15(iii)_CoG_Gov May 2013 - Oxford Health NHS Foundation Trust
advertisement
_CoG_Gov May 2013 - Oxford Health NHS Foundation Trust")
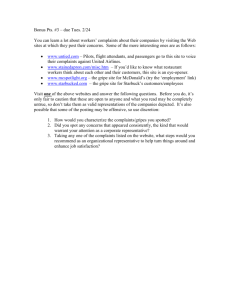
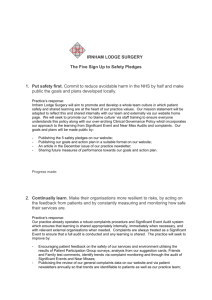
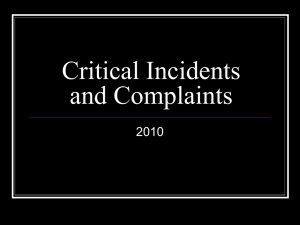
MEMBERS COUNCIL QUALITY REPORT (May 2013) Safety There have been 2613 incidents reported in quarter four and 9881 for the whole year, a mean of 2470 per quarter compared to a mean of 1825 per quarter last year. The number of incidents per quarter was; Q1 2012/13 2226 Q2 2012/13 2529 Q3 2012/13 2513 Q4 2012/13 2613 The number of incidents graded as orange and red by staff remains stable and the steady increase in green and yellow rated incidents has leveled off due to the large number of ungraded incidents awaiting sign off by managers currently being dealt with through line management. In 2009, we set a target of increasing the number of less serious (green and yellow) incidents we reported by 50% by March of 2012. It is expected that a Trust with a good safety culture will report high levels of low level incidents and work to learn from incidents and reduce the number of serious incidents. We have now met the target we set ourselves in 2009 as can be seen from the chart below. Year 2009/2010 2010/2011 2011/2012 2012/2013 Target (increase of 50% on 2009 figure) Total (Mental Health and CHO combined) 5981 6230 7302 9069 8972 1 The chart below shows reporting numbers for the main categories of incident over the last 15 months. The types of incident broadly show random variation over the months. *Falls include all fall incident patient and staff The level of reported violence has been maintained. Wards in the mental health division remain the highest reporters. Changes in the number of incidents on a particular ward are usually due to the presence of individual patients who account for a large number of incidents. A report on the use of physical restraint and seclusion accompanies this report to the IGC. This details where incidents of violence and aggression are occurring, their nature and severity. The notable increase this quarter is in reported incidents of self harm which has increased each month since December. The areas with the largest increase have been Portland and Ashurst wards, as shown in the chart below. The increase in Ashurst was mainly accounted for by one patient who self harmed 38 times, which is 84% of the Ashurst’s self harm incidents in total for Q4. The increase on Portland Ward was due to incidents from 13 patients, four of whom had 5 or more self harm incidents in March alone. The chart below shows the most common outcome from a SIRI this quarter is an RCA investigation. There have been a substantial number of RCA’s and record reviews requested this quarter. The total number of investigations was 34 comprising 19 RCAs, 10 record reviews, 2 IIRs and 1 Independent Management Review requested. In 2 cases a decision on the level of investigation has still to be taken (table below). In addition, 2 RCAs and 1 record review have been requested for the 3 orange incidents noted above. Type of Investigation 40 30 Total SIRIs 20 RCA 10 Record Review 0 None/Other Q1 12/13 Q2 12/13 Q3 12/13 Q4 2 Overall there were more SIRIs this year than in previous years. This is likely due to a wider range of incidents being designated as SIRIs to be investigated. Of 9 completed SIRI RCA Investigations that went to panel in Q4, 7 sought to involve family, carers or patients. On 2 occasions families both participated and wished to receive feedback. On 3 occasions families wanted to be given feedback but did not wish to participate in the investigation. There was only 1 case where the family neither wanted to be involved or receive feedback. In addition to the RCA investigations that are carried out, it is also expected that patients and relatives are advised of record reviews and invited both to participate and receive feedback. The Eighth Learning from Incidents Newsletter was published in February 2013. In addition to the regular content around incidents and patterns of SIRIs there was a highlighted piece on the Francis report and the role that the SIRI process can play in ensuring an open scrutiny of practice and learning to reduce harm. The last two learning events in Oxon and Bucks took place in February 2013. Attendance was much improved in response to better advertising and support from Divisions. The sessions continue to be very positively received by those who attend. The next Learning events will be held in June 2013. Patient Experience Friends and Family test pilot In the Febraury Members quality report Govenors were informed about the requirement to implement the F&F test in the Community Hospitals and Minor Injuries Units (MIU) from April 2013. During quarter 4 we undertook a pilot testing 4 methods of surveying to see which may be the most productive. The Community Hospitals and Abingdon and Witney MIUs patients