swede heart scaar
advertisement

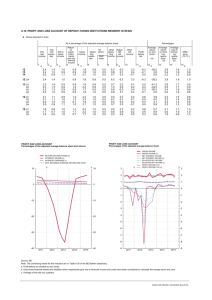
Transforming Health Care Delivery through CV Registries The Swedeheart registry Stefan James, MD, PhD Director of Interventional Cardiology Associate Professor of Cardiology Uppsala Clinical Research Centre University Hospital Uppsala, Sweden Quality registry previously RIKS-HIA SCAAR Hjärtkir SEPHIA Journal Ålder, kön, etc. x x x x x Tid. sjukdomar x x x x Tid. mediciner x x x x Status x x x x Labvärden x x x x LVEF x Komplikationer x x x x x Långtidsuppföljn x x x x x x x Prevention, QoL x x Ulf Stenestrand, 2008 Quality registry today Swedeheart RIKS-HIA SCAAR Hjärtkir Ålder, kön, etc. x x x Tid. sjukdomar x Tid. mediciner Journal SEPHIA TAVI x x x x x x x x x x x x Status x x x x x Labvärden x x x x x LVEF x x x Komplikationer x x x x x x Långtidsuppföljn x x x x x x x x x Prevention, QoL x Modifierad efter Ulf Stenestrand, 2008 Quality registry tomorrow Journal Swedeheart RIKS-HIA SCAAR Hjärtkir Ålder, kön, etc. x x x Tid. sjukdomar x Tid. mediciner SEPHIA TAVI x x x x x x x x x x x x Status x x x x x Labvärden x x x x x LVEF x x x Komplikationer x x x x x x Långtidsuppföljn x x x x x x x x x Prevention, QoL x Modifierad efter Ulf Stenestrand, 2008 SCAAR SWEDE HEART Hospitals No Patients Annual No Thoracic surgery 100 % 8 100 % 7000 SCAAR (coronary angiography and PCI) 100 % 30 100 % 40000 RIKS-HIA coronary intensive care registry 100 % 73 60% 50000 SEPHIA Secondary Prevention After Myocardial Infarction(<75 yrs) 85% 65 55% 5500 TAVI 100 % 7 100 % 150 Correct data Stimulate use of data Samma information används både i register och journal ökar tillförlitligheten Färre inmatningar - säkrare / reducerar dubbelarbete Används data aktivt ökar validiteten Följa egna patienters resultat / komplikationer Intressanta interaktiva on-line rapporter Modul för läkare under utbildning Automatisk rapport till strålfysik SCAAR Data entry on line by the operator SWEDE HEART 190 variables: Patients characteristics Procedural details (lesions, stents, devices etc.) History is presented and all previously implanted stents have to be checked Pharmacological treatment Complications Interactive immediately available information SCAAR SWEDE HEART Information om tidigare ingrepp Rätt åtgärd kan vidtas Dålig teknik, medicin, medicinteknisk utrustning eller sjukvårdsartiklar kan identifieras Patients enrolled 2003-2004 and followed max 3 years N=19 771 0.08 0.06 0.04 Future potential increased mortality? 0.02 RR: 1.03 (0.84,1.26) RR: 1.32 (1.11,1.57) RR 1.3 (1.1-1.6) 0.00 Cumulative risk of death 0.10 ?? 0.0 0.5 1.0 1.5 2.0 2.5 3.0 9298 3434 5966 1777 3199 626 5y Time (years) BMS 12880 DES 5770 12473 5605 12354 5541 12228 5471 N Engl J Med 2007;356:1009-19. The SCAAR Scare “The SCAAR registry is contaminated with fraud data….” M Leon 2007 “This clearly shows how inappropriate registry studies are….” Kastrati 2007 “What is rotten in the kingdom of Sweden” P. Serruys 2008 BMS vs DMS Bare metal stents vs. Death metal stents Patients enrolled 2003-2006 and followed max 5 years 0.10 BMS DES 0.05 RR: 0.82 (0.73, 0.92) 0.00 Cumulative risk of death 0.15 N= 47.867 RR: 1.06 (0.97, 1.17) 0 1 2 3 Time (years) 4 5 James, N Engl J Med 2009;360(19):1933-45 Stent thrombosis SCAAR SWEDE Slope 0.5% per year 2 Cumulative rate of definite stent thrombosis (%) SCAAR N=64 979 stents 1.5 DES, N=26 330 Unadjusted 1 BMS, N=38 649 0.5% early 0.5 0 0 1 2 Years after PCI Lagerqvist, Circ Cardvasc Int 2009 Oc;2(5):401-8 HEART SCAAR 0,12 Stents used <1000 times excluded Adjusted 0,11 Braun Coroflex Blue, N=3,761 Hexacath Titan2, 0,10 N=1,974 Abbott Flexmaster Fl, N=1,311 0,09 Medtronic Driver, N=15,954 Sorin Chrono, N=2,465 BS Liberté, N=28,735 Abbott Vision, N=8,565 Other, N=3,654 0,08 0,07 3.0% Cumulative risk of Restenosis 0,06 0,05 Medtronic Endeavor, N=4,891 1.4% 0,04 BS Taxus Express, N=3,165 Cordis Cypher, N=11,513 BS Taxus Liberté, N=16,357 XienceV / Promus, N=1,849 0,03 2.3% 0,02 0,01 N=104,142 stents 0,00 November 8th 2009. Copyright SCAAR. 