File
advertisement

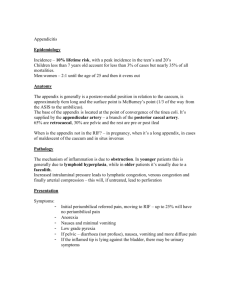
Muhammad Sohaib Shahid (Lecturer & Course Co-ordinator MIT) University Institute of Radiological Sciences & Medical Imaging Technology (UIRSMIT) Abdominal Wall • The abdomen is the region of the trunk that lies between the diaphragm above and the inlet of the pelvis below. • Structure of the Anterior Abdominal Wall The anterior abdominal wall is made up of skin, superficial fascia, deep fascia, muscles, extra peritoneal fascia, and parietal peritoneum. Skin • The skin is loosely attached to the underlying structures except at the umbilicus, where it is tethered to the scar tissue. The natural lines of cleavage in the skin are constant and run downward and forward almost horizontally around the trunk. The umbilicus is a scar representing the site of attachment of the umbilical cord in the fetus; it is situated in the linea alba Clinical Notes • Surgical Incisions If possible, all surgical incisions should be made in the lines of cleavage where the bundles of collagen fibers in the dermis run in parallel rows. An incision along a cleavage line will heal as a narrow scar, whereas one that crosses the lines will heal as wide or heaped-up scars. • Infection of the Umbilicus In the adult, the umbilicus often receives scant attention in the shower and is consequently a common site of infection. Nerve Supply • The cutaneous nerve supply to the anterior abdominal wall is derived from the anterior rami of the lower six thoracic and the first lumbar nerves . • The first lumbar nerve is represented by the iliohypogastric and the ilioinguinal nerves. Dermatomes • The dermatome of T7 is located in the epigastrium over the xiphoid process. • The dermatome of T10 includes the umbilicus • L1 lies just above the inguinal ligament and the symphysis pubis. Blood Supply • Arteries The skin near the midline is supplied by branches of the superior and the inferior epigastric arteries. • The skin of the flanks is supplied by branches of the intercostal, the lumbar, and the deep circumflex iliac arteries . • In addition, the skin in the inguinal region is supplied by the superficial epigastric, the superficial circumflex iliac, and the superficial external pudendal arteries, branches of the femoral artery. Veins The venous drainage passes above mainly into the axillary vein via the lateral thoracic vein and below into the femoral vein via the superficial epigastric and the great saphenous veins Superficial Fascia • The superficial fascia is divided into a superficial fatty layer (fascia of Camper) and a deep membranous layer (Scarpa's fascia) . The fatty layer is continuous with the superficial fat over the rest of the body and may be extremely thick (3 in. [8 cm] or more in obese patients). • The membranous layer is thin and fades out laterally and above where it becomes continuous with the superficial fascia of the back and the thorax, respectively. • Inferiorly, the membranous layer passes onto the front of the thigh, where it fuses with the deep fascia one fingerbreadth below the inguinal ligament. • In the midline inferiorly, the membranous layer of fascia is not attached to the pubis but forms a tubular sheath for the penis (or clitoris). • Below in the perineum, it enters the wall of the scrotum (or labia majora). From there it passes to be attached on each side to the margins of the pubic arch; it is here referred to as Colles' fascia. • In the scrotum, the fatty layer of the superficial fascia is represented as a thin layer of smooth muscle, the dartos muscle. The membranous layer of the superficial fascia persists as a separate layer. • Deep Fascia The deep fascia in the anterior abdominal wall is merely a thin layer of connective tissue covering the muscles; it lies immediately deep to the membranous layer of superficial fascia. Membranous Layer of Superficial Fascia and the Extravasation of Urine • The membranous layer of the superficial fascia is important clinically because beneath it is a potential closed space that does not open into the thigh but is continuous with the superficial perineal pouch via the penis and scrotum. Rupture of the penile urethra may be followed by extravasations of urine into the scrotum, perineum, and penis and then up into the lower part of the anterior abdominal wall deep to the membranous layer of fascia. The urine is excluded from the thigh because of the attachment of the fascia to the fascia lata . • When closing abdominal wounds it