body mass index -High alcohol intake -High salt intake -Low potassium intake -Low fibre/high fat -Physical inactivity -Stress SBP higher by:- 15 mmHg 8 mmHg 5 mmHg 5 mmHg 2-3 mmHg 2-3 mmHg ???? Age being older Ethnicity African-Caribbean Family history positive Body mass Overweight/obese Alcohol intake high Which is more strongly related to risk, systolic or diastolic? -Both are important, systolic slightly more so -In older people, `high’ systolic BP can occur with `normal’ diastolic pressure (isolated systolic hypertension), is associated with increased CV risk How strong are the relative risks of high blood pressure (60-69 years)? -Usual systolic BP 20 mmHg higher: relative risk of stroke 2.32 relative risk of CHD 1.85 -Usual diastolic BP 10 mmHg higher: relative risk of stroke 2.50 relative risk of CHD 1.79 Applies above SBP 115, DBP 75 mmHg Prospective Studies Collaboration, Lancet 2002 Percent of Population 25 20 90th percentile 15 10 95th percentile 5 0 80 120 100 140 160 180 Systolic Blood Pressure (mm Hg) Source: NHANES II 200 Stroke Rate per 1,000 Population 12 10 8 6 4 2 0 <120 120-139 140-159 160-179 Systolic Blood Pressure (mm Hg) Source: Framingham Heart Study, 1980 180+ Mortality From CHD (No./10,000 Person Years) 140 130 120 110 100 90 80 70 60 50 40 30 20 10 0 110 United States Northern Europe Mediterranean southern Europe Inland southern Europe Serbia Japan 120 130 140 150 Systolic Blood Pressure (mm Hg) 160 170 (Adjusted for age, serum TC, current smoking status for each quartile) Van den Hoogen PCW, et al, for the Seven Countries Study Research Group. N Engl J Med. 2000;342:1-7. DIES 16 yr Lost 150/100 9 yrs 140/95 4 130/90 120/80 0 10 20 Build/Bp Study: 1935-1954;Metropolitan Life 30 40 50 Hypertension • Angina pectoris • Unstable angina • Myocardial infarction • Sudden death • Heart failure • TIA • Ischemic stroke • Hemorrhagic stroke • Renovascular disease • Renal failure • Claudication • Aneurysm • Critical limb ischemia -Coronary (ischaemic) heart disease -Stroke (all types) -Ischaemic stroke -Haemorrhagic stroke -Subarachnoid haemorrhage -Heart failure -Hypertensive heart disease -Sudden death -Renal failure -(All-cause mortality) How do we know this? Population-Based Strategy SBP Distributions Before Intervention After Intervention Reduction in BP Reduction in SBP % Reduction in Mortality mmHg Stroke CHD Total 2 3 5 -6 -8 -14 -4 -5 -9 -3 -4 -7 Hypertension 1991;17:I-16–I-20. SOURCES OF DIETARY SALT Water 1% Other Sodium 3% Table Salt 9% Cooking Salt 6% Processed Food 81% Source: James et al. The dominance of salt in manufactured food in the sodium intake of affluent societies. Lancet 1987;8530:426-428. Raised blood pressure is the biggest single cause of cardiovascular disease accounting for 62% of strokes and 49% of heart disease. Strokes and coronary heart disease kill more people around the world than any other cause of death – around 12.7 million people each year. It is estimated that reducing salt intake by 6g a day could lead to a 24% reduction in deaths from strokes and an 18% reduction in deaths from coronary heart disease, thus preventing approximately 2.6 million stroke and heart attack deaths each year worldwide. Preventable Treatable Controllable Why is so Difficult to Do? Sustained reduction in blood pressure over about 5 years effectively reverses the risks of the higher pressure -If usual diastolic BP 10 mmHg lower:relative risk of stroke reduced by about 60% relative risk of CHD reduced by about 44% Greater BP reduction gives greater CV risk reduction -Similar BP reduction (e.g. 10 mmHg) will reduce relative risk of CVD by similar amount, whatever the starting blood pressure Because the relations of BP and CVD risk are continuous there is no rational target for BP reduction (pragmatic targets for patients on treatment) Br Hyp Soc SBP <140 DBP < 85 mmHg Who should have their BP lowered? -The traditional view: The reason for lowering blood pressure is that it is high…. `People who need their blood pressure lowered are those who have a high blood pressure’ -The new view The reason to lower blood pressure is to reduce the risk of cardiovascular disease `People who need their blood pressure lowered are those who are at high risk of cardiovascular disease (almost irrespective of their blood pressure)’ -The third (middle) way `Blood pressure should be treated on its merits but should take account of overall CV risk’ Lifestyle Modifications Modification Approximate SBP Reduction (range) Weight Reduction 5-10 mmHg/10kg Adopt DASH eating plan 8-14 mmHg Dietary sodium reduction 2-8 mmHg Physical activity 4-9 mmHg Moderation of alcohol consumption 2–4 mmHg Responsibility for a Problem (Who is to blame?) Self Responsibility for a Solution (Who will control the future?) Self Other Other Moral Model Compensatory Model • Person feels lazy • Person needs motivation • Person feels deprived • Person needs power (skill) Enlightenment Model Medical Model • Person feels guilty • Person needs discipline • Person feels ill • Person needs treatment * Brickman, American Psychologist 37(4):368–384, April 1982. Patient believes – His diagnosis – Hypertension is serious – In the efficacy of medicine – He can control HBP with doctor’s help. Patient doesn’t understand the difference between control and cure. He thinks he’s “cured”. Patient receives no call from doctor. Patient cooperates with doctor, and BP is controlled. Patient told, “It’s okay now.” Patient receives no re-education about the lifelong need for treatment. Patient doesn’t want to think of himself as “sick.” Patient believes doctor meant “Stop taking the medicine” when he said, “You’re under control.” Belief that he’s “cured” and “told to stop medicine” is reinforced. Patient stops medicine and visits. Drops out Patient believes – His diagnosis – In medicine and its efficacy to lower blood pressure – In the need for lifelong treatment – In the hazard of HBP if left uncontrolled Patient believes medicine is needed only to lower blood pressure, not to keep it low. Patient has no symptoms to tell him that blood pressure is uncontrolled. Patient believes hypertension is “nervous tension.” Patient believes he can tell when BP is high since he knows when he is tense. Medical system does not follow up to recall patient for appointments. Patient believes he can control HBP with “selfdiscipline” or by “accepting life.” Patient takes medicine when he feels tense and believes this adequately lowers BP. Patient feels no need to see doctor and keep appointments because he knows when to take medicine. Patient believes he’s adequately controlled—reinforced by lack of professional intervention. Remains Uncontrolled Drops out • Public health approaches, (e.g. reducing calories, saturated fat, and salt in processed foods) can achieve a downward shift in a population’s BP. • Reducing overall BP by only a few mm Hg could affect overall CVD morbidity and mortality by as much or more than treatment alone. • Public Health approaches provide an attractive opportunity to interrupt and prevent the costly cycle of managing hypertension and its complications.