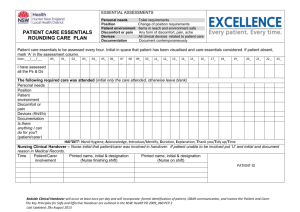
Effective Communication & Handover in Healthcare
advertisement

Communication over the phone & handover Effective communication is very important. • From 1995 – 2005 JCAHO reviewed over 2537 sentinel events in General Hospitals and Emergency Departments • Communication issues identified as being the root cause and the major contributor in these events • In 2005 nearly 70% of sentinel events, the root cause was communication. Why does communication break down? • Different communication styles • High level of activity • Frequent interruptions • No standardization in organizing essential information What Can Go Wrong? • CONCERN was communicated – BUT: • PROBLEM: was not clearly stated • PROPOSED ACTION: didn’t happen • DECISION: was not reached What is SBAR? • The SBAR model is a simple method to help standardize communication • SBAR allows all parties to have common expectations: • What is going to be communicated • How the communication is structured • Required elements • Focuses on the problem, not the people So What is SBAR? • Situation: Give a brief introduction, the punch line (5-10 seconds) of what you are calling about. • Background: Give data relevant to the problem including history and clinical findings. • Assessment: State what you think the problem is but give an indication of severity • Recommendation: What do you think need to be done for this patient and if appropriate get an estimated time frame for a response. SITUATION • State: your name and unit • I am calling about:: (Patient Name & bed number) • The problem: The reason I am calling ….. Situation (Scenario 1) • “Good evening sir. This is Dr. XYZ, a Resident doctor on duty, I just saw Mr. ABC on bed no 9 in the ward. I am contacting you because Mr. ABC is complaining of severe abdominal pain”. Background • Information about the patient that the doctor needs to know that will help in identifying the source of the problem as well as its potential solution. • This includes medical history and clinical findings. Background (Scenario1) • “He got admitted to the hospital five days ago with appendicitis and you had done appendicectomy on him three days back.” Assessment • The assessment is when the doctor recalls what was observed when checking the patient. • This includes the information gathered during the physical examination. • The most common information that is obtained from patients are their vital signs: blood pressure, heart rate, temperature and respiratory rate. Assessment (Scenario1) • “I found him the bed groaning with his hand on his abdomen. He states the pain is worse today even after taking the pain medication you already ordered. His temperature is raised and incision site looks good, but his blood pressure is reduced and he is tachycardic and tachypnoeic. His saturation is 85% on air. I think he needs intensive care monitoring” RECOMMENDATION • State what you would like to see done: • • • • Transfer the patient? Change treatment? Come to see the patient at this time? Talk to the family and patient about….? Recommendation (Scenario1) • Could you please come to see him now? • Do you want me to get US abdomen done? • How long it will take for you to come down to see this patient?” Scenario 2 • You have seen 58 yr old patient with chest pain. He has family history of heart disease. He is diabetic and hypertensive. Before coming to the hospital he has seen the GP for this chest pain and has been given antacids. • On examination his HR is 118/min regular but only carotid and femoral pulses are palpable. He has cold peripheries and his BP is 75/50mmHg. JVP 3 cm. HS are normal and chest is clear. Pulse oximetry is not picking up signal. On examination of abdomen he has mild splenomegaly but no jaundice. He has no palpable Urinary bladder and he says he has not passed urine for the past 16 hours. • You are consulting your Senior …. Scenario 2 - SBAR • Situation: 58 yr old with severe shock • Background: Cardiovascular risk factors for IHD. Currently had angina type chest pain. BP 75/50, HR 118/min, JVP 3cm, cold peripheries. • Assessment: Severe cardiogenic shock • Recommendation: Please can you come to see him immediately. Would you like me to prepare for any inotropic infusion while you are coming? How soon can I expect to see you? Handover • Transfer of responsibility from one care giver to other. • Goal is to provide timely, accurate information about • • • • a patient's care plan, treatment, current condition and any recent or anticipated changes. • Handover is a crucial communication, if carried out poorly can obviously compromises patients safety. Handover • Handover in ICU during shift change • Hand over on the phone of particular patient Tools to assist handover • Forms and checklists • Five P’s • • • • • Patient: Name, Identifiers, Age, Sex, Location Plan: Patient Diagnosis, treatment plan, next steps Purpose: Provide a rationale for the care plan Problems: Explain what's different or unusual about this specific patient Precautions: Explain what's expected to be different or unusual about the patient Tools to assist handover • Forms and checklists Tools to assist handover • Forms and checklists Handover in ICU Tools to assist handover • Background clinical information • ‘ He is 60 yr old pt, known to have COPD and HT’ Tools to assist handover • Course of acute illness ‘He has septic shock from perforated ischemic bowel and developed acute kidney injury. He has been extubated for the past 24 hours, off antibiotics and is on intermittent haemodialysis’ Tools to assist handover • To do list ‘He needs to have a new haemodialysis catheter inserted tonight as existing one is having inadequate flow’ Tools to assist handover • Anticipation of events ‘In case his blood pressure drops again, I’d escalate antibiotics and ask for CT scan of the abdomen’ Handover of a patient on the phone Tools to assist handover • I PASS THE BATON: This technique is designed to assist with both simple and complex handoffs. • I : Introduction - Individuals involved in the handoff identify themselves, their roles and jobs • P : Patient - Name, Identifiers, Age, Sex, Location • A : Assessment - Present chief complaint, vital signs, symptoms and diagnosis • S : Situation - Current status, response to treatment • S : Safety concerns - Critical lab values and reports, socioeconomic factors, allergies • B : Background - Previous episodes, Current medications, and family history • A : Actions - Details about what actions were taken and/or are required • T : Timing - Level of urgency and explicit timing • O : Ownership - Who is responsible? • N : Next - What will happen next? Plan of action Introduction Hi I’m Dr. XYZ. I am the registrar on call. I would like to handover a patient to you Patient He is 60 year old man called ABC, hospital no 11111, in ward B Assessment His main problem is AKI due to obstructive uropathy. He is anuric. He is a bit tachypnoeic and tachycardic HR 100/min. BP is normal Status He has just received dialysis for fluid overload and hyperkalaemia. He is not acidaemic. Safety Concerns We are mainly now concerned about his fluid overload causing breathing difficulty and hyperkalemia. There are no other safety concerns at present Background He has no relevant past medical history. He is allergic to Quinolones Action I have just asked for chest xray and sent blood for urgent potassium. Can you please check it? Timing …..which should be available in next 30 min. Ownership If there is a problem his consultant is Dr. xxxx He is looking after this patient Next If the X ray is still showing signs of fluid overload and potassium is still high, he may need more dialysis. Key points • Handover is a crucial communication • Written notes should be used to supplement a verbal handover • Do not overwhelm the recipient with irrelevant information • Use a system to avoid omitting something vital. •Thanks!