is usual for a surgeon to put in a continuous suture uniting the divided membranous layer of superficial fascia. This strengthens the healing wound, prevents stretching of the skin scar, and makes for a more cosmetically acceptable result. Muscles of the Anterior Abdominal Wall • The muscles of the anterior abdominal wall consist of three broad thin sheets that are aponeurotic in front; from exterior to interior they are the : • External oblique, Internal oblique, and Transversus. • On either side of the midline anteriorly is, in addition, a wide vertical muscle, the rectus abdominis . As the aponeuroses of the three sheets pass forward, they enclose the rectus abdominis to form the rectus sheath. • The lower part of the rectus sheath might contain a small muscle called the pyramidalis. External Oblique • The external oblique muscle is a broad, thin, muscular sheet that arises from the outer surfaces of the lower eight ribs and fans out to be inserted into the xiphoid process, the linea alba, the pubic crest, the pubic tubercle, and the anterior half of the iliac crest . • A triangular-shaped defect in the external oblique aponeurosis lies immediately above and medial to the pubic tubercle. This is known as the superficial inguinal ring. The spermatic cord (or round ligament of the uterus) passes through this opening and carries the external spermatic fascia (or the external covering of the round ligament of the uterus) from the margins of the ring. • Between the anterior superior iliac spine and the pubic tubercle, the lower border of the aponeurosis is folded backward on itself, forming the inguinal ligament . • From the medial end of the ligament, the lacunar ligament extends backward and upward to the pectineal line on the superior ramus of the pubis . Its sharp, free crescentic edge forms the medial margin of the femoral ring. • On reaching the pectineal line, the lacunar ligament becomes continuous with a thickening of the periosteum called the pectineal ligament • The lateral part of the posterior edge of the inguinal ligament gives origin to part of the internal oblique and transversus abdominis muscles. To the inferior rounded border of the inguinal ligament is attached the deep fascia of the thigh, the fascia lata. Internal Oblique • The internal oblique muscle is also a broad, thin, muscular sheet that lies deep to the external oblique; most of its fibers run at right angles to those of the external oblique . • It arises from the lumbar fascia, the anterior two thirds of the iliac crest, and the lateral two thirds of the inguinal ligament. The muscle fibers radiate as they pass upward and forward. • The muscle is inserted into the lower borders of the lower three ribs and their costal cartilages, the xiphoid process, the linea alba, and the symphysis pubis. • The internal oblique has a lower free border that arches over the spermatic cord (or round ligament of the uterus) and then descends behind it to be attached to the pubic crest and the pectineal line. Near their insertion, the lowest tendinous fibers are joined by similar fibers from the transversus abdominis to form the conjoint tendon . The conjoint tendon is attached medially to the linea alba, but it has a lateral free border. • As the spermatic cord (or round ligament of the uterus) passes under the lower border of the internal oblique, it carries with it some of the muscle fibers that are called the cremaster muscle . The cremasteric fascia is the term used to describe the cremaster muscle and its fascia. Transversus • The transversus muscle is a thin sheet of muscle that lies deep to the internal oblique, and its fibers run horizontally forward . • It arises from the deep surface of the lower six costal cartilages, the lumbar fascia, the anterior two thirds of the iliac crest, and the lateral third of the inguinal ligament. • It is inserted into the xiphoid process, the linea alba, and the symphysis pubis. The lowest tendinous fibers join similar fibers from the internal oblique to form the conjoint tendon, which is fixed to the pubic crest and the pectineal line . Rectus Abdominis • The rectus abdominis is a long strap muscle that extends along the whole length of the anterior abdominal wall. It is broader above and lies close to the midline, being separated from its fellow by the linea alba. • The rectus abdominis muscle arises by two heads, from the front of the symphysis pubis and from the pubic crest . It is inserted into the fifth, sixth, and