Chapter 37: Orthopaedic Trauma
advertisement

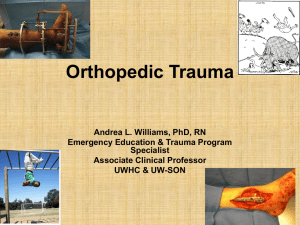
Chapter 37 Orthopaedic Trauma National EMS Education Standard Competencies Trauma Integrates assessment findings with principles of epidemiology and pathophysiology to formulate a field impression to implement a comprehensive treatment/disposition plan for an acutely injured patient. National EMS Education Standard Competencies Orthopaedic Trauma • Recognition and management of − Open fractures − Closed fractures − Dislocations − Amputations National EMS Education Standard Competencies • Pathophysiology, assessment, and management of − Upper and lower extremity orthopaedic trauma − Open fractures − Closed fractures − Dislocations − Sprains/strains National EMS Education Standard Competencies • Pathophysiology, assessment, and management of (cont’d) − Pelvic fractures − Amputations/replantation − Compartment syndrome − Pediatric fractures − Tendon laceration/transection/rupture National EMS Education Standard Competencies Medicine Integrates assessment findings with principles of epidemiology and pathophysiology to formulate a field impression and implement a comprehensive treatment/disposition plan for a patient with a medical complaint. National EMS Education Standard Competencies Nontraumatic Musculoskeletal Disorders • Anatomy, physiology, assessment, and management of − Nontraumatic fractures National EMS Education Standard Competencies • Anatomy, physiology, epidemiology, pathophysiology, psychosocial impact, presentations, prognosis, and management of common or major nontraumatic musculoskeletal disorders − Disorders of the spine − Joint abnormalities − Muscle abnormalities − Overuse syndromes Introduction • Musculoskeletal injuries are one of the most common reasons for seeking medical attention. − Easily identified by pain, swelling, and deformity − May cause short- or long-term disability − Always check for life-threatening injuries first. Functions of the Musculoskeletal System • Supports the soft tissues of the body • Generates movement • Protects fragile organs and structures • Generates blood cells (hematopoiesis) The Body’s Scaffolding: The Skeleton • Axial skeleton − − − − Vertebral column Skull Rib cage Spinal column • Appendicular skeleton − Pectoral girdle − Pelvic girdle − Upper and lower extremities Shoulder and Upper Extremities • The pectoral girdle is composed of: − Two scapulae (shoulder blades) − Two clavicles (collarbone) Shoulder and Upper Extremities • The upper extremity joins the shoulder girdle at the glenohumeral joint. • The forearm is made up of the radius and ulna. Shoulder and Upper Extremities • Hand consists of: − Carpals − Metacarpals − Phalanges Pelvis and Lower Extremities • The pelvic girdle is three bones fused together: − Ischium − Ilium − Pubis Pelvis and Lower Extremities • The lower extremity is the: − Thigh − Leg − Foot Pelvis and Lower Extremities • Three classes of foot bones: − Tarsals − Metatarsals − Phalanges Characteristics and Composition of Bone • Bone shapes − Long bones: longer than they are wide − Short bones: nearly as wide as they are long − Flat bones: thin and broad − Irregular bones: shape serves a certain function − Round bones: found in proximity to a joint Characteristics and Composition of Bone • Typical long bone architecture − Three regions: • Diaphysis • Epiphysis • Metaphysis − Articular surfaces join other bones, forming joints. Characteristics and Composition of Bone • Age-associated changes in bone − Bones decrease in density, leading to: • Loss of height • Changes in facial structure − Osteoporosis is a significant density decrease. Courtesy of Tim Arnett/University College London Joints • Formed when two bones come together − Some are fused and allow for no motion. − Others allow for motion by permitting movement between the two bones. Joints Joints • Types of joints − Fibrous − Cartilaginous − Synovial Joints • Bursa: Padlike sac or cavity in the connective tissue − Contains fluid that helps reduce friction between tendons and bones, or tendons and ligaments − Bursitis: Inflammation of a bursa Skeletal Connecting and Supporting Structures • Tendons connect muscle to bone. • Ligaments connect bone to bone. • Cartilage forms the smooth surface over bone ends where they articulate. The Moving Forces: Muscles • Three types of muscle: − Cardiac − Skeletal − Smooth The Moving Forces: Muscles • Skeletal muscle − Also known as voluntary or striated muscle − Includes all muscles