eEdE-165
advertisement

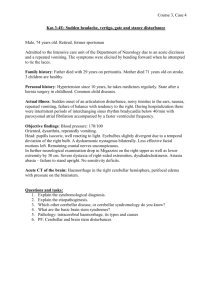
Department of Diagnostic and Interventional Imaging Department of Pediatrics Control #: 326 Cerebellar Infections in Children. Clinical and Imaging Vignettes eEdE#: eEdE-165 Eliana Bonfante M.D. Rajan Patel M.D. Gloria Heresi M.D. Roy Riascos M.D. No Disclosure Purpose • To describe the clinical presentation and diagnostic algorithm for infections of the posterior fossa in children. • To illustrate the imaging findings of frequent and infrequent infectious diseases that affect preferentially the posterior fossa structures. Approach Using a case based format we review the clinical presentation, diagnostic workup and imaging findings of multiple infectious processes that present predominantly in the posterior fossa in children. Discussion Cerebellar Infections in Children. Clinical and Imaging Vignettes Introduction • Different infectious agents result in a preferential involvement of the cerebellum in pediatric patients. • The clinical presentation, workup, and imaging findings of posterior fossa infections in children will be discussed in a case based format. Infections of the posterior fossa in children Clinical presentation • Ataxia • Fever • Nausea and vomiting Workup • CBC • CSF analysis • Urine and serum drug screen Imaging findings • CT • MRI Clinical presentation • Ataxia (Greek: ataktos, lacking order) refers to a pathologic abnormality of organization or modulation of movement. • Causes of cerebellar ataxia in children: – Infectious/immune-mediated cerebellar disorders (acute cerebellar ataxia, acute demyelinating encephalomyelitis, systemic infections) – Toxic: alcohol and drug related – Mass lesions : tumor, vascular lesions, abscesses , – Hydrocephalus – Trauma – Stroke – Paraneoplastic disorders (Opsoclonus-myoclonus syndrome) – Sensory ataxia (Guillain-Barré syndrome Miller Fisher syndrome) – Paretic ataxia – Inborn errors of metabolism Clinical presentation Acute Cerebellar Ataxia AKA Acute cerebellitis • The most common cause of childhood ataxia (40% of all cases) • Postinfectious cerebellar demyelination > direct infection of the cerebellum. • Postinfectious cerebellar demyelination is thought to be an autoimmune phenomenon incited by infection or immunization, with subsequent cross-reaction of antibodies against cerebellar epitopes, although specific autoantibodies have only rarely been identified. Workup Reported Causes of Infectious/Postinfectious Cerebellitis in Childhood Systemic infection Direct Infection • • • • • • • Echovirus type 9 Varicella zoster Coxsackie B Bacterial meningitis (pneumococcal, meningococcal) Coccidiomycosis Histoplasmosis Toxoplasmosis Post- or Parainfectious Cerebellitis • • • • • • • • • Varicella zoster Epstein-Barr virus Mumps Legionella pneumophilia Hepatitis A Influenza A and B Herpes simplex virus I Coxsackie A • • • • • • • • Echovirus type 6 Enterovirus type 71 Malaria Poliovirus type 1 Japanese B encephalitis Parvovirus B19 Measles Mycoplasma pneumoniae • • • • Typhoid fever Scarlet fever Mycoplasma pneumoniae Diphtheria Leptospirosis Workup • Routine CSF analysis includes – – – – – Cellularity (total WBC and red blood cell [RBC] counts) Absolute neutrophil count Chemistry (glucose and total protein concentrations Gram-stained smear of the sediment Bacterial culture. • Ancillary CSF microbiologic testing: – Culture for viruses, mycobacteria, fungi – Polymerase chain reaction (PCR): ideally suited for identifying fastidious organisms that may be difficult or nearly impossible to culture such as enteroviruses, herpes simplex virus (HSV), Epstein-Barr virus, Borrelia burgdorferi, and has been especially useful in the diagnosis of DNA and RNA viral meningitis. Workup CSF feature Significance Lymphocytosis Supports presence of inflammatory process Pleocytosis, elevation of CSF protein Suggest meningitis or encephalitis Glucose Decreased in bacterial meningitis Protein Elevated in meningitis and in 26-50 % of postinfectious cerebellar ataxia Cytoalbuminologic dissociation Guillain Barre, Miller Fisher Oligoclonal bands, elevation of serum to CSF immunoglobulin index and myelin basic protein Acute cerebellar ataxia, acute postinfectious demyelinating encephalopathy, and multiple sclerosis Imaging workup • Neuroimaging is often obtained in the emergency room to exclude a mass lesion. In the absence of altered consciousness, focal neurologic signs, or marked asymmetry of ataxia, the yield of such scans is low. • Computed tomography (CT) and magnetic resonance imaging (MRI) of the brain are normal in most children with postinfectious ataxia. Case 1 Clinical presentation 2 year old female presented with acute