Presenting - Minnesota Women Physicians
advertisement

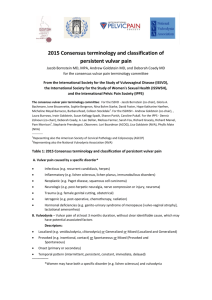
Bridget Keller, MD Stacey Seibel, PhD, LP 28 y.o. G1P1001 married female presents with chief complaint of dyspareunia and vulvar pain. Pain is burning, raw and occurs with sexual intercourse, touch and tampon use. Pain is localized to a specific area that she can show you. She has seen at least 3 other physicians for this complaint with no relief. She is frustrated. Evaluation? Diagnosis? Treatment options? Discuss diagnosis and classification of vulvodynia Review vulvar anatomy Identify treatment strategies and discuss the importance of multidisciplinary treatment ISSVD Definition “Chronic vulvar discomfort, most often described as burning pain, occurring in the absence of relevant visible findings or a specific, clinically identifiable neurologic disorder” Diagnosis of exclusion Prevalence Incidence 1 in 4 women 3.2% affected at some point in life 3-7% reproductive aged women All ethnicities Highest incidence of symptom onset women age 18-25 Vulvar pain due to a specific disorder (not vulvodynia) Infection Inflammatory Lichen sclerosus, contact dermatitis Neoplastic Neurologic Pudendal nerve entrapment, spinal nerve compression Generalized Provoked (sexual, non sexual or both) Unprovoked Mixed Localized Provoked (sexual, non sexual or both) If confined to vestibule – “Provoked vestibulodynia” Unprovoked Mixed Vulvar pain related to a specific disorder is not considered vulvodynia Infections Inflammatory or dermatologic condition Neoplasm Neurologic disorder (nerve entrapment, spinal nerve compression) Chronic pain/discomfort around opening of vagina (e.g., the vestibule) Often inflammation and irritation around the vestibule Resultant pain with vaginal penetration (e.g., intercourse; tampon insertion) Presenting Complaint: “Sex hurts” Pain can also occur with wearing tight clothing, sitting, exercise, and pelvic exams Generalized vulvodynia – neuropathic pain syndrome Co-morbid conditions Interstitial cystitis Fibromyalgia IBS Depression Chronic fatigue syndrome Clinical History Risk factors Co morbid conditions Psychosocial issues Physical Exam Visual exam Cotton swab test Neurosensory exam Pelvic floor exam Clinical History Risk factors Co morbid conditions Psychosocial issues Physical Exam Visual exam Cotton swab test Neurosensory exam Pelvic floor exam Standard of care is a combination of medical, physical therapy and/or psychotherapy services Individualized multidisciplinary care The majority of women with vulvodynia can develop healthy, painless (and enjoyable) sexual relationships Primarily treatable Remission rates 17-25% in population based studies Vulvar self care Topical medication Lidocaine, estrogen Oral medication TCA, Gabapentin Injectable medication Nerve blocks Surgery Vestibulectomy Dietary modifications Topical Medications/vestibulodynia Zolnoun, et al 5% Lidocaine ointment to affected area at night. Soak cotton ball in 5% ointment and apply cotton ball directly to vestibule nightly for 3 months. 36-76% improvement in ability to have intercourse at follow up. 2% Lidocaine jelly to affected area 15-20 minutes prior to sexual activity and as needed up to 5 times daily Reduces allodynia response on vulva Oral medications/unprovoked generalized vulvodynia Amitriptyline 10 mg q HS increase weekly up to 150 mg Gabapentin 300 mg PO increase by 300 mg every 3 days to 3600 mg daily Systematic Review states insufficient evidence to support use of antidepressant (JSexMed 2012;Sept 13) Oral Despiramine and Topcial Lidocaine for provoked vestibulodynia: a RCT (Obstet Gynecol 2010;116-58493) Oral despiramine and topical lidocaine as monotherapy or in combination failed to reduce pain more than placebo Vestibulectomy For provoked vestibulodynia only Superficial removal of affected area of vestibule with or without vaginal advancement May be done in office under local anesthesia or in OR Last resort treatment Requires commitment to self care after surgery and physical therapy treatment after healing Reported success rates 60-95% Vulvodynia Interventions – Systematic Review and Evidence Grading (Obstet Gynecol Surv. 2011 May;66(5):299-315 Insufficient evidence to