attached to the skeleton − Affected by work to which they are subjected − Attached to bones by tendons The Moving Forces: Muscles Muscle Innervation • Occurs when somatic motor neurons transmit electrical stimuli − Motor units respond by either contracting or not. Musculoskeletal Blood Supply • Upper extremity’s supply comes from the subclavian artery. • Lower extremity’s supply comes from the external iliac artery. Musculoskeletal Blood Supply Patterns and Mechanisms of Musculoskeletal Injury • A pathologic fracture is produced by a force that generally would not cause harm to a healthy bone. Injury Forces and Motions • Direct force − Occurs when the force of an impact is too great to be absorbed by the soft tissue • Indirect force − Occurs when the force applied to one part of the body is transmitted to a weaker area Fractures • A break in the continuity of a bone • Occur when the amount of force applied to a bone overcomes the strength of the bone Fractures • Classification − Based on: • Direction of the fracture line • Number of fractures • Number of cortices involved Fractures • Classification − May be classified based on type of displacement Fractures • Classification (cont’d) − Open fracture: skin is broken. − Closed fracture: skin remains intact. Courtesy of Rhonda Beck Fractures • Signs/symptoms − Pain close to site − Deformity − Shortening − − − − Swelling Guarding Tenderness Crepitus − Exposed bone © Chuck Stewart, MD. Ligament Injuries and Dislocations • Dislocation: Bone is totally displaced from the joint. − Evaluation reveals: • Obvious and significant deformity • Significant decrease in joint’s ROM • Severe pain Ligament Injuries and Dislocations • Dislocation (cont’d) − Subluxation: Partial dislocation − Luxation: Complete dislocation − Diastasis: Ligaments that hold two bones in place are disrupted Ligament Injuries and Dislocations • Sprains: Ligaments are stretched or torn. − Typical symptoms include: • Pain • Swelling • Discoloration over the injured joint Muscle and Tendon Injuries • Strains • Achilles tendon rupture • Injuries related to inflammatory responses − Bursitis − Tendinitis Injuries That May Signify Fractures • Amputation: Separation of a limb or other body part from the rest of the body − May be complete or incomplete Courtesy of Andrew N. Pollak, MD, FAAOS Injuries That May Signify Fractures • Laceration: Smooth or jagged cut caused by a sharp object or a blunt force − Depth of the injury can vary. − Deep lacerations may cause nerve injury. Patient Assessment • Patients may be classified based on injury: − Life- or limb-threatening injury or condition − Life-threatening injuries, simple musculoskeletal trauma − Life- or limb-threatening musculoskeletal trauma − Isolated, non–life- or non–limb-threatening injury Scene Size-Up • Focus on safety and standard precautions. • Consider the mechanism of injury (MOI). • Request additional resources as needed. Primary Assessment • Focus on mental status, ABCs, and priority. • Priorities should include: − Identifying the injuries − Preventing further harm or damage − Supporting the injured area − Administering pain medication if necessary Primary Assessment • Form a general impression. − Evaluate level of consciousness. − If there was significant trauma, musculoskeletal injuries may be a lower priority. • Do not waste time on prolonged assessment. • Complete additional assessment during transport. Primary Assessment • Airway and breathing − Very little else matters if the patient’s airway and breathing are inadequate. − Evaluate the chief complaint and MOI. Primary Assessment • Circulation − Hypoperfusion is a primary concern. • Treat the patient for shock immediately. • Assess for pulses proximal to injury, and note any circulatory changes. − Check for external bleeding. Primary Assessment • Transport decision − Rapid transport should be provided for: • Patients with airway or breathing problems • Patients with significant bleeding • Patients with a significant MOI − Patients with simple MOIs may be stabilized prior to transport. History Taking • Use the standard SAMPLE format. • Obtain information about the incident. − Condition and position of patient before incident − Details of incident − Position of patient after incident Secondary Assessment • Obtain a baseline set of vital signs. • Compare one side of the injured extremity with the other. • Perform and exam, noting DCAP-BTLS. Secondary Assessment • Cover the 6 Ps: − − − − − − Pain Paralysis