OHA Update

REVENUE CYCLE IN 2016
OHA UPDATE
December 11, 2015
WHAT’S UP FOR 2016
• Federal o Medicare 2016 CY Hospital OPPS Final Rule o Growing Pains for Medicare Hospital P-for-P Programs o Value-Based Purchasing Rated Poor by GAO o Comprehensive Care Joint Replacement Model Challenged o Medicare Medical Review Programs Expanding o RAC Contract Re-Bid Vacated; What Now? o What About Medicaid RAC? o ICD.10 Conversion Follow-up
• State o Ohio Medicaid Hospital Policy and Payment Updates o Medicaid EAPG OPPS o Medicaid Episodes-of-Care Expanding into Payments o Other Medicaid Initiatives
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 2
Medicare CY 2016 OPPS Final Rule
Big Cut in Annual Update for Lab Services is Controversial o Final Rule Out Oct. 30; Effective Jan. 1, 2016 (Mostly!) o Usual Mix of Updates to APC Groups & Weights, Inpatient-Only
Procedures and Quality Reporting Rule o .2% Cut for Alleged Increases Related to “Two-Midnight Rule”
Payments is Still in (for Now)
– CMS States it Will Comment Later o Three Big Updates:
• “Two-Midnight” Inpatient Admission Policy Hardened
• QIO (Ohio’s is KePRO Area 4 ) Takes Over Post-Pay
Reviews of Short-Stay Medical Necessity (Site of Service)
• Started Oct. 1;
Some Details Available in Webinar Materials
• “Significant” Problems to be Referred to Medicare RAC
• Does Not Affect RAC Reviews of Physician’s Order
• Reduced Annual Payment Update by 2% to Pay for
Unbundled Lab Services
• Will Cause Negative Update for Most Hospitals in CY 2016
• Watch for Advocacy/Legal Action on This
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 3
MEDICARE PAY FOR PERFORMANCE PROGRAMS
The Medicare Update Factor is Under Siege
Behavioral
Offset
Productivity Offset
Readmissions
Penalty
Supplemental
Reduction Factor
Medicare
Hospital
Update Factor
Quality Pay-for-
Reporting Reduction for Non-Compliance
Value-Based
Purchasing
Pool Carve-Out
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM
Meaningful Use
Reduction for Non-
Compliance
Healthcare-
Acquired
Conditions
Penalty
December 11, 2015 4
-2
-3
-4
0
-1
2
1
3
4
MEDICARE IPPS UPDATE & PAYMENTS AT RISK
UNDER PAY FOR PERFORMANCE PROGRAMS
Marketbasket
Effective Market
Basket
Value Based
Purchasing
2013 2014 2015 2016
Readmissions
Reduction
Hospital Acquired
Conditions
Ohio Hospital Association | CELEBRATING 100 YEARS | December 11, 2015 5 AAHAM
MEDICARE P-FOR-P PROGRAMS
…But What do They Add?
