Best Practice 1
advertisement

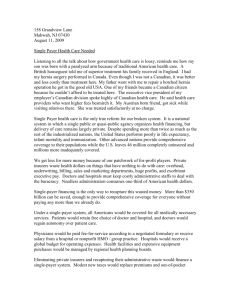
Contracts’ Language Review, ACO’s Capitated Agreements and 10 Best Practices o Session Sample4Title Slide Headline Here Up to Two Lines Long Presented by: Steve Selbst, Regina Vasquez, and Susan Charkin Presented to: John DoeSteve Selbst Name: President & CEO Title: CEO / Co-Owner Anybusiness Corporation Healthcents Inc. October 18, 2011 7/18/13 Learning Objectives • Finish contract negotiations process Language Review Monitor Claims and remember to renegotiate (Best Practice 10) • ACOs and Capitation • Bringing it all together with the 10 Best Practices, review of: • How to evaluate a managed care fee proposal • Preparing a SWOT analysis to identify opportunities and threats to a practice’s reimbursements • Conducting a managed care proposal reimbursement analysis used for benchmarking, pattern identification and business modeling Evaluate in-network vs. out-of-network options and maximize your billed charges to uniform, customary & reasonable (UCR) levels. • Techniques for negotiating “win- win” agreements with managed care companies • Simple technique for monitoring claims payments and comparing to your contracted rates to insure that you are not underpaid Most importantly, make more money from your commercial payer agreements! Your Contracts’ Assessment and proposal letters • Contact Susan Charkin at 831-455-2695 or charkin@healthcents.com If possible (Not required), bring… Revenue collected over a one year period for each payer Overall % Medicare you are currently contracted at by payer Any known issues with a payer, e.g., collections or other Any knowledge you have about your competition and the market that you are in Susan will discuss approaches to moving each of your agreements forward to higher reimbursement or other recommendations This ½ hour high value assessment is included as a part of your class. Also, remember to send a sample proposal letter to support@healthcents.com for feedback Operational Language Review, example Contract Language Template *Note: Healthcents staff are not attorneys and offer recommendations based on operational language that can impact reimbursement not legal advice Section Title Desired Language Sample Payer Clause Payment Policies Read manual / review Familiarize staff with Payer's payment policies; review with staff, sign up for PayerOnline: https://www.payerwebsite.com Protocols Read manual / review Familiarize staff with Payer protocols; review Payer's online information with your office staff: Payer's Affiliates Read manual / review Request a current list of Payer affiliates. Representations and Warranties of Practice Read manual / review Obtain Additional Manuals referred to regarding policies and protocols for certain Benefit Plans. Services not covered under a Benefit Plan Read manual / review Prior to delivery of services, obtain written waiver for services not covered under agreement. Cooperation with Protocols Make this more specific, don't box yourself in! Practice will provide notification for certain services, and respond to Payer for requests for clinical information; establish protocols for prompt turnaround time to provide requested clinical information. This list of services can vary by benefit plan, staff should verify benefits and eligibility prior to any procedure. Payment of Claims As short as possible, no more than 90 days from the date of service. Try to get this inserted vs. the language Payer may change its Payment Policies from time to time, but will make Payment offered here Policies available Time to File Claims Ideally 6 months or more Denial of Claims for Not Following Protocols, Not Timely Filing, or Lack of Medical Necessity 12 months is likely reasonable for appeals on denials Timely filing requirement is 90 days from date of service Claims may be denied for lack of timely filing or if Practice does not follow protocol; appeal period is 12 months after date of denial Member information is subject to change retroactively and payer may bill Retroactive correction of information As long as you are not a party to the payer collecting over individual/other responsible party for any services deemed overpayments due to regarding whether patient is a Customer payment to a patient, this should be okay. member ineligibility at time of service. More Operational Language Review Section Title Desired Language Sample Payer Clause Payment under this Agreement is payment in full This is okay but, make sure that your billed charges are set at UCR thresholds and review and verify patient benefit plans Practice will not seek payment in excess of the Payer's contractual rate, even if it is less than Practice's billed or customary charges. Correction of overpayments and underpayments of claims Be careful, here, since the 12 month period specifies that practice has 12 months to get payments that were made incorrectly. Make sure that the payer's time frame on retrospective reviews, as well, does not exceed 12 months. Also, remember "Best Practice 10", conduct a spot audit of your top codes, every month, to insure accurate payments. If