Paresthesias Pulselessness Pallor Pressure • Pain − Remember OPQRST mnemonic. − Ask the patient to rate pain on a 1 to 10 scale. Secondary Assessment • Inspection − Check for: • Deformity • Skin changes • Swelling • Muscle spasms • Abnormal limb positioning • Increased or decreased ROM • Color changes • Bleeding Secondary Assessment • Palpation − Check for point tenderness. − Identify instability, deformity, abnormal joint or bone continuity, and displaced bones. − Feel for crepitus. − Palpate distal pulses. • Palpate pelvis and upper and lower extremities. Secondary Assessment • Motor function and sensory exam − Check that the patient does not have a lifethreatening injury. − Consider the preinjury level of function. − Compare both sides of the body. Reassessment • The overall goal is to identify the type and extent of the injury and to provide treatment. − Treatment begins in the field. General Treatment of Fractures and Sprains • Fractures − Control external bleeding. − Prevent infection. − Manage internal bleeding. − Immobilize. • Sprains − − − − − Immobilize. Chill. Elevate. Splint. Reduce weight bearing. − Manage pain. Volume Deficit Due to Musculoskeletal Injuries • Prevent hypotension and instability. − Apply pressure. − Splint. − Administer IV fluids. Pain Control • Assess the patient’s pain level. • Try simple measures to control pain. − Splint − Rest and elevation − Heat or ice • If measures fail, administer an analgesic or antispasmodic agent. Cold and Heat Application • During the first 48 hours, cold packs can be used to reduce pain and swelling. • Heat therapy should be avoided in the first 48 to 72 hours, but can then be used to: − Increase blood flow. − Decrease stiffness. Splinting • Decreases pain • Reduces risk of further damage • Controls bleeding Principles of Splinting • Make sure the injured area can be seen. • Assess and record distal PMS functions. • Cover all wounds with a sterile dressing. • Do not move the patient before splinting. • Fractures—immobilize bone ends and joints. Principles of Splinting • Dislocations—splint entire length of bone. • Pad the splint well. • Support the injury and minimize movement. • Splint knees straight, elbows at right angle. • Discontinue traction if patient reports pain. Principles of Splinting • Splint firmly. • Avoid covering fingers and toes. • Apply cold packs, and elevate the limb. • In the case of life-threatening injuries, splinting should not delay transport. Types of Splints • Rigid splint − Inflexible device attached to a limb − Must be padded and long enough − Use two providers to apply. Types of Splints • Sling and swathe − Slings are useful to stabilize upper extremities. − Swathes add more stabilization for: • Injuries to clavicle • Anterior dislocations of the shoulder Types of Splints • Pneumatic splints − Stabilize fractures to the lower leg or forearm − Advantages: • Slow bleeding • Minimize swelling Types of Splints • Pneumatic antishock garment (PASG) − Used for injuries to lower extremities or pelvis. − Be sure to check with medical control. − Document injuries before applying. − Do not remove in the field. Types of Splints • Vacuum splints − Sealed mattresses filled with air and plastic beads − Becomes rigid like a plaster cast Types of Splints • Pillow splints − Used to stabilize an injured foot or ankle − Mold the pillow around the injury and secure in place with cravats. Types of Splints • Traction splints − Used to stabilize femur fractures − Reassess PMS functions after applying. Types of Splints • Buddy splinting − Used for injuries to the fingers and toes − An adjacent finger or toe acts as a splint. − Avoid taping over joints or cutting off circulation. Pediatric Fractures • Weakness of growth plates makes children’s bones vulnerable to fracture. • Tenderness, swelling, and bruising tend to be at a lower level. • Pelvic fractures are unusual. Assessment and Management • When assessing, look for signs of abuse. • Adjust your approach as needed. • Stabilize all sprains and fractures. • Transport child with a family member. Complications of Musculoskeletal Injuries • Likelihood of complication is due to: − Strength of force that caused the injury − Location of the injury − Patient’s overall health Complications of Musculoskeletal Injuries • Paramedics can reduce the probability of long-term disability by: − Preventing further injury − Reducing the risk of wound infection − Minimizing pain − Transporting to appropriate facility Vascular and