were given on discharge or departure a postcard with the test question and four follow up questions which could be returned via freepost or completed on site and placed in a comments box. The postcard also contains information about how the patient could either complete the survey online or phone a free phone number and have the questions asked of them. Henley MIU had an electronic kiosk in the area outside the treatment room where a patient could complete it on site but with privacy. The pilot was run from 14th Jan to 20th March 2013 there were 198 responses in total from the following sources; on-line survey – 5 postcards – 157 kiosk – 36 telephone - 0 The Department of Health expects a response rate of 15%; the Trust during the pilot achieved a 4% response rate which poses a real challenge to prepare for the F&F test being a mandatory requirement by April 2014. In the meantime the Trust is expected to publish its net promoter score for Community Hospitals and MIUs and submit the score to the Local Area Team. 3 The net promoter score is calculated using the proportion of patients who would strongly recommend the service minus those who would not recommend it, or who are indifferent. Those respondents who answer the question as don’t know or blank are excluded from the calculation in line with national reporting guidance. During the pilot the Trusts NPS (net promoter score) was 65. % of respondents who said extremely likely to recommend (133 divide 191 x 100 = 69.63) % of respondents who would not recommend (neither likely or unlikely, unlikely and extremely unlikely) (9 divide 191 x 100 = 4.71) Minus Net promoter score = 65 (out of a possible 100) Complaints and PALS The number of complaints received during 2012 – 2013 by quarter is; Quarter 1 (April-June 2012): 42 Quarter 2 (July-September 2012): 68 Quarter 3 (October-December 2012): 87 Quarter 4 (January-March 2013): 81. The graph below shows the number received by month, the average number received for the two year period is 20 per month, and this increases to 23 per month if the average is taken just for the last year in 2012/13. There is an upward trend in the number of complaints which have been received and this trend is also reflected in the number of calls made to the Complaints & PALS Service free phone number to discuss informal concerns. Number of complaints received by month April 2011-March 2013 Excludes withdrawn formal complaints and re-opened complaints are not re-counted Includes MP forwarded patient concerns 40 35 Formal Complaints & MP Concerns 34 32 average for 2 years 30 29 28 26 Number 25 Linear (Formal Complaints & MP Concerns) 26 24 20 20 22 21 20 21 21 17 15 16 14 12 16 15 14 13 16 16 10 10 5 Mar-13 Jan-13 Feb-13 Dec-12 Oct-12 Nov-12 Sep-12 Jul-12 Aug-12 Jun-12 Apr-12 May-12 Mar-12 Jan-12 Feb-12 Dec-11 Oct-11 Nov-11 Sep-11 Jul-11 Aug-11 Jun-11 Apr-11 May-11 0 The majority of complaints which have been received are from or about the care and treatment of different patients/service users; out of the 278 complaints received 258 were from different 4 patients, and nine patients made two or three complaints (seven made two complaints and two made three complaints). In 2012/13, 24 concerns initially raised as a formal complaint have since been withdrawn by the complainant and resolution has been reached informally, there is no particular trend of which Division or team/ ward the concerns are being withdrawn from. The Parliamentary Health Service Ombudsman (PHSO) have reported that NHS Trusts are receiving an increasing number of complaints and that in 2011/12 there was a rise by 13% in complaints received from 2010/11. The Trust has seen these same increases with 154 complaints received in 2010/11, 203 in 2011/12 (24% increase on 2010/11) and a projected 261 in 2012/13 (which would be a 22% increase on 2011/12). However it is important to note the size of the Trust and number of services now provided has changed over the last three financial years. 94% of complaints have been acknowledged within the NHS Complaints Regulations (2009) of three working days and 82% of the 225 closed cases (184) have been responded to within an agreed timescale with the complainant. The majority of complaints received by the Trust contain a number of different concerns; however the complainant usually has a primary concern and reason for making a complaint. The most common categories for the primary concerns raised in the complaints (including open and closed complaints) received across the Trust in 2012/13 were (in order of high to low): 1. Poor/ inappropriate communication about decisions about care, explaining service provision and involving/ informing carers and relatives (41 complaints plus theme detailed as a secondary concern for a further 19 complaints) 2. Breach of confidentiality (15 complaints plus theme detailed as a secondary concern for a further 3 complaints) 3. Inpatient discharge either delayed, too