• Readmissions Reduction
Policies Show Promise
• VBP Shows Little Shift in
Hospitals’ Quality Performance that Would Not Have Occurred
Without the Program
• VBP Eligible Hospitals
Received <.5% of Applicable
Medicare Payments,
Compared to 1% to 1.5%
Reduction To Annual
Inflationary Update
• Smaller VBP Hospitals Had
Larger Negative Effects
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 6
Medicare Comprehensive Care Joint Replacement Model
Demo in 67 CBSAs – Three in Ohio o Start Date: April 1, 2016; Duration: Five Years o Applies Only to IPPS Hospitals in Covered CBSAs Not Already in BCPI for Lower-Extremity Joint Replacement o Episodes Triggered by Discharge under MS-DRGs 469 & 470 o All Part A and B Services Related to the Major Joint Replacement
Included in a 90-Day Episode o Payments Retroactively Reconciled to a Target Price for the Episode. o No Change to Current Billing or Initial Payment Practices o Target Price set at Blend of Historical Hospital-Specific Cost and
Regional Cost; Regional Component Increases Over Time o Expected Spending Discounted by 2% to Reach Performance Period
Target Price o Hospital's Financial/Quality Outcomes Could Result in Incentives (Year
One) or Penalties (Year Two and Beyond)
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 7
Medicare Comprehensive Care Joint Replacement Model
Industry Reaction is Mixed o Should Ease Process for Beneficiaries, Lessen Cost-Sharing
Over Time, but… o Disconnect Between Cost of Care and Target Price for Care
Delivered in Bundle o No Price Negotiation – Medicare Sets the Target Price o Over-Emphasis on Hospital Role in Bundled Episode
• Focus is on Medicare Spending; Hospitals Have Limited
Control Over Non-Hospital Care Delivered in Episode
• All Covered Providers’ Services Included in Bundle, but Only
Hospital’s Payments Affected o Focus is on Penalizing “Over-Spending” Hospitals; No Bonus for
Low-Cost - High Quality Performers o Limited Ability for Hospitals to Control Medicare Covered &
Payable Services; Little Room to Innovate o Could Impact Patient Access to Covered Care
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM 8 December 11, 2015
HOSPITAL UTILIZATION REVIEW PROGRAMS
Decreasing Bang for Increasing Buck o Multiple Contractors & Auditors with Differing Rules,
Targets, Procedures, Experience & Authority o Duplication of Effort; Little Coordination Between
Payers o Increasing Cost of Compliance
• Personnel
• IT
• Claims Management o Conflicting and Proprietary Criteria & Guidelines o Misaligned Incentives
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 9
MEDICARE HOSPITAL MEDICAL REVIEW PROGRAMS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 10
MEDICARE RAC CONTRACT RE-BID
Medicare RAC Contract Re-bid (Again!) o New Regions Drawn to Re-Weigh Claims Volume o Existing Region B Subdivided
• At Least Some Region B States Must Switch Contractors o Limited “Old” Contract Activity Expanding
• (Mostly) Automated Reviews & DRG Validations
• Effective Through Dec. 31, 2015 (Expect Extension) o Details and Review Issues Listed on CGI Webpage
• DRG Payment Complex Reviews (Over/Underpayments)
• Code and Unit Overpayments Automated Reviews
• Drug Unit Overpayments o CGI Also Cleaning Up Old ADRs for Records Never Submitted
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 11
MEDICARE RAC MAPS – OLD VS. NEW
Current (Old Contracts) New Contracts
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 12
CMS RAC PROCESS IMPROVEMENTS
Now Being Phased in Over Contract Extensions (Indicates New SOW) o Expanded Discussion Periods o Delayed Award of Contingency Fees o Additional Program Education and Outreach & (QIO or
MAC; Who’s on 1 st ?) o New Standards for RAC Accuracy & Overturned Denials o Faster Review Turnaround o Limits on Look-back for Patient Status Reviews o ADRs Must be Diversified o ADR Limits Adjusted to Provider Compliance Rates
(Benchmarks Still Under Discussion) o Provider Satisfaction Surveys (New Contractor will Perform) o Short-Stay IPPS Policy Still Under Consideration!
o … and Effects of ALJ Appeals “Buy-out” Still Unclear
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 13
WHAT ABOUT THE MEDICAID RAC?!
RFP Out for New Contractor, but no Takers o CGI Contract Ended in July, 2014 o ODM Assumed Responsibility for Outstanding Reviews,
Recoveries and Appeals
• ODM Will Internally Correct Claims Recovered in Error
• ODM will Complete any Reviews of ADRs/Medical
Records Sent to CGI Before Contract Ended
• ODM Will Manage Any Requested Appeal CGI did not
Complete
• Interest on New Recoveries Will Only Accrue to
Original Overpayment Notification or Appeal Request o No News on Next Steps
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 14
ICD.10
• No Major Breakdowns
• Some Hospitals are
Reporting Payment
Slowdown and an Increasing
Number of Glitches
• Watch out for BWC Self-
Insured Employers / TPAs;
They are Not Required to be HIPAA Compliant!