either party determines claims were not paid correctly, the party may seek correction of payment but Practice must seek correction prior to 12 months after payment was made, overpayments may be offset from future payment. Term Can be either 1, 2 or 3 years depending upon your risk acceptance, tolerance and COLA offers for subsequent years from the payer The agreement proposes an Initial Term of 3 years, renewable automatically for one year terms Termination Benefit Plan Descriptions Contract Rate, "Lesser of…" Multiple Outpatient Procedures Practice-based Physician and Other Provider Charges Better to have 90 days without cause, also, be sure that there is language to address substantive changes to the contract, such as fee schedule changes, which allow you to terminate with as little as 30 day notice when such changes happen. Also require the payer to notify you, in writing, in advance of such changes. Make sure you know which payer products you are signing up for e.g., which PPO(s), HMO, Medicare Advantage etc. Remember to set your chargemaster above any contracted rate for all payers all key codes and set at UCR thresholds, likely 250%+ of Medicare in your locality. Consult with your CPA and tax advisor in this area to be sure write offs and other accounting concerns are balanced. Also, make sure the payer does not place limits on your ability to increase your billed charges, especially when contracted rates are not tied to billed charges. By either party with 180 day notice prior to the anniversary date of the agreement. Agreement contains a Medicare Advantage benefit plan (with corresponding payment appendix) and work comp benefit plan Reimbursement rates are lesser of eligible charges or aggregate applicable contract rate Multiple procedure contract rate is based on Payer's OPG methodology at Follow Medicare Guidelines of 100% of Primary and 100/50/50 (primary procedure plus up to two (2) additional procedures 50% for Subsequent. during the outpatient encounter) Make sure you complete credentialing prior to the beginning of the contract term or renewal term for all Assure all Practice based physicians are contracted or contractual physicians who practice under this agreement payment penalty provisions will be implemented And other operational language items to look for… • Use of non-par providers, e.g., ancillary services, anesthesia • Timely submission of claims (120 is reasonable, shoot for 365) • Timely claims payments (30-45 days from receipt of claims) • Claims Refunds: Ask that you be responsible for making payment vs. payment is withheld from future claims payments • Claims Changes: Ask that they payer request your permission, in writing before re-coding, re-ordering or modifying your claims • Bi-Lateral procedure reimbursement • Eliminate “favored nation” language • Changes to contract should trigger 30 day termination without cause, fee schedule changes should be categorized as material changes • Silent PPO’s, understand the payment relationships among your agreements, primary and secondary • Make sure there is agreement on reimbursement for other listed and unlisted services • Have your legal counsel review for possible legal concerns, we recommend always having a legal counsel review your contracts About Commercial Payer ACO’s • ACOs are networks of providers who are held accountable for the cost and quality of the full continuum of care delivered to a group of patients. – Part of the Affordable Care Act –Intended to reduce fragmentation and improve coordination among various providers, to result in lower health care use. • PCP is the “Point Guard / Quarterback”, generally may participate in only one ACO • Specialists may participate in many ACO’s •Fundamentally, 3 different Structures, next diagram… How are ACOs Structured? ACO Model 1 ACO Model 2 ACO Model 3 IPA or PCP Group Multispecialty Group Specialty Group Hospital Medical Staff Organization (MSO) or Physician-Hospital Organization (PHO) Hospital Hospital Devers & Berenson, 2009, RWJF and The Urban Institute, Timely Analysis of Immediate Health Policy Issues 8 Should a Urologist Participate in an ACO? Evaluate options available in your area, PPO, HMO , ACO, IPA • Compare reimbursement in the different payment models, ACO, PPO, HMO, other • Very Important: Evaluate bonus structures and reimbursement models (Value Based Contracting models) • Evaluate IT integration and patient data integration and tracking • Capitated vs. Fee for Service? • Go where your patients, employer groups and the money goes • Read our new article published by MGMA on the class web page! Capitation • Getting started • What is capitation-based payment • Methodology – Parameters for evaluation – Kinds of capitation agreements – Risks assessment How to leverage capitation agreement Getting Started Rules of Engagement: • Who is proposing capitation agreement (provider or carrier) • Know your practice statistics – – – – Volume of patients Fee-for-service carrier profile (Revolution Software) Demographics ICD-9 & CPT • Develop actuarial soundness (scope of services covered) • Request capitation agreement/proposal • Allow time to thoroughly review capitation proposal Developing your capitation rate For example, if a practice generates total payer 1 revenue of $1,000,000 and decided to assume cap shared risk of 4,000 assigned lives, you are collecting an average of $250 (i.e., 1M/$4K) per patient each year for payer 1. Cap payment payer 1 = $250/12 =$20.83pmpm (per member per month) Continue • For example, a Urologist who is hired at $550,000 per year with benefits included, decided to start accepting cap payments. The capitated agreement is one of 5 agreements that generate equal amounts of revenue. The practice wants to know what will be a good capitation rate… Divide $550,000 cost by 2,860 (industry standard for the average number of patients a typical urologist sees per year). • (550,000 / 2,860)/12=$16.02 then divide by 5 = $3.02 pmpm What Is Capitation-Based Payment? • Capitation-a payment method for health care services. • Capitation based payment is when the physician, hospital, or other health care provider is paid a contracted rate for each member assigned, referred to as "per-member-per-month" rate, regardless of the number or nature of services provided. • The contractual rates are usually adjusted for age, gender, illness, and regional differences. Mosby's Medical Dictionary, 8th edition. © 2009, Elsevier. Methodology • Parameters for evaluation – In order to evaluate a capitation based payment agreement, provider must evaluate what it cost to deliver care and what the carrier is willing to pay for services. – Establish a bench mark: the provider must examine the volume of patients, diagnosis (ICD-9), procedure or services to be provided (CPT), age and sex. – Do price or contract comparison (fee-for-service vs. capitation). If you do not have an internal tracking system in place, the Revolution Software. Healthcents can help you establish adequate contract rate comparisons. – Make sure that insurance is able to supply you with timely enrollment history. Confirm if payment is based on guarantee or assigned lives. – Check kinds of capitation payment agreement you are able negotiate. Kinds of Capitation Agreements • Per-member-per-month (PMPM) Payment - capitation payment based on number of patients assigned to the provider each month to manage patient care. • Partial Global Payment (PMPM) - capitation payment that does not only cover services provided by the provider, it includes outpatient services provided to enrollee. For example, laboratory and diagnostics services. • Global Payment (PMPM) - Capitation payment that includes the total risk for all items and services provided for patient assigned or enrollee selected. Includes facility services. Risks Assessment • Risk based payment - the provider is compensated on the ability to predict and manage future utilization for the population assigned (ability to manage risks). To leverage risks based payment provider should fully understand how risk is shared (upside vs. downside) • Upside Risk - if provider provides adequate care and save costs the provider should be able to benefit and share savings. • Downside Risk - is there a clause in the agreement that penalizes provider for over utilization? • Manage risk by obtaining stop-loss insurance. How to Leverage a Capitated Agreement? • Carve out high dollar services • New technology usually referred to experimental services should be included in agreement and paid at fee-for-service rate (billed with report). • Negotiate adequate number of enrollees. Capitation payment should be based on date of enrollment and not date of assignment. • Establish division of financial responsibility (DOFR) between health plan and provider. (Wes Cleveland-AMA) • Surplus payment received from better utilization should not be refunded. Contracts Negotiation Process • Data Analysis • Proposal Letter • Make Initial Contact with Payer • Negotiate until agreement is reached • Analyze Counter offers • Escalate to Senior Management • Consider Out of Network Option • Monitor Claims • Re-Negotiate Phase 1: Phase 2: Phase 2: Phase 3: Prepare Negotiate Continue to Negotiate Monitor / Re-negotiate Negotiations Completed We are here Question (You have seen this before) If we have two CPT codes, 52332 which is paid @80% of Medicare, including patient co-payment, by the payer, at $1600/service and code 99213 which is paid @90% of Medicare, including patient co-payment, by the payer, at $60/service and 52332 is performed 100 times a year and 99213 is performed 1000 times a year and I can get a 20% increase on one or the other, but not both codes, which code should I accept the increase on to increase my revenue the most? a) Code 99213 b) Code 52332 10 Best Contracting Practices boils down to… PREPARE NEGOTIATE MONITOR Contracts Negotiation Process • Data Analysis • Proposal Letter • Make Initial Contact with Payer • Negotiate until agreement is reached • Analyze Counter offers • Escalate to Senior Management • Consider Out of Network Option • Monitor Claims • Re-Negotiate Phase 1: Phase 2: Phase 2: Phase 3: Prepare Negotiate Continue to Negotiate Monitor / Re-negotiate Negotiations