seventh costal cartilages and the xiphoid process . • The rectus abdominis muscle is divided into distinct segments by three transverse tendinous intersections: one at the level of the xiphoid process, one at the level of the umbilicus, and one halfway between these two . These intersections are strongly attached to the anterior wall of the rectus sheath . • The rectus abdominis is enclosed between the aponeuroses of the external oblique, internal oblique, and transversus, which form the rectus sheath. • Note that the posterior border of the external oblique muscle is free, whereas the posterior borders of the internal oblique and transversus muscles are attached to the lumbar vertebrae by the lumbar fascia Pyramidalis Muscle • The pyramidalis muscle is often absent. It arises by its base from the anterior surface of the pubis and is inserted into the linea alba . It lies in front of the lower part of the rectus abdominis. Function of the Anterior Abdominal Wall Muscles • The oblique muscles laterally flex and rotate the trunk. The rectus abdominis flexes the trunk and stabilizes the pelvis, and the pyramidalis keeps the linea alba taut during the process. • The muscles of the anterior and lateral abdominal walls assist the diaphragm during inspiration by relaxing as the diaphragm descends so that the abdominal viscera can be accommodated. • The muscles assist in the act of forced expiration that occurs during coughing and sneezing by pulling down the ribs and sternum. Their tone plays an important part in supporting and protecting the abdominal viscera. By contracting simultaneously with the diaphragm, with the glottis of the larynx closed, they increase the intraabdominal pressure and help in micturition, defecation, vomiting, and parturition. Nerve Supply of Anterior Abdominal Wall Muscles • The oblique and transversus abdominis muscles are supplied by the lower six thoracic nerves and the iliohypogastric and ilioinguinal nerves (L1). The rectus muscle is supplied by the lower six thoracic nerves . The pyramidalis is supplied by the 12th thoracic nerve. Inguinal Canal • The inguinal canal is an oblique passage through the lower part of the anterior abdominal wall. • In the males, it allows structures to pass to and from the testis to the abdomen. • In females it allows the round ligament of the uterus to pass from the uterus to the labium majus. • The canal is about 1.5 in. (4 cm) long in the adult and extends from the deep inguinal ring, a hole in the fascia transversalis , downward and medially to the superficial inguinal ring, a hole in the aponeurosis of the external oblique muscle. • It lies parallel to and immediately above the inguinal ligament. In the newborn child, the deep ring lies almost directly posterior to the superficial ring so that the canal is considerably shorter at this age. Later, as the result of growth, the deep ring moves laterally. • The deep inguinal ring, an oval opening in the fascia transversalis, lies about 0.5 in. (1.3 cm) above the inguinal ligament midway between the anterior superior iliac spine and the symphysis pubis . Related to it medially are the inferior epigastric vessels, which pass upward from the external iliac vessels. The margins of the ring give attachment to the internal spermatic fascia (or the internal covering of the round ligament of the uterus). • The superficial inguinal ring is a triangularshaped defect in the aponeurosis of the external oblique muscle and lies immediately above and medial to the pubic tubercle . The margins of the ring, sometimes called the crura, give attachment to the external spermatic fascia. Walls of the Inguinal Canal • Anterior wall: External oblique aponeurosis, reinforced laterally by the origin of the internal oblique from the inguinal ligament . This wall is therefore strongest where it lies opposite the weakest part of the posterior wall, namely, the deep inguinal ring. • Posterior wall: Conjoint tendon medially, fascia transversalis laterally . This wall is therefore strongest where it lies opposite the weakest part of the anterior wall, namely, the superficial inguinal ring. • Roof or superior wall: Arching lowest fibers of the internal oblique and transversus abdominis muscles • Floor or inferior wall: Upturned lower edge of the inguinal ligament and, at its medial end, the lacunar ligament . Function of the Inguinal Canal • The inguinal canal allows structures of the spermatic cord to pass to and from the testis to the