• OHA is Surveying Finance
& ABC Committees
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 15
HCAP 2016 o Ohio 1 st State to Reform Medicaid DSH Formula in
Response to Medicaid Expansion & Federal DSH Audits o 2014 Program Emphasis Shifted From Uncompensated &
Charity Care to Medicaid Shortfall & Uncompensated Care o OHA Recommended Transition Period Over 2 – 4 Years
• Why: Usable Medicaid Cost Report Data is Generally
Two Years Old (Pre-Medicaid Expansion)
• Response: Keep $100M in Pot 3A in 2014 as Cushion
• Transfer $36M of Pot 3A to Pot 2 in 2015
• Transfer Half of Remaining Funds in Pot 3A in 2016
• Transfer All Remaining Funds to Pot 2 in 2017.
• Request ODM File Multi-Year Medicaid State Plan
Amendment to Avoid Duplicate CMS Reviews.
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 16
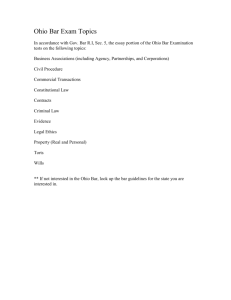
HOSPITAL PAYER MIX FY13-15
35%
30%
25%
20%
15%
15%
18%
25%
29%
28%
33%
10%
5%
6%
4%
3%
0%
% of total charges billed for % of total charges billed for uninsured Medicaid
% of total billed charges for commercial
*Does not include children's hospitals data
FY13
FY14
FY15
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 17
OHIO HOSPITAL CARE ASSURANCE PROGRAM
HCAP TIMELINE – CY/FFY 2015
CMS APPROVES 2014
CHANGES
(JUNE but CMS has until 7/30 – 90 th day)
ODM RESPONDS TO
RAI
(NOVEMBER)
CMS APPROVES 2015
(DECEMBER)
ODM INITIATES 2014
ASSESSMENTS/PAYM
ENTS
(JULY)
CMS ISSUES RAI
(OCTOBER)
ODM INITIATES
ASSESSMENTS/PAYM
ENTS FOR 2015
(JANUARY/FEBRUARY)
ODM FILES 2015 SPA
(JUNE/JULY)
CMS IGNORES SPA
FOR 89 DAYS
(OCTOBER)
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 18
HCAP 2015
PRELIMINARY MODEL
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 19
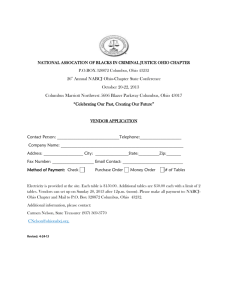
FEDERAL MEDICAID DSH FUNDING
HCAP Funding 2014 - 2025
Baseline vs. SGR Fix Levels
$900
$800
$700
$600
$500
$400
$300
$200
$100
$0
2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025
Baseline Program Funding Adjusted Program Funding
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM
FFY
2014
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
Change in Net
Gain ($)
Change in Net
Gain (%)
$0 0.0%
$0
$0
0.0%
0.0%
$0
($74,365,059)
($108,895,256)
($142,375,927)
0.0%
-17.7%
-25.2%
-32.1%
($175,902,095)
($209,474,896)
($243,095,496)
($276,765,091)
($278,824,088)
-38.6%
-44.7%
-50.4%
-55.8%
-54.7%
December 11, 2015 20
2016 MEDICAID PAYMENT & POLICY UPDATES o HHTLs to End
• ODM will Simply Release Draft and Final Rules o Pre-Certification Suspended Until January 2017 o Other Payment Provisions
• 5% Outpatient Payment Reduction to Non-Childrens Hosps.
