A Cognitive Approach to Understanding Trauma, Dissociation and
advertisement

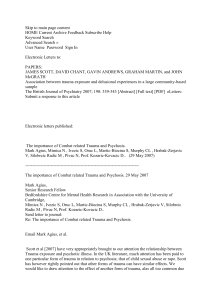
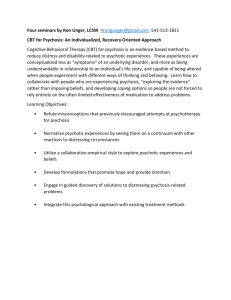
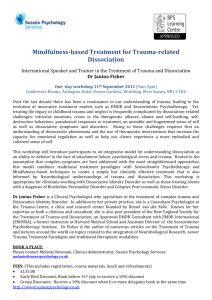
A Cognitive Approach to Understanding Trauma, Dissociation and Psychosis: research evidence and clinical implications Tony Morrison School of Psychological Sciences, University of Manchester & Psychosis Research Unit, GMWMHFT www.psychosisresearch.com Objectives • Understand the relationships between trauma, dissociation and psychosis utilising a cognitive model • Have an awareness of current evidence supporting this approach to understanding these links • Development of case formulations and outline of a treatment approach • Consider the implications of this approach for own clinical practice Read, J., van Os, J., Morrison, A. P., & Ross, C. A. (2005). Childhood trauma, psychosis and schizophrenia: a literature review and clinical implications. Acta Psychiatrica Scandinavica, 112, 330-350. Females: 36 studies from 1984-2001; total sample =2318 Males: 23 studies from 1987-2001; total sample =1234 80 Proportion experienced 69 70 61 60 50 53 49 50 40 36 Females 29 30 20 20 10 0 CSA Males CPA EITHER Type of abuse BOTH 1 Studies of Post-Psychotic PTSD Proportion meeting DSM-IV PTSD criteria 80 67 70 60 50 40 52 46 51 50 52 35 Initial 6m follow-up 30 20 10 0 McGorry Shaw et Priebe et Frame & Shaw et et al. al. (1997) al. (1998) Morrison al. (2002) (1991) N=45 N=105 (2001) N=42 N=36 N=60 Frame, L. & Morrison, A.P. (2001) Causes of PTSD in psychosis. Archives of General Psychiatry, 58, 305-306. Percent meeting DSM-IV caseness PTSD in Psychosis 80 70 67 60 50 50 40 30 20 10 0 Discharge (n=60) Follow-up (n=18) Frame, L. & Morrison, A.P. (2001) Causes of PTSD in Percentage of DTS variance psychosis. Archives of General Psychiatry, 58, 305-306. 60 52 50 40 30 20 13 6 10 0 PANSS: Psychotic symptoms Impact of events: psychosis Measure Impact of events: hospital Criteria for PTSD • 1. Individual exposed to a traumatic event and responded with intense fear/distress • 2. Persistently re-experience the event – – – – Intrusive recollections Recurrent dreams Reliving Intense distress at reminders Criteria for PTSD • 3. Avoid trauma linked thoughts feelings and conversations – Avoid activities, places ,people that trigger reminders – Fail to recall part of the trauma – Diminished interest – Feels detached from others – Unable to feel emotions normally appropriate to sits Criteria for PTSD • 4. Increased arousal – Sleep disturbance – Irritability/anger outbursts – Difficulty concentrating – Hypervigilance – Increased startle response Symptom Overlap Both disorders can be divided into positive and negative symptoms Shared PS. (Hall&del similar to intrusions, threat appraisals & flashbacks) Shared NS. (Numbing, responsiveness, concentration, derealisation, detachment, self-neglect & withdrawal) Paranoia & arousal, hypervigilence & sleep problems common to both Cognitive factors • Cultural unacceptability of appraisals and the cognitive and behavioural consequences of trauma may make people vulnerable to psychosis – Negative beliefs about self, world and others (such as ‘I am vulnerable’ and ‘Other people are dangerous’) have been shown to be associated with psychosis (Garety, Kuipers, Fowler, Freeman, & Bebbington, 2001; Morrison, 2001) – Such beliefs specifically formed as a result of trauma are related to psychotic experiences (Kilcommons & Morrison, 2005) – Positive beliefs about psychotic experiences (such as ‘Paranoia is a helpful survival strategy’) may also be related to traumatic experience, and have been shown to be associated with the development of psychosis (Morrison, Gumley, Schwannauer et al., 2005). Cognitive factors – Psychotic experiences are essentially normal phenomena that occur on a continuum in the general population (Johns & van Os, 2001). – It would seem that the occurrence of trauma in the life history of a person experiencing such phenomena may represent the difference