01 Greenough-Psy400INTRO 2007
advertisement

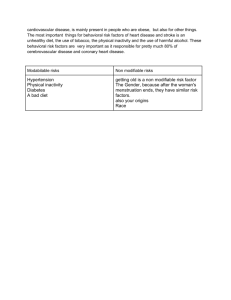
Behavioral Sciences Faculty: William Greenough: Course Director Brian Ross, Psychology Michael Wilson, Visiting Professor Donna Korol, Psychology, Medicine Karl Rosengren, Psychology, Kinesiology Joe Goldberg, College of Medicine Robert Rich, College of Law Carol Packard, College of Medicine Aaron Grossman, Teaching Assistant Bill Greenough, Professor of Psychology, Psychiatry and Cell and Structural Biology Wgreenou@uiuc.edu Office Hour: 11-12 Tu or by appt. Office 2347 Beckman Institute Phone: 333-4472 (for appts.) The Behavioral Sciences course is taught in synchrony with the Neuroscience course to minimize overlap and cover areas from complementary perspectives. Course Objectives: Bases •Many of the greatest health risk factors today are behavioral, the realm of Behavioral Science •Self-injurious behaviors such as smoking, alcohol and drug abuse, poor dietary and exercise habits, now constitute the largest controllable risk factors for mortality •Psychiatric disorders: major cause of disability •Behavior can put others at risk (e.g., ARND) •Physician’s responsibility is to inform and advise patients at risk or putting others at risk Course Objectives: Bases •Other behavioral issues important in Medicine •Stress is a serious medical issue (CardioVascD) • Compliance (taking medicine, following medical advice, regular preventative medicine) • Sexual function (taking a sexual history) • Is my child “normal”? Development and Aging • Stress-related or affected disorders • Lifestyle (Tobacco, Diet, Exercise, Alcohol, Sleep) Objectives for this lecture • Be aware of changing causes of mortality and medical costs in 21st century • Understand Biomedical vs. Biopsychosocial models of illness and health maintenance • Recognize importance of behavioral sciences to modern medical practice • Understand example of stress and coronary heart disease • Understand course objectives Dramatic changes have occurred across the past century in causes and ages of death. Infectious disease has become largely controlled, and hence people are living longer and dying from different causes Source: U. S. Senate Sub-Committee on Aging, OASDI, 2003 *Infectious Disease * ** * *Lifestyle * * * * * Life Expectancy, 1900 = 54.3; 1996 = 81.5 (Sweden) Source: S. E. Taylor, Health Psychology (5th Edition), Mc Graw-Hill, 2003 Is Smoking on the Decline? Not over the last decade (Source CDC, 2003; Behavioral Risk Factor Surveillance System) Current Smokers* Nationwide Year: Median % 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 23.0 23.1 22.2 22.6 22.7 22.4 23.4 23.2 22.9 22.6 23.2 22.8 States include District of Columbia and Puerto Rico in applicable years *All respondents 18 and older who have ever smoked 100 cigarettes in their lifetime and reported smoking every day or some days. Alcohol Use: Chronic Drinking* Nationwide (CDC, 2003) Year: Median % 1990 3.2 1991 3.4 1992 3.0 1993 3.0 1994** No Data 1995 2.8 1996** No Data 1997 3.0 1998** No Data 1999 3.6 2000** No Data 2001 5.1 States include District of Columbia and Puerto Rico in applicable years *All respondents 18 and older who report an average of two or more drinks per day i.e., 60 or more alcoholic drinks a month. Denominator includes all survey respondents except those with missing, don't know, and refused answers. Obesity: By Body Mass Index* Nationwide Year: Median % 1990 11.6 1991 12.6 1992 12.6 1993 13.7 1994 14.4 1995 15.8 1996 16.8 1997 16.6 1998 18.3 1999 19.7 2000 20.1 2001 21.0 States includes District of Columbia and Puerto Rico in applicable years *All respondents 18 and older who report that their Body Mass Index (BMI) is 30.0 or more. BMI is defined as weight in kilograms divided by height in meters squared (w/h**2). Denominator includes all survey respondents except those with missing, don't know, and refused answers. (Source CDC, 2003) Look again at the diseases that are increasing: Source: S. E. Taylor, Health Psychology (5th Edition), Mc Graw-Hill, 2003 Risk Factors for Leading Causes of Death in US • Heart Disease: Tobacco, Obesity, Blood Pressure, Cholesterol (Diet), Exercise • Cancer: Tobacco, Improper Diet, Alcohol, Environmental Exposure • Stroke: Tobacco, Blood Pressure, Cholesterol, Exercise • Accidents: Seat Belts, Alcohol, Home Hazards • Chronic Lung Disease: Tobacco, Environment Source: M. McGinnis (1994). The role of behavioral research in National Health Policy, in S. Blumenthal et al. New Frontiers in Behavioral Medicine: Proceedings of the National Conference. NIH Publications. Cost of Treatment for Selected Preventable Conditions • Heart Disease: Coronary Bypass surgery, $30,000 • Cancer: Lung Cancer Treatment, $29,000 • Injuries: Quadriplegia (lifetime), $600,000 • Total Annual US Cost of Alcohol Abuse: $148,021,000,000* Source: M. McGinnis (1994). The role of behavioral research in National Health Policy, in S. Blumenthal et al. New Frontiers in Behavioral Medicine: Proceedings of the National Conference. NIH Publications. *Source:THE ECONOMIC COSTS OF ALCOHOL AND DRUG ABUSE IN THE UNITED STATES, 1992. H. Harwood, D. Fountain, and G. Livermore. Analysis by the Lewin Group. Rockville, MD: DHHS, NIH, NIDA, OSPC, NIAAA, OPA. Biomedical