Neurovascular Injuries • Devascularization: Loss of blood flow to a body part, occurring when blood vessels are damaged following a musculoskeletal injury • Neurovascular injuries occur when the skeletal system is compromised. Vascular and Neurovascular Injuries • Assessment and management − Assess and reassess pulses. − Control bleeding. − Maintain adequate intravascular volume. Compartment Syndrome • Condition that occurs when pressure is too high within fascia • Causes include: − Overly tight bandages, splints, casts, or PASG − Fracture, dislocation, crush injury, vascular injury, soft-tissue injury, bleeding disorder − Fluid leakage or edema Compartment Syndrome • Assessment − The first sign is searing or burning pain out of proportion to the injury. − Neurologic symptoms include: • Paresthesias • Paralysis of involved muscles − Pulselessness is a late sign. Compartment Syndrome • Management − Elevate the extremity to heart level. − Apply cold packs. − Open or loosen constrictive clothing or splint. − Administer high-flow oxygen and isotonic crystalloid solution. Crush Syndrome • Result of prolonged compressive force that impairs muscle metabolism and circulation − When force is released, contents of the muscles enters the systemic vasculature, resulting in: • Decreased blood pH • Hyperkalemia • Renal dysfunction Crush Syndrome • Assessment and management − Before releasing the compressing force: • Assess the ABCs. • Administer supplemental oxygen and isotonic crystalloid solution. • Establish cardiac monitoring. Crush Syndrome • Assessment and management (cont’d) − If ECG shows signs of hyperkalemia: • Administer calcium to stabilize the myocardium. • Administer sodium bicarbonate to promote the intracellular shift of potassium. Thromboembolic Disease • Includes deep vein thrombosis (DVT) and pulmonary embolism • Signs and symptoms of DVT include: − Disproportionate swelling of an extremity − Discomfort in extremity that worsens with use − Warmth and erythema of the extremity Thromboembolic Disease • Signs and symptoms of pulmonary embolism include: − − − − Sudden dyspnea Pleuritic chest pain Tachypnea Right-side heart failure − Cardiac arrest Thromboembolic Disease • Signs and symptoms of fat embolism include: − Tachycardia − Pulmonary congestion − Petechiae − Change in mental status − Organ dysfunction Thromboembolic Disease • Treatment includes: − Maintaining an airway − Supplying adequate oxygen − Maintaining intravascular volume − Providing rapid transport Shoulder Girdle • The shoulder girdle consists of: − Clavicle − Shoulder − Scapula Shoulder Girdle • Clavicle fractures: − Pain in shoulder − Swelling − Unwillingness to raise the arm − Tilting of the head toward fracture • Shoulder injury: − Swelling − Ecchymosis − Pain • Scapular fracture: − Pain that increases with arm abduction − Swelling Shoulder Girdle • Management − Treat shoulder fractures with a sling or swathe. − Treat suspected scapula fractures with full spinal stabilization. Midshaft Humerus Fractures • Assessment − Signs and symptoms include: • Significant swelling • Ecchymosis • Gross instability of the region • Crepitus • Damage to upper arm nerves and blood vessels Midshaft Humerus Fractures • Management − To correct angulated fractures, apply longitudinal traction. − Once the extremity is in place, apply a rigid splint and a sling. − Use cold packs to reduce pain and swelling. Elbow • Distal humerus − Supracondylar fractures typically occur as a result of falling onto an outstretched hand. • Proximal radius and ulna − Radial head fractures occur as a result of falling onto an outstretched hand or from a direct blow. Elbow • Signs of a distal humerus fracture: − Pain in the elbow − Significant swelling − Ecchymosis • Signs of a radial head fracture: − Pain associated with supination or pronation − Ecchymosis Elbow • Treatment of injuries is the same: − Repeatedly assess for compartment syndrome. − Conduct a neurovascular exam before splinting. • If there is a distal pulse, splint. • If there is no distal pulse, consult medical facility. − Transport the patient gently. Forearm • Fractures may involve radius, ulna, or both. • Typically occur as a result of: − Direct blow (nightstick fracture) − Falling onto outstretched hand (Colles fracture) Forearm • Signs of a Colles fracture include: − Dorsally angulated deformity of the distal forearm − Pain − Swelling • Treatment includes: − Splinting − Application of cold packs − Neurovascular exams Wrist and Hand • Scaphoid − Injuries result from falling onto an outstretched hand. • Boxer’s fracture − Occurs after punching a hard object • Metacarpal shaft − Fractures result from a crush injury or direct trauma. • Mallet finger − Occurs when a finger is jammed into an object Wrist and Hand • Signs of scaphoid fracture include: − Pain − Tenderness in the anatomic snuffbox • Signs of a boxer’s fracture include: − Pain over ulnar aspect of the hand − Swelling Wrist and Hand • Signs of metacarpal fractures include: − Abnormal rotation of fingers − Swelling of palm − Pain − Tenderness • Signs of mallet finger include: − Inability to extend distal phalanx − Flexed position is maintained. Wrist and Hand • Management − Secure extremity to an armboard or rigid splint. − Elevate the extremity. Courtesy of AAOS Pelvis • Disruptions of the pelvic ring occur secondary to highenergy trauma. • If pelvic injury exists, suspect multisystem trauma. Pelvis • Structures at risk for injury with pelvis fracture: − − − − − Bladder Urethra Rectum Vagina Sacral nerve plexus • Blood vessels most prone to damage: − Veins within pelvis • Nerves at greatest risk of injury: − Those in lumbar and sacral regions − Sciatic nerves − Femoral nerves Pelvis • Lateral compression pelvic ring disruptions − Result from side body impact Courtesy of Andrew N. Pollak, MD, FAAOS − Lower risk of hemorrhage Pelvis • Anterior-posterior compression pelvic ring disruptions − Occur following a head-on collision or fall − Risk of hemorrhage is high. Pelvis • Vertical shear − Occurs when a major force is applied to pelvis − Results in increased pelvic volume • Straddle fracture − Occurs after a fall when a person lands in the region of the perineum − Carries a risk of complications Pelvis • Open pelvic fractures − Injury to the major vascular structures can cause life-threatening hemorrhage. − May result from penetrating or blunt trauma − Causes massive hemorrhage Pelvis • Signs of a stable injury include: − Pain in the pelvis − Difficulty bearing weight • Signs of profound injury include: − − − − Shock Gross instability Diffuse pain Possible bruising or lacerations − Possible hematuria Pelvis • Signs of a vertical shear include: − Significant shortening of limb − Possible massive hemorrhaging into the pelvis • Signs of an open fracture include: − Blood in the vaginal or rectal regions Pelvis • Assess mental status and ABCs. • Assess the pelvis for bleeding, lacerations, bruising, and instability. • A search for entry and exit wounds should not delay transport. Pelvis • Treatment should include: − Monitoring ABCs − Spinal stabilization − IV access • The goal of management is to: − Reduce bleeding. − Decrease instability. • May include pelvic binder Pelvis • To apply a pelvic binder: − Place binder over the trochanters and below the ribs. − Connect sides. − Apply pressure from either side. − Perform definitive tightening. EMS facility courtesy of St. Charles County Ambulance District, Missouri, © Ray Kemp/911 Imaging Hip • Fractures of the femoral head are usually associated with a hip dislocation. • Femoral neck and intertrochanteric fractures are a result of falls. • Proximal femoral shaft injuries result from a high-energy mechanism. Hip • Signs and symptoms may include: − Pain in the affected hip − Inability to bear weight − Reports of snapping sounds or feelings − Externally rotated and shortened leg − Tenderness to palpation − Swelling, deformity, ecchymosis Hip • Treatment depends on the MOI. − For older patients with a low-energy injury, support the injured extremity with pillows and blankets. Hip • For younger patients with high-energy injuries: − Immobilize. − Establish vascular access. − Monitor for shock. − Transport to a trauma center. Femoral Shaft • Fractures occur following high-energy impacts. • Signs and symptoms may include: − − − − − Angulation Limb shortening Thigh edema Crepitus Neurovascular damage Femoral Shaft • Treatment includes: − Monitoring for shock − Full spinal immobilization − Establishing vascular access − Use of a traction splint or PASG − Administration of pain medication Knee • Fractures result from direct blows, axial load of the leg, or contractions of quadriceps. • Signs and symptoms include: − Significant pain − Decreased ROM − Ecchymosis, swelling, deformity Knee • Management depends on status of pulses − Good distal pulse—splint extremity in position found. − No pulse—seek medical consultation. • Elevate the leg and apply cold packs. • Perform frequent