abdomen in the male. (Normal spermatogenesis takes place only if the testis leaves the abdominal cavity to enter a cooler environment in the scrotum.) • In the female, the smaller canal permits the passage of the round ligament of the uterus from the uterus to the labium majus. Mechanics of the Inguinal Canal • The inguinal canal in the lower part of the anterior abdominal wall is a site of potential weakness in both sexes. It is interesting to consider how the design of this canal attempts to lessen this weakness. • Except in the newborn infant, the canal is an oblique passage with the weakest areas, namely, the superficial and deep rings, lying some distance apart. • The anterior wall of the canal is reinforced by the fibers of the internal oblique muscle immediately in front of the deep ring. • The posterior wall of the canal is reinforced by the strong conjoint tendon immediately behind the superficial ring. • On coughing and straining, as in micturition, defecation, and parturition, the arching lowest fibers of the internal oblique and transversus abdominis muscles contract, flattening out the arched roof so that it is lowered toward the floor. The roof may actually compress the contents of the canal against the floor so that the canal is virtually closed . • When great straining efforts may be necessary, as in defecation and parturition, the person naturally tends to assume the squatting position; the hip joints are flexed, and the anterior surfaces of the thighs are brought up against the anterior abdominal wall. By this means, the lower part of the anterior abdominal wall is protected by the thighs Spermatic Cord • The spermatic cord is a collection of structures that pass through the inguinal canal to and from the testis . It begins at the deep inguinal ring lateral to the inferior epigastric artery and ends at the testis. • Structures of the Spermatic Cord • The structures are as follows: • Vas deferens • Testicular artery • Testicular veins (pampiniform plexus) • Testicular lymph vessels • Autonomic nerves • Remains of the processus vaginalis • Genital branch of the genitofemoral nerve, which supplies the cremaster muscle Coverings of the Spermatic Cord (the Spermatic Fasciae) • The coverings of the spermatic cord are three concentric layers of fascia derived from the layers of the anterior abdominal wall. Each covering is acquired as the processus vaginalis descends into the scrotum through the layers of the abdominal wall . • External spermatic fascia derived from the external oblique aponeurosis and attached to the margins of the superficial inguinal ring • Cremasteric fascia derived from the internal oblique muscle • Internal spermatic fascia derived from the fascia transversalis and attached to the margins of the deep inguinal ring • Vasectomy • Bilateral vasectomy is a simple operation performed to produce infertility. Under local anesthesia, a small incision is made in the upper part of the scrotal wall, and the vas deferens is divided between ligatures. Spermatozoa may be present in the first few postoperative ejaculations, but that is simply an emptying process. Now only the secretions of the seminal vesicles and prostate constitute the seminal fluid, which can be ejaculated as before. Scrotum • The scrotum is an outpouching of the lower part of the anterior abdominal wall. It contains the testes, the epididymides, and the lower ends of the spermatic cords .The wall of the scrotum has the following layers: • Skin: The skin of the scrotum is thin, wrinkled, and pigmented and forms a single pouch. A slightly raised ridge in the midline indicates the line of fusion of the two lateral labioscrotal swellings. (In the female, the swellings remain separate and form the labia majora.) • Superficial fascia: This is continuous with the fatty and membranous layers of the anterior abdominal wall; the fat is, however, replaced by smooth muscle called the dartos muscle. This is innervated by sympathetic nerve fibers and is responsible for the wrinkling of the overlying skin. The membranous layer of the superficial fascia (often referred to as Colles' fascia) is continuous in front with the membranous layer of the anterior abdominal wall (Scarpa's fascia), and behind it is attached to the perineal body and the posterior edge of the perineal membrane . At the sides it is attached to the ischiopubic rami. Both layers of superficial fascia contribute to a median partition that crosses the scrotum and separates the