between patients and non-patients (Honig et al., 1998). – It appears that catastrophic or negative appraisals of psychotic experiences result in the associated distress (Chadwick & Birchwood, 1994; Morrison, Nothard, Bowe, & Wells, 2004), and that such appraisals are more likely if people have a history of trauma Morrison, A.P., Beck, A.T., Glentworth, D., Dunn, H., Reid, G., Larkin, W. & Williams, S. (2002) Imagery and Psychotic Symptoms: A Preliminary Investigation. Behaviour Research and Therapy, 40, 1053-1062. • 74.3% (n = 26) were able to identify an image in relation to their psychotic symptoms. • For those patients who were able to identify idiosyncratic images experienced in conjunction with their hallucinations and delusions: – 69.2% (18 out of 26) reported that their images were recurrent – 96.2% (n=25) were able to link the image to the experience of a particular emotion and to a particular belief – 70.8% (n=17) were able to associate the image with a memory for a particular event in their past. Morrison, A.P., Beck, A.T., Glentworth, D., Dunn, H., Reid, G., Larkin, W. & Williams, S. (2002) Imagery and Psychotic Symptoms: A Preliminary Investigation. Behaviour Research and Therapy, 40, 1053-1062. • Feared catastrophes associated with delusions • • • • Being chopped up with axes Self being pushed into an oven Self being cut in two by man wielding large sword Being led away to prison by two large policemen • Memories of real traumatic life events • Self rocking in a psychiatric hospital • Being assaulted Morrison, A.P., Beck, A.T., Glentworth, D., Dunn, H., Reid, G., Larkin, W. & Williams, S. (2002) Imagery and Psychotic Symptoms: A Preliminary Investigation. Behaviour Research and Therapy, 40, 1053-1062. • Perceived source of psychotic experiences • • • • Neighbours in bedroom talking about me Spirits of friends and relatives surrounding head Man with beard shouting Image of black sphere of energy close to head • Content of the voices • Sexually abusing young girls • Picture of sharp instrument stabbing someone Cognitive Processes & PTSD Psychosis Selective attention to threat Thrasher, Dalgleish & Yule (1994) Bentall & Kaney (1989) Safety-seeking behaviours Ehlers & Clark (2000) Morrison (1998) Unhelpful thought control strategies (particularly punishment and worry) Reynolds & Wells (1999) Morrison & Wells (2000) Biases in autobiographical memory Brewin (1998) Baddeley et al. (1996) Imagery Sleep deprivation Arousal Dissociation Behavioural Role of dissociation in model • Dissociative experiences as trauma generated intrusions – Grounding strategies – Uncontrollable / dangerous? – Unusual (psychotic) appraisals? • Dissociation as a strategy – Pro’s and cons (and evidence for these) – Develop alternative strategies for safety Role of dissociation in model • Procedural beliefs about dissociation (positive and negative) – Evaluate accuracy and helpfulness – Development alternatives – Change bandwidth On the next slide carry out the following instructions Stare at the blue dots while you count slowly to 30. Then close your eyes and tilt your head back. A circle of light will slowly appear. Keep looking at it. What do you see? Common Components of CBT for PTSD & Psychosis • • • • Therapeutic relationship / safety Problem list and goal setting Normalising/education Individualised formulations (collaboratively produced) • Attribution, meanings & beliefs (re: trauma & symptoms) • Modification of safety-seeking behaviours • Modification of imagery Clinical Implications • Assessment and formulation-based intervention should incorporate potential developmental and maintaining factors such as: – Dissociation – Interpretation of intrusions (especially as external and/or madness) – Thought control strategies – Safety behaviours – Biases in memory and attention – Imagery – Procedural beliefs about vigilance, dissociation etc. Principles of Cognitive Therapy A cognitive model is required from which to empirically derive effective treatments: FORMULATE USING MODEL • What