Completed 10 Best Contracting Practices PREPARE: Best Practice 1: Evaluate top codes and figure out which ones are driving revenue Best Practice 2: Benchmark against Medicare and payers to determine patterns of under reimbursement, use 20/80 rule Best Practice 3: SWOT Analysis for your payer fee schedules: Bundled, Grouper rates, things that make it hard for you to negotiate rates, services paid outside of facility fee e.g., anesthesia, implants Best Practice 4: SWOT Analysis for your practice Best Practice 5: Prepare highly impactful proposal letter 10 Best Contracting Practices NEGOTIATE: Best Practice 6: Deliver highly impactful proposal letter to a contracts manager at the payer, initial follow up and establish rapport Best Practice 7: More Follow up, follow up again and again, keep the payer on the hook Best Practice 8: Evaluate payer proposals and look for ways to optimize counter offers if payer does not provide a proposal, don’t take first “No” as an answer. Be ready to escalate at the right time Best Practice 9: Review contract for language that affects reimbursement MONITOR: Best Practice 10: Monitor payments and re-negotiate when the time frame allows Best Practices 1 and 2: Evaluate and Benchmark What should we ask for? Go back to the payer with a counter proposal: • E and M up 40% • Pathology up 30% • Radiology if below 100%, then up 40% (77014, 77418, 77427) • All other up 15%, including codes not priced as a PCT of Medicare • Codes 52000, 55250, and 55700 add $200 for in office based incentive (In addition to the 15% increase proposal) Note: 52332 left out due to unusually high reimbursement 26 Best Practice 3: Fee Schedule SWOT Analysis (Our offer / proposal to payer) Best Practice 3: More SWOT, In vs. Out of Network Option Best Practice 3: More SWOT, Billed Charges Assessment Another Question / Scenario (Again this is a repeat)… Two practices merge, Practice A and Practice B, into a new practice, named Practice C. Prior to the merger, Practice A had an PPO agreement with Payer 1 that paid, in network, $1,000,000 the 12 months just before the merger. Their overall weighted average rate of reimbursement with Payer 1 is 100% of Medicare. Prior to the merger, Practice B had an in network PPO agreement with Payer 1 that paid $200,000 the 12 months just before the merger. Their overall weighted average rate of reimbursement with Payer 1 is 120% of Medicare. Practice C has decided to remain in Payer 1’s network, as long as their total group reimbursement with Payer 1 increases in aggregate. After a long and difficult negotiation with Practice C, Payer 1 made a final offer of 108% of Medicare, down 12% from Practice B’s current reimbursement. Assuming that, in the absence of change, revenues will remain constant, should practice C accept this new and final offer from payer 1? a) b) Yes No S.W.O.T. – Identify Saleable Solutions and Potential Obstacles to Getting an Increase (Best Practice 4) Strength Opportunities • • • • • • • • Location Size and market presence Practice Patterns Referral Network Practice Collaborations Employer Groups New Services Value Based Contracting Weakness Threats • Competing Practices • Payer Reimbursement Policy • Mergers • Payer initiated ACOs • Out of Network Reimbursement Policy 31 Putting together a highly impactful proposal letter (Best Practice 5) • Establish relationship, why am I writing to you Mr. or Ms. Payer? • Sell your Practice and address payer concerns What are the reasons that it is advantageous to the payer to increase our reimbursement? • Close the “sale”, throw the hook 32 Establish the Relationship • State the reason for contact and establish Practice / Physician relationship with plan – Example of opening paragraph I am contacting you on behalf of Practice NAME to initiate a renegotiation of their current fee schedule. Practice epitomizes “patient centered care” and is consistently performing services at 1/2 the cost of competing practices and is the single largest provider of orthopedic care in the area. Practice been doing so for the past ## years. In the past 12 months, they provided care to #### PAYER covered lives, receiving $$$ for rendered services from PAYER. 33 Sell your Practice and address payer concerns • Network coverage, specialties, clinical efficiency = lower cost, administrative efficiency = lower cost Practice is the largest, most comprehensive orthopedic practice in the greater CITY/COUNTY area. They are the only Practice that provides SPECIAL PROCEDURES. Practice also provides extensive unique office based procedures. Their professional specialties include LIST SUB OR SPECIFIC SPECIALTIES. The effect of handling these procedures in our office vs. the local hospital is a savings of XX to PAYER. 