testes from each other. • Spermatic fasciae: These three layers lie beneath the superficial fascia and are derived from the three layers of the anterior abdominal wall on each side, as previously explained. • The external spermatic fascia is derived from the aponeurosis of the external oblique muscle. • The cremasteric fascia is derived from the internal oblique muscle • The internal spermatic fascia is derived from the fascia transversalis. • The cremaster muscle is supplied by the genital branch of the genitofemoral nerve . The cremaster muscle can be made to contract by stroking the skin on the medial aspect of the thigh. This is called the Cremasteric reflex. • The function of the cremaster muscle is to raise the testis and the scrotum upward for warmth and for protection against injury. For testicular temperature and fertility. Structure of the Posterior Abdominal Wall • The posterior abdominal wall is formed in the midline by the five lumbar vertebrae and their intervertebral discs and laterally by the 12th ribs, the upper part of the bony pelvis , the psoas muscles, the quadratus lumborum muscles, and the aponeuroses of origin of the transversus abdominis muscles. The iliacus muscles lie in the upper part of the bony pelvis. • Lumbar Vertebrae • The body of each vertebra is massive and kidney shaped, and it has to bear the greater part of the body weight. The fifth lumbar vertebra articulates with the base of the sacrum at the lumbosacral joint. • The intervertebral discs in the lumbar region are thicker than in other regions of the vertebral column. They are wedge shaped and are responsible for the normal posterior concavity in the curvature of the vertebral column in the lumbar region (lordosis). For a full description of the structure of the lumbar vertebrae and the intervertebral discs. • Twelfth Pair of Ribs It should be noted that the head of the 12th rib has a single facet for articulation with the body of the 12th thoracic vertebra. The anterior end is pointed and has a small costal cartilage, which is embedded in the musculature of the anterior abdominal wall. In many people it is so short that it fails to protrude beyond the lateral border of the erector spinae muscle on the back. Muscles of the Posterior Abdominal Wall • Psoas Major • The Psoas muscle arises from the roots of the transverse processes, the sides of the vertebral bodies, and the intervertebral discs, from the 12th thoracic to the 5th lumbar vertebrae . The fibers run downward and laterally and leave the abdomen to enter the thigh by passing behind the inguinal ligament. The muscle is inserted into the lesser trochanter of the femur. The psoas is enclosed in a fibrous sheath that is derived from the lumbar fascia. The sheath is thickened above to form the medial arcuate ligament. • Nerve supply: This muscle is supplied by the lumbar plexus. • Action: The psoas flexes the thigh at the hip joint on the trunk, or if the thigh is fixed, it flexes the trunk on the thigh, as in sitting up from a lying position. Quadratus Lumborum • The quadratus lumborum is a flat, quadrilateral-shaped muscle that lies alongside the vertebral column. It arises below from the iliolumbar ligament, the adjoining part of the iliac crest, and the tips of the transverse processes of the lower lumbar vertebrae . The fibers run upward and medially and are inserted into the lower border of the 12th rib and the transverse processes of the upper four lumbar vertebrae. The anterior surface of the muscle is covered by lumbar fascia, which is thickened above to form the lateral arcuate ligament and below to form the iliolumbar ligament. • Nerve supply: This muscle is supplied by the lumbar plexus. • Action: It fixes or depresses the 12th rib during respiration and laterally flexes the vertebral column to the same side. • Iliacus • The Iliacus muscle is fan shaped and arises from the upper part of the iliac fossa. Its fibers join the lateral side of the psoas tendon to be inserted into the lesser trochanter of the femur. The combined muscles are often referred to as the iliopsoas. • Nerve supply: This muscle is supplied by the femoral nerve, a branch of the lumbar plexus. • Action: The iliopsoas flexes the thigh on the trunk at the hip joint, or if the thigh is fixed, it flexes the trunk on the thigh. Peritoneal Lining of the Abdominal Walls • The walls of the abdomen are lined with parietal peritoneum. This is a thin serous membrane consisting of a layer of mesothelium