0 1 2 Time (Years after stenting) 3 4 5 James, Eurointervention 2009 Stent thrombosis Cumulative risk of acute stent thrombosis SCAAR Number of stents (events) Adjusted for baseline differences in clinical, lesion and vessel characteristics Braun Coroflex Blue 3868 (93) Hexacath Titan2 2225 (50) BS Taxus Express 3148 (78) 0,02 Cordis Cypher 12240 (264) Medtronic Driver 19767 (265) BS Liberté 32630 (377) BS Taxus Liberté 17705 (269) Abbott Flexmaster Fl 1302 (18) Sorin Chrono 2594 (21) 0,01 Other 4591 (40) Abbot Vision 9756 (105) Medtronic Endeavor 5521 (55) Medtronic Resolute 1038 (7) Xience V – Promus 3417 (12) Abbott Xience Prime 1091 (3) 0,00 120,893 stents 0 1 2 3 4 Time (Years after stenting) 5 1,657 events Stent N < 400 excluded July 18th 2010. Copyright SCAAR. New generation DES n-DES vs o-DES: adjusted HR 0.62; 95% CI: 0.53-0.72 n-DES vs BMS: adjusted HR: 0.29; 95% CI: 0.25-0.33 o-DES vs BMS: adjusted HR: 0.46; 95% CI: 0.43-0.51 Adjusted BMS n-DES vs o-DES: adjusted HR: 0.50; 95% CI: 0.35-0.71 o-DES n-DES vs BMS: adjusted HR: 0.33; 95% CI: 0.23-0.47 n-DES o-DES vs BMS: adjusted HR: 0.65; 95% CI: 0.54-0.46 BMS o-DES n-DES Adjusted n-DES vs o-DES: adjusted HR: 0.77; 95% CI: 0.63-0.95 n-DES vs BMS: adjusted HR: 0.55; 95% CI: 0.46-0.67 o-DES vs BMS: adjusted HR: 0.72; 95% CI: 0.64-0.81 Adjusted BMS; N=42773 o-DES; N=12153 n-DES; N= 6425 Sarno et al ESC 2011 Over 20 high ranked publications annually 3.2% 3.0% 2.8% 2.6% 2.4% 2.2% 2.0% 1.8% 1.6% 1.4% 1.2% 1.0% 0.8% 0.6% 0.4% 0.2% 0.0% Surgery Bleeding Major Med discont’ Proportion Pseudoaneurysm Transfusion Hb-drop >20g/L Tretment more than compression Bleeding Minor Prolonged hosp Ultrasound/CT ´ Prolonged compression time Hematoma >5cm Any bleeding Complications in hospital Puncture site Femoral Radial Adjusted Cumulative Risk of death for up to 1 year: transfemoral vs. transradial access site Adjusted OR (95% CI) 0.78 (0.64-0.96) P= 0.018 Eur Heart J In press Radial procedures 2003-2011. Proportion Andel (%) 70 50 60 40 50 30 40 (%) 30 20 20 10 Figur 124. Andel punktioner i armen vid angio/PCI, 2003 - 2011. 2010 2009 2011 20102008 2009 2007 2008 2007 2006 2006 2005 2005 2004 2004 0 2003 0 2003 10 Registerbaserade case control studier TOPAS SCAAR/RIKS-HIA database screened for subjects surviving ST/MI occuring within 6 months of stenting and controls Subjects invited by local study sites (n=12) if ST/MI occured while subject on dual antiplatelet treatment All subjects on aspirin 75 -160 mg o.d. Subjects not already on clopidogrel were administered 600 mg clopidogrel 16-26 h prior to PD assessment ST Cases (n=48) VerifyNow P2Y12, VASP MI Cases (n=30) VerifyNow P2Y12, VASP Matched controls (n=50, n=28) VerifyNow P2Y12, VASP Internationella jämförelser Quality index Quality index and mortality Mortality post MI Andel mortaiity 30 day 30-dagarsmortalitet 30% 25% > 75 years 20% 15% 65-74 years 10% < 65 years 5% 0% 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 Kvinnor <65 år Män <65 år Kvinnor 65-74 år Män 65-74 år Figur 27g. Utvecklingen av 30-dagarsmortalitet vid hjärtinfarkt i relation till ålder och kön, alla åldrar, 1995-2006. Kvinnor >=75 år Män >=75 år Reasons for success Initiated by cardiologists, driven by National and local enthusiasts (champions) Highly motiverated users Immediate benefit in the local unit – on-line-reports, local variables, local development Open comparison of hospital performances All hospitals part of the same system Published studies in high ranked journal SCAAR TAPAS, total mortality at 1 year Vlaar, P.J. et al. NEJM 2008, 371: 1915 SWEDE HEART Proportion thombus aspiration in Sweden SCAAR SWEDE HEART TASTE trial flow chart SCAAR SWEDE HEART Thrombus Aspiration in ST-Elevation myocardial infarction in Scandinavia Patients with suspected STEMI referred to