quickly or lack of planning and arrangements (12 complaint plus theme detailed as a secondary concerns for a further 7 complaints) 4. Dissatisfied with process and outcome of continuing healthcare assessment (12 complaints plus theme detailed as a secondary concern for a further complaint) 5. Medication not received or delay, incorrect, side effects, method of administration and information (12 complaints plus theme detailed as a secondary concern for a further 14 complaints) 6. Lack of diagnosis or disagree with diagnosis (11 complaints plus theme detailed as a secondary concern for a further 1 complaint) The Complaints & PALS Department has an initiative scheme called “The PALS Exchange” where the team collects donations from a wide range of sources. The team seeks donations via announcements on the Trust’s Intranet and in the Insight magazine and requesting donations from local companies, Tesco’s in Aylesbury have been particularly supportive of the Trust in this respect. The items collected, books, DVD’s, CD’s, magazines, board games, puzzles and toiletries are given to wards for patients. Articles such as DVD are provided on an exchange/rotation basis to ensure variety on wards. PALS have been working closely with Helen Waddon, Community Champion from the large Tesco’s store in Aylesbury and together have run a number of themed events on the wards within Aylesbury. These have included an Olympic event, a pamper session, flower 5 arranging and most recently an Easter themed event. The team works with Helen to run a different themed event every month. The Complaints & PALS Department has also recently started to recruit volunteers to assist in running PALS surgeries across the Trust. There are currently three volunteers due to start participating in PALS surgeries from May. Each are experts by experience and it is anticipated that on occasions this may assist in patients feeling more confident ion giving feedback and suggestions for improvement. For further details on patient feedback including examples of accolades and compliments sent to clinicians from patients please see the Complaints Annual report presented to the Integrated Governance Committee during May and is available on request from Hannah Smith via the CEO Office. CQC Inspections – The Trust has had no announced or unannounced inspection visits this quarter. Clinical Effectiveness The key results for the following clinical audits completed in quarter four are: Audit Name Rating by Clinical Audit Committee Satisfactory Mental Capacity Act / DOLs audit in Oxon Community Hospitals Participation of adult mental health and addictions service Poor practitioners at Child Protection Case Conferences POMH-UK Topic 12a: Prescribing for people with a Personality Disorder POMH-UK Topic 2f: Monitoring metabolic side effects of patients on antipsychotics in Assertive Outreach and Forensic Units Quarterly audit of non-attendance in Wiltshire and B&NES Poor Poor Satisfactory Community and OSCA Services Quarterly audit of non-attendance in Swindon Community & OSCA Satisfactory Services Trust wide CPA audit for quarter 2 Satisfactory The Divisions are responsible for producing an action plan based on their results for each audit and the completion of the action plans are monitored by each Divisions local clinical governance group supported by the Quality and Audit Team. A summary of the results and associated improvement plans for the above audits was presented to the IGC in May 2013 and is available on request from the CEO office. Summary of completed audits during 2012/13 6 The initial 3 year Trust wide Clinical Audit plan for 2012-2015 proposed a total of 28 audits to be completed during the year 2012-13. During 2012-13 one national audit was removed from the national audit programme schedule for 2012/13 - POMH-UK Topic 4: Prescribing Anti-Dementia Drugs. An additional seven audits were added to the plan following publication of the Commissioning for Quality and Innovation (CQUIN) requirements and two Trust wide priority audits were added to the plan during the year (Medical Devices and Self assessment of how family friendly mental health in-patient wards are) making a total of 36 projects. Status of audit projects at end of March 2013 Completed and reported to IGC Draft report awaiting rating by CAC Data analysis Not completed Total Number of projects 25 7 3 1 36 The Carers Survey was the only project that was not started during 2012/13 as the action plan from the previous survey was still being completed. This survey is carried forward to the 2013-2014 plan. A number of performance targets were included as clinical audits in the 2012/13 plan; consequently they have not resulted in an action plan. The 2013/14 audit plan will only include audits that specifically measure an aspect of quality of care. Author: Caroline Birch (Deputy Director of Nursing) Lead: Ros Alstead (Director of Nursing and Clinical Standards) 7