respiratory failure that required CPR and intubation. Workup • CBC leukocytosis • Negative blood and urine viral cultures • CSF not suggestive of meningitis (Glucose 67, Protein 94, RBC 6950, WBC 22, 77% Segs, 14% Lymphs.) • Tracheal aspirate positive for Group A Streptococcus and adenovirus. Imaging findings • Chest x-ray showed bibasilar atelectasis • Brain CT showed edema in the cerebellar hemispheres Case 1 - Imaging findings Brain CT shows edema in both cerebellar hemispheres. MRI demonstrates cytotoxic edema and hemorrhage in both cerebellar hemispheres. There is also gyriform contrast enhancement. Case 1- Analysis • The patient developed acute hydrocephalus that required occipital decompressive craniectomy and shunt placement. • Empiric broad spectrum antibiotics were started. • Workup yielded positive tracheal cultures for adenovirus and Group A Streptococcus. • Group A Streptococcus was deemed to be the most likely causative agent. Case 2 Clinical presentation • 8 year old female with history of absence seizures who presented with fever, nausea and vomiting followed by rapid mental status decline Workup • CSF and blood cultures were unrevealing. • Stool culture for Shigella Sonnei was positive Imaging findings • Brain CT and MRI showed edematous changes in the right cerebral hemisphere and left cerebellum. Case 2 – Imaging findings Brain MRI shows cytotoxic edema in the right cerebral and left cerebellar hemisphere. A decompressive hemicraniectomy on the right was performed. Case 2 - Analysis • The patient required decompressive hemicraniectomy due to severe right hemispheric swelling. • A positive stool culture for Shigella sonnei made Ekiri syndrome the most likely diagnosis. • Shigella infection is known to be associated with seizures, encephalopathy with lethargy, confusion, and headache. • Ekiri Syndrome is a particularly lethal and rare syndrome associated with Shigella characterized by the rapid development of seizures, cerebral edema and coma in patients with high fever and few dysenteric symptoms. Case 3 Clinical presentation • 9 year old African American male presenting with jaundice, abdominal pain, and lethargy. • The patient had a history of travel to Tanzania in Eastern Africa two months prior to admission. Workup • Blood smear positive for Malaria Imaging findings • Brain CT demonstrated bilateral cerebellar edema. • Brain MRI showed edema and hemorrhage in both cerebellar hemispheres. Case 3 - Imaging findings Brain MRI shows cytotoxic edema in both cerebellar hemispheres, with small foci of hemorrhage. Case 3 - Analysis • CNS malaria is a life-threatening complication seen in 2% of malaria cases, particularly in Plasmodium falciparum infection. • Cerebral damage in malaria is due to vascular sequestration of parasitised erythrocytes and the potential cerebral toxicity by cytokines. • Reported MRI findings include focal or diffuse signal changes in centrum semiovale, corpus-callosum, thalamus, and insular cortex. Central pontine myelinolysis, myelinolysis in the upper medulla, cerebellar syndrome with demyelination, and micro infarcts of the cerebellar hemispheres have also been reported. Case 4 Clinical presentation Workup • 13 year old female presents with 1 day history of severe frontal headache. • CSF with elevated protein, leukocytosis, and lymphocytic predominance, but high eosinophil count. • She also has photophobia. • 2 weeks ago, patient had watery, non-bloody diarrhea for 3 days, and bloody emesis. Imaging findings • MRI demonstrated cerebellar swelling and enhancement Case 4 – Imaging findings Brain MRI shows cytotoxic edema in the superior cerebellum bilaterally, with patchy linear contrast enhancement. Case 4 - Analysis • CSF with elevated protein, leukocytosis, and lymphocytic predominance, but high eosinophil count. • The workup for infections including HIV, HSV, West Nile virus, adenovirus, parainfluenza, and influenza was negative. • Mycoplasma EBV and CMV serologies showed old infections. • Patient had a full recovery. • Final diagnosis: Acute cerebellitis with unknown etiology. Case 5 Clinical presentation Workup • • 10 yo male presenting with headaches, neck pain, photophobia, and right sided weakness. CSF analysis demonstrated xanthrochromia, elevated WBC and RBC, as well as eosinophilia on the cell differential. • CSF and serum were negative for Histoplasma antigen and Coccidioides. • Serum Mycoplasma IgG and IgM were positive. Imaging findings • Brain CT shows edema in the right cerebellar cortex. • Brain MRI shows severe edema in the right cerebellum, with gyriform contrast enhancement. Case 5 – Imaging findings Brain CT shows edema in the right cerebellar cortex. Brain MRI