34 Close the sale and “throw the hook” • Closing statement– restate the purpose of the letter and “throw the hook” Following a review of the existing fee schedule, Practice has found that the reimbursement from your organization is not competitive and does not sufficiently reimburse the practice for the high-quality, coordinated care provided to your members. Practice is committed to remaining in PAYER network, but must do so at rates that make good business sense. To that end, Practice has included, in Appendix A of this letter, a reasonable proposal commensurate with the cost and value that Practice provides to your members and your network. I am confident we can come to a mutually acceptable fee schedule agreement. Your written reply to this proposal is requested by no later than DATE (2.5 weeks from date of proposal). In the meantime, if you have any questions about the practice or the attached proposal, please do not hesitate to contact me. 35 Best Practices 6, 7 and 8 • Best Practice 6: Deliver highly impactful proposal letter to a contracts manager at the payer, initial follow up and establish rapport • Best Practice 7: Follow up, follow up again and again, keep the payer on the hook • Best Practice 8: Evaluate payer proposals and look for ways to optimize counter offers. If payer does not provide a proposal, don’t take first “No” as an answer. Be ready to escalate at the right time • Data Analysis • Proposal Letter • Make Initial Contact with Payer • Prepare and deliver proposal letter, initial follow up (Practice 6) Phase 1: Prepare • Follow Up (Practice 7) • Analyze Counter • Negotiate until agreement is reached • Escalate to Sr. Level Manager (Practice 8) • Consider Out of Network Option Phase 2: Phase 2: Phase 3: Negotiate Continue to Negotiate Monitor / Re-negotiate Negotiations Completed • Monitor Claims • Re-negotiate Review contract for language that affects reimbursements (Best Practice 9) • • • • • • • • • • • • Term and termination (90 days without cause) Use of non-par providers, e.g., ancillary services, anesthesia Timely submission of claims (90 is reasonable, shoot for 180) Timely claims payments (30-45 days from receipt of claims) Multiple Procedures / Bi-Lateral 23 hour stays Implants carved out as needed Retrospective review of overpayments, 90 days maximum, reimburse them vs. they deduct automatically Lesser of Language Eliminate “favored nation” language Changes to contract should trigger 30 day termination without cause, fee schedule changes should be categorized as material changes Have your legal counsel review for possible legal concerns Best Practice 10, Monitor Claims New: Value Based Contracting Efficiency (2% if >70 points) Generic Drug Utilization >90%: 75 pts 88 - 89%: 60 pts 86 - 87%: 45 pts Preferred Drug Utilization >90%: 25 pts. 88 - 89%: 20 pts 86 - 87%: 15 pts Qualitative (2% if >70 points) Quantitative (1% if >70 points) In network referrals only Follows Urology Best Practices Guidelines >2.5: 50 pts 2.25 - 2.49: 60 pts 2.0 - 2.24: 45 pts Active EPrescriber: 25 pts 75 pts Patient Satisfaction 3 stars: 25 pts 2 stars: 20 pts 10 Best Contracting Practices PREPARE: Best Practice 1: Evaluate top codes and figure out which ones are driving revenue Best Practice 2: Benchmark against Medicare and payers to determine patterns of under reimbursement, use 20/80 rule Best Practice 3: SWOT Analysis for your payer fee schedules: Bundled, Grouper rates, things that make it hard for you to negotiate rates, services paid outside of facility fee e.g., anesthesia, implants Best Practice 4: SWOT Analysis for your practice Best Practice 5: Prepare highly impactful proposal letter 10 Best Contracting Practices NEGOTIATE: Best Practice 6: Deliver highly impactful proposal letter to a contracts manager at the payer, initial follow up and establish rapport Best Practice 7: More Follow up, follow up again and again, keep the payer on the hook Best Practice 8: Evaluate payer proposals and look for ways to optimize counter offers if payer does not provide a proposal, don’t take first “No” as an answer. Be ready to escalate at the right time Best Practice 9: Review contract for language that affects reimbursement MONITOR: Best Practice 10: Monitor payments and renegotiate when the time frame allows Questions/Comments? • Class schedule/content • Rick Rutherford, CMPE, CHA • Director - Practice Management AUA • Phone: 410-689-3713 • RevolutionSoftware™ Questions • Regina Vasquez, Sr. VP of Accounts – Healthcents, Inc. • Tel: (719) 243-3845 • rvasquez@healthcents.com • Healthcents, Inc. Corporate • Susan Charkin, President – Healthcents, Inc. • charkin@healthcents.com • Steve Selbst, CEO, selbst@healthcents.com • Healthcents Inc. Tel: (800) 497-4970 • www.healthcents.com Thank You for your participation and we wish you succe$$ in your contract negotiations! Your Contracts’ Assessment and proposal letters • Contact Susan Charkin at 831-455-2695 or charkin@healthcents.com If possible (Not required), bring… Revenue collected over a one year period for each payer Overall % Medicare you are currently contracted at by payer Any known issues with a payer, e.g., collections or other Any knowledge you have about your competition and the market that you are in Susan will discuss approaches to moving each of your agreements forward to higher reimbursement or other recommendations This ½ hour high value assessment is included as a part of your class. Also, remember to send a sample proposal letter to support@healthcents.com for feedback