primary PCI N = 5000 STEMI diagnosis confirmed at coronary angiography. Informed consent obtained Online 1:1 randomization in SCAAR, guidewire advancement, i.c. nitroglycerin Thrombus aspiration and PCI PCI alone Immediately after PCI: TIMI flow grade 30 days: all-cause death 1, 2, 5 and 10 years: all-cause death and additional secondary endpoints Fröbert et al, AHJ 2009 Two questions need to be answered: Is the patient informed verbally and accepts participation? Are inclusion and no exclusion criteria met? TASTE SCAAR SWEDE HEART Thrombus Aspiration in ST-Elevation myocardial infarction in Scandinavia All primary PCI:s Randomized SCAAR Randomized Clinical Registry studies- RRCT SWEDE HEART New concept for clinical research Combines the advantages of a clinical registry and randomized study Ideal for studies with a simple hypothesis that can be evaluated with hard reliable endpoints Only clinically relevant questions can be addressed No substitute for RCT but a complement Development Treatment support Propose treatments and strategies according to guidelines Suggest discontinuation of therapies when risk for complications Automatic Syntax score calculation for stabil angina and more than 1 vd Calcualate CHADS-VASC score Warn about bleeding in ACS patients with high risk; high age, female sex, low body weight, reduced renal function PROM- Patient related outcome measures Acreditation Acreditation for users Web based course for handling regsitries for all new staff i required for access of user name and password Automatic annual control for all users 1 Stefan James Chairman SCAAR About Quality Registries Test Case Course Content Aim and goal About quality registries Final case Certification and Evaluation Communication News Events Science Questions The Swedish Health and Medical Service A system of national quality registries has been established in the Swedish health and medical services in the last decades. There are about 70 registries and four competence centres that receive central funding in Sweden. Definition of quality registers in Sweden A national quality registry contains individualised data concerning patient problems, medical interventions, and outcomes after treatment; within all healthcare production. It is annually monitored and approved for financial support by an Executive Committee. Vision The vision for the quality registries and the competence centres is to constitute an over-all knowledge system that is actively used on all levels for continuous learning, quality improvement and management of all healthcare services. 50 years old man with history of hypertension: -Chest pain 2 hours -St – elevations in inferior leads -Bp 160/100 mmHg -HR 48/min Ambulance Treatment: -ASA 320mg -Clopidogrel 600mg -Morphine 2 x 5mg -Oxygen Certification Aim and goal Background The quality certification process. The user have to pass a test in step two, to be able to get to step three. In step three the user have to pass the final case to get a certificate. Final Case and evaluation Aim and goal About Quality Registries Final Case Content: Content: Content: Content: Final Case for achieving certific ation. The case highlight important pieces of information in the Quality Register. -The certificate -Aim of Quality Registries -Purpose with certification process -National work with Quaity Registries -Atricels related to Cardiology -Common concepts -SCCAR Quality Registry -Multiple chocie -Test Case Certification and evaluation -Certifikation is recorded in a database -User can evaluate the course Monitoring Monitoring of a larger proportion of variables and patients Regional cross monitoring of hospital staff Monitoring symposia Automated checks Monitoring of non reported events Adjudication Important outcome variables adjudicated by competent staff Ex. Stent thrombosis, Restensis, bleeding, stroke 10% of reported event controlled PROM Patient Related Outcome Measures