• New Pre-Admission “DRG Window”
• Changes to Paragraph L Exceptions
• Medicaid/Medicare Cost Sharing Policy Expanded To Docs
• NCCI Edits Go Into Effect on Outpatient Claims Jan. 1
• Revenue Lines on Individual Outpatient Bills Must be in
Date-of-Service and Revenue Code Order
• New EOB Codes on Permedion Denials o Updated Hospital Billing Guidelines Available
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 21
MEDICAID DSH AUDITS
FFY 2011 & 2012 o ODM Delivered 2011 Final Report to CMS in Dec. 2014.
• No response Yet
• 11 Hospitals with Adjusted DSH Limit Below 2011
Payment o FFY 2012 Report Due to CMS in December 2015
• 183 Hospitals Audited – All Had Adjustments of Varying Size
• 14 Hospitals with Adjusted Hospital-Specific DSH Limit
Below 2012 Payment o Common Issues Cited by Myers & Stauffer
• Patient Logs Submitted, but no Corresponding Data on Cost
Report
• Reverse of Above: Cost Report Data, but No Log
• Logs Not in the Required Format
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 22
MEDICAID DSH AUDITS
FFY 2013 Audit
• Report Due to ODM in June 2016; Due to CMS in
December 2016
• Desk Reviews Underway, with On-site Reviews
Expected February – April 2016
– High DSH Payment
– Proximity of HCAP Payment to DSH Limit
– Subject to On-Site Audit in Previous Year
– May Also Include Non-Financial Program Exam
• New Logs for MyCare Ohio & Medicaid-Eligible, but not ODM-Paid Costs and Payments
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 23
MEDICAID EAPG OPPS
Background
• Enhanced Ambulatory Patient Groups
– Created by 3M
– In Use at 13 State Medicaid or Blue Cross Plans
– Designed for Outpatient Encounters and Services
– Replaces Ohio Medicaid Outpatient Fee Schedules
– Groups Services with Similar Cost & Resource Use
– Applicable to All Ambulatory Settings
• Same-Day Surgery
• Outpatient Hospital ED & Clinic Visits
• Freestanding Outpatient Diagnostic & Treatment Facilities
• Ohio Implementation Scheduled July 1, 2016
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 24
MEDICAID EAPG OPPS
EAPGs vs. DRGs
DRG
– Inpatient Admission
– Discharge Date Defines
Code Sets
– Uses ICD-9-CM or ICD-
10-CM Diagnosis &
Procedure Codes
– Only One DRG per
Admission
– Employs Some Charge
Bundling
EAPG
– Ambulatory Visit
– Claim “FROM” Date Defines
Code Sets
– Uses ICD-9-CM or ICD-10-
CM Diagnosis Codes &
HCPCS/CPT, Procedure
Codes
– Multiple EAPGs May be
Assigned per Visit
– Employs Significant Charge
“Packaging,” Consolidation &
Discounting
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 25
MEDICAID EAPG OPPS
EAPGs vs. ODM Fee Schedules
FEE SCHEDULES EAPG
– Uses ICD.9.CM or ICD.10.CM
Diagnosis Codes &
HCPCS/CPT Procedure Codes
– Uses ICD.9.CM or ICD.10.CM
Diagnosis Codes &
HCPCS/CPT Procedure Codes
– 11 Fee Schedule Groupings
(Facility Fees, Surgical & Other
Procedures, and Diagnostic
Tests)
– 564 EAPGs in Five Major
Categories (Significant, Ancillary
& Incidental Procedures,
Medical Visit and Drugs)
– Multiple Fee Schedule
Payments Likely Per Visit
– Multiple EAPGs Possible per
Visit
– Employs CCI Edits, but Little
Charge Bundling/Packaging
– Permits Exception Payments for
High Cost Pharmacy, Medical
Supply & Device Costs, and for
Outpatient Observation
– No CCI Edits in 3M Model, but
Employs Significant Charge
Packaging, Consolidation &
Discounting
– No Exception Payments
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 26
MEDICAID EAPG OPPS
ODM OPPS Policy Decisions Completed
• Applies to ALL Hospitals
• Most of 3M OPPS Architecture Adopted
• Ohio-Specific EAPG Weights Determined