support any non-surgical therapies for vestibulodynia Single RPCT demonstrate lack of evidence for topical 5% xylocaine, oral desipramine, oral fluconazole, topical cromolyn, topical nifedipine, and botox injections. Fair evidence of benefit of vestibulectomy Placebo effect demonstrated Insufficient direct evidence for efficacy of any intervention for generalized unprovoked vulvodynia Adverse impact on perception of self as a woman Sense of body betrayal Feelings of inadequacy/abnormality Disconnect from genitals due to representation of something negative /painful Relationship discord Other sexual health concerns in both partners (e.g., low sexual desire; erectile dysfunction) Psychiatric impact (e.g., depression; hopelessness; anxiety) Self-protective response to physical pain Body tenses up in anticipation of pain = pain History of negative and/or unhealthy sexual experiences (e.g., trauma) Psychiatric Co-morbidity (e.g., anxiety) Sex as a linear concept (A = B = C) Expectation that all intimacy will lead to sex Muscle tension at “point of no return” Unhealthy relationship dynamics Can I trust he/she will respect boundaries? Goal: Relaxation of pelvic floor muscles with vaginal penetration through use of multiple modalities to restore sexual function Vaginal dilators A gradual approach to being able to receive penetration without pain Anatomy and physiology education Education in exercises for home Biofeedback Trigger point injections Patient and partner education Shifting intimacy dynamics Breaking the association that all intimacy leads to expectation of intercourse Expectation = muscle tension = pain Even once physical components are treated, pain may remain present. Necessity of shifting intimacy dynamics. Ban on intercourse until body is healed Golden opportunity to bolster non-penetrative intimacy Slowly pushing the limits of intimacy Avoiding a 0 to 1000 approach (this does not work) Allowing touch to be a positive experience again Often awkward, “clinical” and painless intercourse occurs prior to spontaneous, pleasurable and painless intercourse Do not trust until experience absence of pain Addressing impact to sense of self as a sexual being Development of a healthy overall sexuality Learning to cope with chronic pain Impacts nearly every aspect of one’s life Treating co-occurring psychiatric concerns (e.g., depression; anxiety) 28 y.o. G1P1001 with localized, burning vulvar pain that is worse with intercourse and tampon insertion. Her diagnosis is most likely A. Generalized vulvodynia B. Recurrent vulvar candidasis C. Provoked Vestibulodynia D. Pudendal nerve entrapment 28 y.o. G1P1001 with localized, burning vulvar pain. Exam reveals vestibular erythema and a positive cotton swab test. You prescribe A. Topical 5% lidocaine B. Pelvic Floor Physical Therapy C. Sexual counseling D. all of the above Recommendations for the treatment of vulvodynia typically include which two (2) of the following: A. Scheduling intercourse B. Slowly increasing non-sexual intimacy C. Increased sexual frequency as a means of de- sensitization D. Initial ban on penetrative sex Stacey Seibel, PhD, LP Stacey.Seibel@ParkNicollet.com Bridget Keller, MD Bridget.Keller@ParkNicollet.com Vulvodynia: An Under-Recognized Pain Disorder Affecting 1 in 4 Women and Adolescent Girls. National Vulvodynia Association. Slides reproduced with permission. Clin Anat. 2013 Jan;26(1):130-3. Vulvar Pain: Anatomic and Recent Pathophysiologic Considerations. J Sex Med. 2012 Sep 13. A Systematic Review of the Utility of Antidepressant Pharmacotherapy in the Treatment of Vulvodynia Pain. Obstet Gynecol Surv. 2011 may;66(5):299-315. Vulvodynia Interventions – Systematic Review and Evidence Grading Acta Obstet Gynecol Scand. 2010 Nov;89(11):1385-95. Surgical Treatment of Vulvar Vestibulitis: a Review. Obstet Gynecol. 2010 Sep;116(3):583-93. Oral Despiramine and Topical Lidocaine for vulvodynia: a Randomized Controlled Trial. Br J Dermatol. 2010 Jun;162(6):1180-5. Guidelines for the Management of Vulvodynia. Obstet Gynecol 2003;102:84-7. Zolnoun DA, Hartmann KE, Steege JF. Overnight 5% Lidocaine Treatment for Vulvar Vestibulitis J Low Genit Tract Dis 2005;9(1):40-51. Haefner, HK, et al. The VulvoDynia Guideline.