neurovascular checks. Tibia and Fibula • Fractures may result from direct trauma or rotational or compressive forces. • Signs and symptoms may include: − Significant deformity − Soft-tissue injury Tibia and Fibula • Treatment: − Apply a rigid splint. − Administer pain medication. − In case of angulation, attempt to align the leg. − Elevate the extremity to heart level. − Apply cold packs. Ankle • Fractures usually result from sudden, forceful movements of the foot. Courtesy of Andrew N. Pollak, MD, FAAOS Courtesy of Andrew N. Pollak, MD, FAAOS Ankle • Signs of an ankle fracture include: − Pain − Deformity, swelling − Damage to nerve and blood vessels − Compartment syndrome − Chronic pain and arthritis • Treatment includes: − Stabilization − Elevating extremity to heart level − Applying cold packs − Reduction if associated with a pulseless foot Calcaneus • Fractures can occur when a patient jumps and lands on the feet or a powerful force is applied to the heel. • Signs and symptoms may include: − Foot pain − Swelling − Ecchymosis Calcaneus • Treatment includes: − Splinting the extremity with a pillow − Application of ice packs − Spinal stabilization Shoulder Girdle Injuries and Dislocations • Acromioclavicular (AC) joint separation − Usually results from a direct blow to the superior aspect of the shoulder Courtesy of Anand M. Murthi, MD Shoulder Girdle Injuries and Dislocations • Posterior sternoclavicular joint dislocation − Usually results from a direct blow to the clavicle • Shoulder dislocation − Usually results from a fall onto an outstretched arm Shoulder Girdle Injuries and Dislocations • Signs of AC joint separation include: − Pain − Tenderness − Possible protrusion of the distal clavicle Shoulder Girdle Injuries and Dislocations • Signs of shoulder dislocation include: − Severe pain − Decreased ROM − Possible bulge at the acromion − Palpable humeral head − Muscle spasms Courtesy of AAOS Shoulder Girdle Injuries and Dislocations • Treat AC separation with a sling and swathe. • Treat posterior sternoclavicular dislocations by positioning supine with arm abducted. • Treat dislocated shoulders by splinting the extremity in the position it was found. Elbow Dislocation • High risk of neurovascular injury • Usually results from a fall onto an outstretched hand or from hyperextension of the elbow joint − Nursemaid’s elbow is caused by a sudden pull on a child’s arm. Elbow Dislocation • Signs of elbow dislocation include: − Pain, swelling, ecchymosis − Palpable deformity − Locking or resistance to movement of joint Elbow Dislocation • Signs of radial head subluxation include: − Injured arm held in flexion − Refusal to move hand or elbow − Mild swelling • Treat dislocations and subluxations with a splint. Wrist and Hand Dislocation • Occurs when wrist is hyperextended • Signs and symptoms include: − Pain − Swelling − Deformity Wrist and Hand Dislocation • Treatment − Use a padded board or pillow splint with a sling and swathe. − Apply cold packs. − Elevate the injured extremity. − Administer pain medication as needed. Finger Dislocation • Caused by a sudden jamming force or extension beyond normal ROM • Signs and symptoms include: − Pain − Deformity − Compromise of neurovascular structure Finger Dislocation • Splint entire hand in position of function. • Do not attempt to relocate unless directed by medical control. • To reduce a dislocated digit: − If dislocated to the dorsal side, extend it. − If dislocated to the volar side, flex it. Hip Dislocation • Usually occur due to deceleration injures, in which a flexed knee strikes an immobile object with extreme force Hip Dislocation • Conduct a full-body exam. • Splint extremity in the position it was found. • Perform frequent neurovascular checks. Knee Dislocation • Occurs as a result of high-energy trauma or secondary to powerful twisting forces • Signs and symptoms include: − − − − Pain A report that the knee “gave out” Significant deformity Decreased ROM Knee Dislocation • Assessment depends on neurovascular function. − Palpable pulse—splint in position found. − No palpable pulse—reduce prior to splinting. Tendon Lacerations, Transections, and Ruptures • Knee injury − Twisting may result in laceration, transection, or ligament rupture. − Compression injury may result from a blow to the knee. − Hyperextension or tension may occur. • Shoulder injury − Sternoclavicular sprain results from a blow or twisting. − Rotator cuff injury results from pull on the arm, abnormal rotation, or