• Full Packaging, Consolidation & Discounting
Applied
– Six Month Transition to Full Packaging for “Paragraph
L” Fee Schedule Exceptions, and to Payments for
Outpatient Observation and Dental Services
• Transition Period from Fee Schedules to OPPS for up to Three Years Included
– Stop Loss/Stop Gain Transitional Corridor Likely
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 27
MEDICAID EAPG OPPS
OPPS Policy Decisions Yet to be Made
• Hospital Peer Groups
– Will be Used in Both OPPS and Rebased IPPS
– OHA Recommending Five In-State Peer Groups
(Childrens, Teaching, Urban Non-Childrens Non-
Teaching, CAH, and Non-CAH Rural)
– ODM Still Testing Other Options, Mainly Involved with how to Categorize Teaching & Children’s Groups
• Base Rates to be Determined Once Peer Groups are Identified
• Application of Fiscal Impact Targets Comes Next
• Final Piece Involves Length of Transition &
Gain/Loss Corridors
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 28
EPISODES OF CARE
Demonstration Model Basics o Part of State Improvement Model (Also Includes Patient-
Centered Medical Homes) o State’s Goal: 80-90% of Ohio’s Population in Some Value-
Based Payment Model Within Five Years o EoC Payment Methodology Phase-in
• 2016 Pegged as Performance Year; Risk/Gain-Sharing to Start in 2017.
• Commercials Will Adopt ODM Methodology with
Separate Metrics
• Principal Accountable Providers (PaPs) Must Meet
Quality Metrics to Receive Gain-Sharing
• Medicaid Managed Care Plans Will use ODM Metrics
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 29
EPISODE-BASED PAYMENTS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 30
EPISODE-BASED PAYMENTS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 31
EPISODE-BASED PAYMENTS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 32
EPISODE-BASED PAYMENTS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 33
EPISODE-BASED PAYMENTS
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 34
EPISODES OF CARE
OHT/ODM Outline Encouraging Program Specifics
• Medicaid Gain/Risk Sharing Performance Period Starts 1/1/16, but Payments Will not be Affected Until 1/1/17
• Commercial Payers will Independently Determine Metrics
• 2017 Payments will be Budget Neutral, Assuming No Change to
PAP “Curve”
• ODM will set Cost & Quality Thresholds for FFS and all
Medicaid Managed Care Plans
• Wave One Performance Metrics will Limit Risk Sharing to 10%,
Again, Assumning no Change to Behavior
• Gain-Sharing PAP’s Must Meet Quality Metrics
• Metrics will be Identified
• Quality Metrics will be Set at Top Quartile, but 2017 Thresholds will be set to Allow 75 Percent of Providers to Potentailly Share Gain.
• Metric Thresholds will “Ramp up” to Top Quartile by 2021 kigvg
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 35
POTENTIALLY PREVENTABLE MEDICAID
READMISSIONS
o 3M Product Used to
Calculate PPR Rates o Includes All Hospitals Within
30-Day Period o Compares Actual PPR Rate to Expected Rate o State Average at 9.2%:
State’s goal: 1% Annual;
Decrease o 2015 - Reporting Only;
Released in Feb. & July o Includes Hospital Data 2010
– 2014; MCP Data 2013 -
2014 o Payments Tied to Results in
2016 (?)
Ohio Hospital Association | CELEBRATING 100 YEARS | AAHAM December 11, 2015 36
OHA collaborates with member hospitals and health systems to ensure a healthy Ohio
Charles Cataline
Vice President, Health Economics & Policy charles.cataline@ohiohospitals.org
—
Ohio Hospital Association
155 E. Broad St., Suite 301
Columbus, OH 43215-3640
T 614.221.7614 ohiohospitals.org