Model • • • • Illnesses arise from somatic causes Biochemical-Physiological bases Psychiatric: Neurophysiological bases Psychological and social processes largely independent of disease processes Biopsychosocial Model • Emphasizes health maintenance over disease • Biological, Psychological and Social Factors are all important determinants of health • Health maintenance requires addressing issues at all of these levels As a Physician, your Job is to Optimize Health Go Where the Problems Are Arguably, if saving (or extending) lives is your principal goal, Behavioral Science is the most important pre-clinical course you will take Course Objectives: Basis • Knowledge of human behavior is a critical tool of the physician. • Behavior is a product of the biology of the individual--physician or patient • Behavior is not only your primary source of information about your patients, it is also a primary tool for restoring or improving their health Course Objectives • To understand behavior and its origins in the brain • To understand relationships of behavior to health and disease • To begin to understand psychiatric disorders and their treatment • To understand basic issues of human behavior • To know about development across the lifespan: Adulthood and aging are part of the development process Course Objectives • To appreciate the differences between human and veterinary medicine. • Mammalian physiology is very similar in animals and humans (but not the same in all cases). • What differs most is the capacity of the brain, which makes humans human. Physicians have to recognize this. • To prepare for the Behavioral Science component of Step I of the Boards (United States Medical Licensure Examination)! Why is there so much to learn in medical school? The number of hours in the basic sciences curriculum has not changed appreciably since 1953. The amount of relevant basic science has changed Sociobehavioral Aspects of Cardiovascular Disease (CVD): A Case Study • Long history of interest in relationships of behavior, stress and susceptibility to CVD, Coronary Heart Disease (CHD) • CHD: Myocardical Infarction (MI) [heart attack], pre-clinical signs (arterial plaque, angina [chest pain]) • “ Type A” coronary prone behavior pattern (Friedman & Rosenman) Source: KA Matthews, Psychological perspectives on the development of coronary heart disease, American Psychologist, 60: 783-796, 2005 Coronary Heart Disease • Atherosclerosis: Dynamic and progressive disease; Signs may be present in 20s or 30s • Arterial endothelial dysfunction and inflammation • Initial endothelial damage by oxidized low-density lipoprotein cholesterol, smoking, high blood pressure • Inflammatory response: Intimal layer thickening: monocytes => macrophages • Plaque (lipid and tissue accumulation) closes off artery; rupture => thrombosis Atherosclerosis • Progressive disorder • Non-invasive assessment: Ultrasound scanning (corotid artery intima media thickness), electron beam tomography to assess aortic and coronory calcification • Test for atherosclerosis-related lipoproteins Source: KA Matthews, Psychological perspectives on the development of coronary heart disease, American Psychologist, 60: 783-796, 2005 Risk Factors for CHD: Most Involve Behavioral Management • • • • • • • • High blood pressure (physical exercise can reduce) High cholesterol Central adiposity (distribution: waist circumference) Obesity (exercise, diet) Smoking Sedentary Diabetic Low Socioeconomic background Psychosocial Predictors of Coronary Events • Stressful Environments – Jobs • High effort; low reward • Low decision-making latitude – Primary relationships • Marital distress, dissatisfaction (divorce during study) • Poor communication • Personal Characteristics Psychosocial Predictors of Coronary or Atherosclerotic Events • Stressful Environments • Personal Characteristics – Hostility • Angry affect, mistrustful attitudes towards others, and antagonistic behavior – Depression and anxiety – Major depression and anxiety disorders Who Gets CHD? • These are not just idle speculations but collective findings of many (>20) large scale prospective studies with data collection “blind” to subject characteristics during the study • Criteria included both incidence of CHD and subclinical atherosclerosis measures • Direction of associations can be uncertain, e.g., does stress lead or contribute to hostility and/or anxiety and depression? Speculations on Mechanisms • Stress-associated hormones (e.g., glucocorticoids) (McEwen, Sapolsky) • Cytokines (signaling compounds released by inflamed or damaged tissue acting via receptors) • Irritative effects of risk behavior elements (e.g., tobacco compounds, excess alcohol) Take home points • Behavior and lifestyle characteristics clearly affect susceptibility to cardiovascular disease • There is evidence for mechanisms mediating these phenomena at system, cellular and molecular levels • Psychosocial variables can have critical physiological and medical consequences beyond the realm of mental health Aaron Grossman Teaching Assistant • Medical Scholars Program (MD-PhD, Neuroscience) • PhD Thesis Completed: “Synaptic Plasticity in the Cerebral Cortex of Fragile X Knockout Mice” • USMLE (Boards) Step 1 Completed