a fall onto outstretched arm. Tendon Lacerations, Transections, and Ruptures • Signs include: − − − − Muscle weakness Pain Edema Loss of ROM • Splint in place. • Apply cold packs. • Elevate extremity. • Assess PMS function. Achilles Tendon Rupture • Usually injured in start-and-stop sports • Signs and symptoms include: − Pain from the heel to the calf − Inability for plantar flexion of the foot − Possible deformity Achilles Tendon Rupture • Perform Thompson test to identify. • Management includes: − ICES − Pain control Nontraumatic Musculoskeletal Disorders • Patients usually do not have an acute lifethreatening condition, but there are neurovascular concerns. • Patients are typically already under a physician’s care. Bony Abnormalities • Osteomyelitis: Bacterial infection of the bone • Signs include: − − − − − Fever Chills Erythema Swelling Pain • Treatment includes: − Recognition − Splinting − Transport Bony Abnormalities • Tumor: Growth of abnormal tissue • Signs include: − Pain − Signs of infection − Swelling or a mass of tissue at site • Treatment includes: − Comparing the extremities for asymmetry − Splinting − Transport Disorders of the Spine • Back pain can be assessed into three categories: − Acute: less than 6 weeks in duration − Subacute: from 6 to 12 weeks − Chronic: greater than 12 weeks Disorders of the Spine • Assessment includes: − Obtaining a history − Examination of the ABCs − Evaluation of pain levels − Physical examination − Neurologic and function examination Cauda Equina Syndrome • Caused by a spinal chord compression • Neurologic involvement • Signs and symptoms include: − Urinary retention − Loss of bowel or bladder incontinence Spinal Stenosis • Narrowing of the spinal canal that can occur at single or multiple levels • Signs and symptoms include back pain: − Exacerbated by prolonged extension − Relieved by rest and spinal flexion Joint Abnormalities • Arthritis: Inflammation of a joint − Multiple etiologies and presentations − Three common types: • Osteoarthritis (OA) • Rheumatoid arthritis (RA) • Gout Joint Abnormalities • Arthritis (cont’d) − Signs and symptoms of OA include: • Progressive pain and stiffness • “Cracking” or “crunching” of affected joints − Signs and symptoms of RA include: • Symmetric involvement of hands, feet, or wrists • Insidious or acute onset Joint Abnormalities • Arthritis (cont’d) − Signs and symptoms of gout include: • Hot, red, swollen joint • Decreased ROM − Signs and symptoms of septic arthritis include: • Patient history of IV drug use • Presentation of toxicity, fever, and altered LOC Joint Abnormalities • Arthritis (cont’d) − Treatment of OA: • Low-impact physical therapy • Pain control • Joint injections − Treatment of RA: • NSAIDs − Treatment of gout: • Stabilization • Pain relief • Transport Joint Abnormalities • Slipped capital femoral epiphysis (SCFE) − Occurs in children and adolescents − Signs and symptoms include: • Difficulty walking and weight-bearing • Noticeable limp • Pain and limited flexion and rotation at the hip Muscle Disorders • Myalgia: Muscle pain that is a symptom of another underlying issue − Short periods of intense pain in a diffuse area − Treatment includes: • Rest • Administration of NSAIDs Overuse Syndromes • Tendinitis: Tendon becomes inflamed. • Bursitis: Bursa becomes painful and inflamed. • Treatment includes: − ICES − Pain medication Overuse Syndromes • Carpal tunnel syndrome: Median nerve is compressed where it passes carpal canal. • Cubital tunnel syndrome: Ulnar nerve is compressed at the cubital tunnel. Overuse Syndromes • Carpal/cubital tunnel syndrome treatment includes: − Recognition, splinting, and transport − Rest of affected extremity − Removal of underlying cause Overuse Syndromes • Polyneuropathy − Occurs when there is simultaneous dysfunction of multiple peripheral nerves − Symptoms can be motor, sensory, or both. Overuse Syndromes • Polyneuropathy (cont’d) − Guillan-Barre syndrome • Inflammation and demyelination of peripheral nerves − Poliomyelitis − Asymmetric paralysis of lower extremities − Does not include sensory loss Soft-Tissue Infections • Myositis: Inflammation of the muscle − Signs and symptoms include: • Signs of infection • Muscle weakness • Fatigue on exertion − Treatment is based on presentation. Soft-Tissue Infections • Fasciitis: Inflammation of the fascia − Signs and symptoms include: • History of vector transmission • Red or warm skin • Night sweats/chills • Vomiting/diarrhea − Transport to the hospital