resting on connective tissue. It is continuous below with the parietal peritoneum lining the pelvis • Nerve Supply • The central part of the diaphragmatic peritoneum is supplied by the phrenic nerves, and the peripheral part is supplied by the lower intercostal nerves. The peritoneum lining the anterior and posterior abdominal walls is supplied segmentally by intercostal and lumbar nerves, which also supply the overlying muscles and skin. Paracentesis of the Abdomen • Paracentesis of the abdomen may be necessary to withdraw excessive collections of peritoneal fluid, as in ascites secondary to cirrhosis of the liver or malignant ascites secondary to advanced ovarian cancer. Under a local anesthetic, a needle or catheter is inserted through the anterior abdominal wall. The underlying coils of intestine are not damaged because they are mobile and are pushed away by the cannula. McBurney's Incision • This is chiefly used for cecostomy and appendectomy. It gives a limited exposure only, and should any doubt arise about the diagnosis, an infraumbilical right paramedian incision should be used instead. • An oblique skin incision is made in the right iliac region about 2 in. (5 cm) above and medial to the anterior superior iliac spine. The external and internal oblique and transversus muscles are incised or split in the line of their fibers and retracted to expose the fascia transversalis and the peritoneum. The latter are now incised and the abdominal cavity is opened. The incision is closed in layers, with no postoperative weakness. Abdominal Herniae • A hernia is the protrusion of part of the abdominal contents beyond the normal confines of the abdominal wall . • It consists of three parts: • the sac, the contents of the sac, and the coverings of the sac. • The hernial sac is a pouch (diverticulum) of peritoneum and has a neck and a body. • The hernial contents may consist of any structure found within the abdominal cavity and may vary from a small piece of omentum to a large viscus such as the kidney. • The hernial coverings are formed from the layers of the abdominal wall through which the hernial sac passes. Femoral Hernia • The hernial sac descends through the femoral canal within the femoral sheath, creating a femoral hernia. The femoral sheath, is a protrusion of the fascial envelope lining the abdominal walls and surrounds the femoral vessels and lymphatics for about 1 in. (2.5 cm) below the inguinal ligament . • The femoral artery, as it enters the thigh below the inguinal ligament, occupies the lateral compartment of the sheath. The femoral vein, which lies on its medial side and is separated from it by a fibrous septum, occupies the intermediate compartment. The lymph vessels, which are separated from the vein by a fibrous septum, occupy the most medial compartment. • A femoral hernia is more common in women than in men (possibly because of a wider pelvis and femoral canal) Umbilical Herniae • Congenital umbilical hernia, or exomphalos (omphalocele), is caused by a failure of part of the midgut to return to the abdominal cavity from the extraembryonic coelom during fetal life. The hernial sac and its relationship to the umbilical cord . • Acquired infantile umbilical hernia is a small hernia that sometimes occurs in children and is caused by a weakness in the scar of the umbilicus in the linea alba . Most become smaller and disappear without treatment as the abdominal cavity enlarges. • Acquired umbilical hernia of adults is more correctly referred to as a paraumbilical hernia. The hernial sac does not protrude through the umbilical scar, but through the linea alba in the region of the umbilicus . Paraumbilical herniae gradually increase in size and hang downward. The neck of the sac may be narrow, but the body of the sac often contains coils of small and large intestine and omentum. Paraumbilical herniae are much more common in women than in men. Lumbar Hernia • The lumbar hernia occurs through the lumbar triangle and is rare. The lumbar triangle (Petit's triangle) is a weak area in the posterior part of the abdominal wall. It is bounded anteriorly by the posterior margin of the external oblique muscle, posteriorly by the anterior border of the latissimus dorsi muscle, and inferiorly by the iliac crest. The floor of the triangle is formed by the internal oblique and the transversus abdominis muscles. The neck of the hernia is usually large, and the incidence of strangulation low Lumbar Triangle Inguinal Hernia