are you concerned about? SHARE A GOAL • You are not mad, your difficulties are understandable: NORMALISING MESSAGES AND LANGUAGE • How you appraise events contributes to distress: EVENT – HOW MAKE SENSE – HOW I FEEL – WHAT I DO • Either it is real or you believe it to be real: SIT ON A COLLABORATIVE FENCE • Test it out – drop your safety-seeking responses: EXPERIMENT IN & OUT OF SESSION Formulation • Normalise psychotic experiences, PTSD symptoms and emotions to reduce distress • Have a plausible understanding of the antecedents • basic/horizontal includes maintenance by dysfunctional responses • role of stress, life events and trauma in developmental formulation Unwanted, intrusive memories Voices and visions Physical flashbacks Interpretation of intrusions: Government agents are putting thoughts into my mind My body is being controlled There is a conspiracy to kidnap and harm me I am vulnerable Others can’t be trusted Dissociation and paranoia are useful Dissociation Hypervigilance Thought suppression Social withdrawal Restrict expression Fear Anger High arousal Physical / Sexual abuse Institutional care / prison Normalising information to decatastrophise experiences Administration of the Maastricht Interview Material drawn from “Think you are crazy think again” Presentation and discussion of the “Spot the voice hearer” game Presentation and discussion of Eleanor Longden’s TED talk Recovery stories Normalising information about relative prevalence of trauma and dissociation Conducting surveys Managing Dissociation • • • • • • • • • • • Normalise strategy and symptoms Identify triggers Consent for therapy; yellow and red cards Hold the pen and take the notes Consider current pros and cons vs. past Beliefs about controllability and experiments Physical grounding strategies Grounding objects Grounding phrases External focus of attention Current sensory cues to remain in present Recontextualising trauma • • • • • • Re-examination of meaning Role plays Imagery work Visit sites Responsibility pie charts Surveys Re-examine meaning of trauma • modifying the main problematic appraisals related to the trauma and it’s consequences – ‘I’m not normal and never will be’ = ‘I might have struggled with these experiences, but they are normal reactions to severe trauma and I am learning to cope with them’ – ‘I should have stuck up for myself’ = ‘no one could have fought-off adults’ – ‘I’m vulnerable’ = ‘ I’m no more vulnerable than anyone else; in fact, I’m a strong, resilient person who has been in the Navy’ ACTION: Assessing Cognitive Therapy Instead Of Neuroleptics (formerly North Of Britain Treatment Without Antipsychotics Trial) • Two site single blind RCT with two conditions (CT plus TAU vs. TAU) for people with psychosis not taking antipsychotic medication (due to refusal or discontinuation) • Assessments are 3 monthly following the initial baseline assessment (i.e. at baseline, 3, 6, and 9 months) • Follow-up assessments are at 12, 15 and 18 months • Recruitment target of n=80 – final n = 74 PANSS Total 80 ES = -0.46 70 60 Cognitive Therapy 50 TAU 40 30 0 3 6 9 12 15 18 >50% PANSS Change At 9 months • 7/22 CBT = 32% • 3/23 TAU = 13% At 18 months • 7/17 CBT = 41% • 3/17 TAU = 18% NB: 1 deterioration in CBT at 9 &18 months 2 deteriorations in TAU at 18 months For people with confirmed treatment-resistant schizophrenia that is unresponsive to an adequate trial of clozapine (or unable to tolerate such a trial), is CBT clinically and cost effective and acceptable? Demographics Variable Mean (SD/%) Age 43.04 (10.53) Male: Female ratio Duration of psychosis 273: 109 235.17 (124.50) Attrition at 9 months • CBT plus TAU – 100 completed – 4 withdrawals – 2 lost to follow-up • TAU – 105 completed – 5 withdrawals – 1 lost to follow-up Case study • 1-8 – Problems and goals (confidence, self-esteem, low mood and self-harm, voices, low motivation) – Formulation – Continuum for low self-esteem – Evidential analysis of self-critical thoughts – Positive imagery – Survey / results (judged, relationship, employ) Experiences that worry me Social situations Voices What I make of it I am not good enough I must harm myself Voices are bullies Others will harm me What I do Try to stay in control of thoughts Isolate self and withdraw Negative comparisons Rituals Daydreaming / dissociation What I make of the self / world I am different I am unimportant and worthless Need to be alert for danger Other people cannot be trusted Others will leave and reject me Early experiences Family criticism Never fit in Severe bullying at school and work Wrongful arrest and harassment How I feel Low mood Hopeless Anxiety Anger Case study • 9-11 – Revisit goals – Negative comparisons – I’m a failure – Activity for mood • 12-15 – Daydreaming and dissociation (normalising; pros/cons; diary; modified GAD model) – Voices Case study • 16-18 – PTSD (grounding, attentional focus, reconsider meaning) • 19-22 – Social anxiety (stop post-mortems, anticipation > event, stop safety behaviours, external focus, update image) trigger Social situations Negative thought Others will judge me Others will reject me Image of self Weak Vulnerable Hunched Ugly Very skinny Unconfident Shaky What I do Arrive late Avoid eye contact Only speak to people I know Speak with hand over mouth Doodle/fidget Hunch up and try to disappear How I feel Anxiety Tense Palpitations Sweaty Shaky Case study • Progress: – I am good enough 0% 80% – Social confidence 10% 70% – I am different 100% 50% (neutral) – I’m as important as others 0% 80% – No flashbacks, no self-harm, no suicidal thoughts – Voices only at night and managable – Getting married – Doing postgraduate course Implications for Mental Health Services • Collaborative, hope inspiring relationships with service users • Minimise the harm professionals can cause • Choice of treatments • Provision of normalising, recovery-orientated information • Involvement of service users in planning, delivery & development of services • Measurement of recovery instead of symptoms as primary outcome Phases of therapy 1)Assessment and enagement phase (approx sessions 1-4) 2)Introduction of strategies targeting dissociative phenomena/processes (approx sessions 5-14) 3)Longitudinal Formulation/Cognitive Behavioural Change strategies phase (approx sessions 14-22) 4)Consolidation phase (final 2 sessions) Dissociative focus • Emphasises training and practice of skills to manage dissociative responses and increase perceived controllability of dissociation: Distress tolerance skills and low arousal strategies Refocusing; Use of grounding objects, images, statements and words Other emotional regulation, arousal management strategies, sleep hygiene Attention Training Technique (ATT: Wells, 2009) Trauma and psychosis focus Trauma-related work (e.g. exposure, imagery work, cognitive restructuring informed by CT for PTSD) Additional work targeting maladaptive appraisal of dissociation using CT strategies or techniques adapted from meta-cognitive approaches (e.g. controlled dissociation period) Cognitive and/or behavioural change strategies targeting core appraisals of voices/visions leading to related distress (e.g. beliefs about the power of voices; controllability of voices/voices as a sign of losing control) Consolidate understanding of a developmental / longitudinal formulation of difficulties, which links them (many becomes one problem) Conclusions • • • • Trauma-induced psychosis exists Psychosis can cause PTSD Assess trauma history and PTSD Incorporate trauma and trauma-related processes in the formulation • Intervention strategies derived from PTSD work can be useful (guided by formulation) • Minimise harm / additional trauma from services Objectives revisited • Understand the relationships between trauma, dissociation and psychosis utilising a cognitive model • Have an awareness of current evidence supporting this approach to understanding these links • Development of case formulations and outline of a treatment approach • Consider the implications of this approach for own clinical practice