shows severe edema in the right cerebellum, with gyriform contrast enhancement. Case 5 - Analysis • In the acute phase the patient required ventriculostomy to manage acute hydrocephalus. • The discharge diagnosis was culture negative eosinophilic meningitis. • Empiric antimicrobial treatment for bacteria, fungi, and parasites was given. • There was clinical improvement with residual right sided weakness. Case 6 Clinical Presentation • 16 year old female presented with 3 days history of fever and progressive headache Imaging findings Workup • Seropositive for HIV • Serum antitoxoplasma IgG antibody level 160 mg/dl • CD4+ count 78 cells/mm • CT Head: Hypodensity in the both cerebellar hemispheres (Right>Left) • MRI Brain: Multiple target appearing enhancing lesions in both cerebellar hemispheres with T2 hypointense rim, characteristic for Toxoplasmosis Case 6 –Imaging findings CT Head: Hypodensity in the both cerebellar hemispheres (Right>Left) with minimal mass effect over the 4th ventricle. MRI Brain: Multiple target appearing enhancing lesions with T2 hypointense rim in both cerebellar hemispheres, findings are characteristic for Toxoplasmosis Case 6 - Analysis • With characteristic imaging findings and laboratory analysis, diagnosis of Toxoplasmosis was confirmed. • The patient received a 200-mg loading dose of pyrimethamine and was placed on a regimen containing pyrimethamine (75 mg/day), sulfadiazine (1500 mg 4 times daily), and leucovorin (10 mg/day). • On day 3 of treatment, the patient’s symptoms began to improve. • After 6 days, she was completely asymptomatic and was discharged. • Treatment was continued for 6 weeks, and the patient was subsequently prescribed pyrimethamine 50 mg/day, sulfadiazine 2 g/day, and leucovorin 10 mg/day orally for secondary prophylaxis against Toxoplasma. • Repeat MRI of the brain with contrast 1 month after the diagnosis showed complete resolution of the lesions in both cerebellar hemispheres. Case 6 - Analysis • In immunocompromised individuals (e.g. AIDS patients), toxoplasmosis is the most common cause of a brain abscess. • Pathologically, parenchymal toxoplasma lesions have three distinct zones: – a central avascular zone of coagulative necrosis – an intermediate vascular zone containing numerous organisms – an outermost zone of encysted organisms: Toxoplasma lesions do not have capsule • On post-contrast imaging, Toxoplasmosis demonstrates “ring” enhancement. With delayed or double dose contrast study, it shows central filling of contrast which will give rise to “target” appearance as seen in our case. Conclusions • Numerous viral, bacterial, fungal, and parasitic infectious agents can present with preferential or exclusive involvement of the cerebellum in pediatric patients. • CSF analysis, cultures and other ancillary test are useful to identify specific causative agents. • Imaging findings tend to be similar amongst different pathogens but are helpful for the management of the acute neurologic conditions. • An infectious agent is not always isolated. • Wide spectrum antimicrobial coverage, supportive treatment, and if needed management of hydrocephalus are pivotal in the acute phase. References • • • • • • • Y. De Bruecker et al., “MRI Findings in Acute Cerebellitis,” European Radiology 14, no. 8 (August 2004): 1478–83, doi:10.1007/s00330-004-2247-y. Babak Pourakbari et al., “Lethal Toxic Encephalopathy due to Childhood Shigellosis or Ekiri Syndrome,” Journal of Microbiology, Immunology, and Infection = Wei Mian Yu Gan Ran Za Zhi 45, no. 2 (April 2012): 147–50, doi:10.1016/j.jmii.2011.09.005. Hiromasa Uchizono et al., “Acute Cerebellitis Following Hemolytic Streptococcal Infection,” Pediatric Neurology 49, no. 6 (December 2013): 497–500, doi:10.1016/j.pediatrneurol.2013.06.003. J. Saavedra-Lozano et al., “Isolated Cerebellar Edema and Obstructive Hydrocephalus in a Child with Cerebral Malaria,” The Pediatric Infectious Disease Journal 20, no. 9 (September 2001): 908–11. B. K. Paunipagar D D Rasalkar, “Magnetic Resonance Imaging in Cerebral Malaria: A Report of Four Cases,” The British Journal of Radiology 84, no. 1000 (2011): 380–85, doi:10.1259/bjr/85759874. Ryan and Engle, “Acute Ataxia in Childhood.” Journal of Child Neurology 18,no.5(May2003):309-16. Maria Ciardi et al., “Acute Cerebellitis Caused by Herpes Simplex Virus Type 1,” Clinical Infectious Diseases 36, no. 3 (February 1, 2003): e50–54, doi:10.1086/345781. The University of Texas Health Science Center at Houston Department of Diagnostic and Interventional Imaging Department of Pediatrics CONTACT US Eliana.E.Bonfante.Mejia@uth.tmc.edu Rajan.P.Patel@uth.tmc.edu Gloria.P.Heresi@uth.tmc.edu Roy.F.Riascos@uth.tmc.edu