for diagnosis. Soft-Tissue Infections • Gangrene: Caused when the blood supply to tissue is interrupted or stopped − Characterized by a bad odor − Late signs include discoloration of limbs. − Take standard precautions, and transport rapidly. Soft-Tissue Infections • Paronychia: Bacterial infection of the hand − Spreads to circulatory and lymphatic systems − Characterized by a small pustule or redness − Transport for antibiotic treatment and/or lancing of abscesses. Soft-Tissue Infections • Flexor tenosynovitis of the hand: Caused by infection resulting from penetrating trauma − Signs and symptoms include: • Limited mobility • Swelling • Redness • Transport for treatment. Summary • Injuries and complaints related to the musculoskeletal system are one of the most common reasons that patients seek medical attention. • Musculoskeletal injuries are sometimes very dramatic, but attention should not be focused on them until life-threatening conditions have been addressed. Summary • You have a vital role in reducing the complications associated with musculoskeletal injuries by promptly and effectively splinting injured extremities. • Assume the existence of a fracture whenever a patient who reports a musculoskeletal injury has deformity, bruising, decreased range of motion, or swelling. Summary • Always perform and record an accurate neurovascular examination before and after splinting an injured extremity. • Check penetrating injuries for underlying fractures or other musculoskeletal injury. • Musculoskeletal injuries are likely to be accompanied by hemorrhage. Summary • When a dislocation is associated with absent distal pulses, obtain medical direction to determine whether the injury should be reduced. • Look for injuries to the chest and abdomen, and fully stabilize the spine when patients have evidence of a high-energy injury. Summary • Because fractures may be associated with significant blood loss, resuscitation with IV fluid may be necessary. • Pelvic fractures are potentially lethal. • Posterior sternoclavicular joint dislocations are potentially fatal. • Never forget the ABCs! Summary • Children’s bones contain weak growth plates, making them more susceptible to fractures than sprains. • Remember to consider whether the MOI suggests possible abuse. • Musculoskeletal injuries can lead to numerous complications. Summary • Blood vessels can be damaged following a musculoskeletal injury. • Neurovascular injuries include impalement or laceration of nerves of a plexus, leading to a neurologic deficit. • Compartment syndrome occurs when bleeding or swelling increases to the point that the pressure within that compartment impairs circulation. Summary • Crush syndrome occurs when a prolonged compressive force impairs muscle metabolism and circulation. • Nontraumatic musculoskeletal disorders can be highly complex, encompassing aspects of rheumatology, neurology, oncology, hematology, and infectious diseases. Summary • Slipped capital femoral epiphysis (SCFE) is a problem in the hip that affects the epiphysis of the femur. • Types of arthritis include osteoarthritis, rheumatoid arthritis, gout, and septic arthritis. • Muscle disorders include myalgia and myositis. Summary • Tendinitis and bursitis occur from frequent, repetitive use that results in inflammation. • Paramedics may encounter patients with numbness, tingling, or pain in their wrist or hand. This can be from carpal tunnel or cubital tunnel syndrome. • Polyneuropathy, or peripheral nerve syndrome, stems from actual nerve damage of the peripheral nervous system. Summary • Soft-tissue infections include fasciitis, gangrene, paronychia, and flexor tenosynovitis of the hand. • Fasciitis is inflammation of the fascia. • Gangrene is caused when blood supply to tissue is interrupted or stopped. • Paronychia is a bacterial infection located near the nail plate. Summary • Flexor tenosynovitis of the hand is caused by an infection that is usually the result of penetrating trauma to the hand. Credits • Chapter opener: © Mark C. Ide • Backgrounds: Orange – © Keith Brofsky/Photodisc/Getty Images; Gold – Jones & Bartlett Learning. Courtesy of MIEMSS; Blue – Courtesy of Rhonda Beck; Purple – Jones & Bartlett Learning. Courtesy of MIEMSS. • Unless otherwise indicated, all photographs and illustrations are under copyright of Jones & Bartlett Learning, courtesy of Maryland Institute for Emergency Medical Services Systems, or have been provided by the American Academy of Orthopaedic Surgeons.