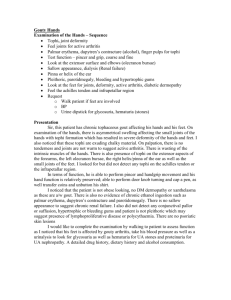
approach to monoarthritis
advertisement

APPROACH TO MONOARTHRITIS DR CB NEL “Inflammation of a single joint” • Acute • Chronic WHERE IS THE INFLAMMATION? • ARTICULAR • pain all planes • • • • PERI-ARTICULAR pain in plane of tendon active = passive active > passive capsular swelling/effusion linear swelling joint line tenderness localised tenderness diffuse erythema/heat localised erythema/heat ACUTE MONOARTHRITIS Septic arthritis Crystal synovitis Trauma Haemarthrosis Foreign body reaction Monoarticular presentation of oligo- / polyarthritis o RA o Erythema nodosum o Juvenile idiopathic arthritis o Reactive, Psoriatic or other Seronegative spondiloarthropathy CHRONIC MONOARTHRITS Foreign body Infection-Tuberculosis Ch. Sarcoidosis Enteropathic Arthritis (mainly Crohn’s) Amyloidosis Pigmented villonodular synovitis Synovial pathology (sarcoma, chondromatosis) Monoarticular presentation of oligo- / poly articular disease CRYSTRAL ARTHROPATHIES Crystal-induced Arthritis • Gout (monosodium urate crystals) most common - First MTP, ankle, midfoot, knee (can be any joint though) - Most initial attacks affect a single joint - Fever (more common with polyarticular) can raise suspicion for infection - Presence of crystal does not exclude infection - May see desquamation of overlying skin - Thiazide diuretics can put at risk - Needle shaped, negatively birefringent crystals • Calcium pyrophosphate dihydrate/pseudogout - Clinically not able to distinguish from gout - Most common in knee and wrists - Evolves over several days (less acute than gout) - Rhomboid shaped, positively birefringent crystals • Other crystals: apatite, calcium oxalate, liquid lipid GOUT URIC ACID POOL Endogenous Exogenous Excretion Kidneys (2/3) Intestines (1/3) Serum urate: 0,12 - 0,55mmol/l Urine urate excretion: 1,5 - 4,4mmol/24 hours MECHANISM OF HYPERURICAEMIA • Underexcretion (Most common) • Overproduction HYPERURICAEMIA AND GOUT • Disorder of purine metabolism • Characterised – hyperuricaemia – deposition of uric acid or urate crystals in the tissues • Manifestations – – – – acute attacks of gouty arthritis tophi kidney stones urate-nephropathy PATHOGENESIS • Hyperuricaemia causes gout, but is not synonomous with gout • Factors promoting crystallisation (0.55mmol/l) – the level of saturation – solubility – pH and temperature of the limb(colder areas) PATHOGENESIS Crystallisation in joint Crystal absorbed by PMN Secretion lysozyme enzymes Severe synovitis ACUTE GOUTY ARTHRITIS • INCIDENCE – Mostly men > 40yrs – Association with Metabolic syndrome – Sometimes postmenopausal women (Often on Diuretics) PRECIPITATING CAUSES IN ACUTE GOUTY ARTHRITIS • Trauma and surgery • Medication • Alcohol • Diet CLINIAL PICTURE ACUTE GOUTY ARTHRITIS • Goes to bed healthy • Wakes up sudden monoarthritis ( 85% Podagra) (heel, instep, knee, wrist and hands and elbow -olecranon bursitis) • Rigors with severe pain • Night spent in torture • Joint is red (“ripe tomato”),warm and very tender. • After attack skin around the joint often peels off • Acute attacks usually pass completely until the next attack Uncontrolled hyperuricaemia may lead to polyarticular gout ACUTE GOUTY ARTHRITIS DIAGNOSIS OF GOUT • Family history, as well as a typical history of attacks • Typical clinical picture and tophi • Elevated serum urate - (may be normal during attacks) • Urate crystals in aspiration fluid (as well as tophi) • X rays: Punched-out erosions (Rat bitten) URATE CRYSTALS TREATMENT • • • • Exclude precipitating causes Increased water intake 2-3l/day A low purine diet and avoidance of alcohol are recommended Foods with a very high purine content: anchovy, sardines, liver and kidneys. Most meats, fish and chicken products also have a high purine content. • Treatment of associated conditions such as – – – – – obesity Hypertension Diabetes mellitus hyperlipaemia kidney failure RX ACUTE ATTACK • Avoid prescribing prophylactics (uric acid lowering drugs) • NSAIDS ( not used in kidney failure) • Colchicine • Corticosteroids (in resistant cases) Progression in the disease • Asymptomatic hyperuricaemia – continues until possible first attack • Acute gouty arthritis • Interval hyperuricaemia – periods between attcks • Chronic tophaceous gout • Complications – kidney stones and nephropathy CHRONIC TOPHACEOUS GOUT • Deposition of uric acid crystals in the tissues (tophi) • After repeated attacks after 11 - 12 years • The tophi occur in – – – – The auricles - helix Tendons (hands, achilles tendon and feet) Bursae - especially olecranon bursa The tophi may ulcerate with secretion of pasty material INDICATIONS FOR LONG-TERM PROPHYLACTIC THERAPY If conservative measures do not have the desired effect and the levels still remain high (> 0.55 - 0.6 mmol/l) with repeated attacks (If less than 1 attack per year is experienced, treatment is not necessary) Positive family history of gout and kidney stones with very high urate levels Chronic tophaceous gout Kidney stones or nephropathy MEDICINES FOR LONG-TERM PROPHYLAXIS • Allopurinol 300mg-900mg/day • Uricosurics medicines – Probenecid 250mg bd – Must not be used if there is kidney failure or kidney stones – To avoid kidney stones a high fluid intake (2l/day) must be maintained and in addition the urine can be alkalised with something like “citrosoda” • Colchicine 0.5mg should be added once or twice daily for the first few months in order to prevent recurrent attacks SEPTIC ARTHRITIS CAUSES Bacterial Gonococcal Non-gonococcal(Staphylococcus aureus , nongroup-A beta-hemolytic streptococci, gram-negative bacteria, and Streptococcus pneumoniae) Viral – HBV, Rubella, Mumps, I.M, Parvovirus, Enterovirus, Adenovirus Fungal CAUSES • Most serious cause of monoarthritis, can destroy cartilage in one to two days • Non-gonococcal are most serious - most common in knees and hips - sternoclavicular joints in IV drug users - most febrile but do not appear especially ill - 90% monoarticular, hematogenous spread - 80% Gram(+) anaerobes * 60% S. Aureus (most PCN, some meth resistant) * 15% Non-group A, beta-hemolytic strep * 3% Strep pneumo - 18% Gram(-) - Anearobes on rise in IV drug users/immunocompromised/HIV • • • • common organisms Staphylococci or Streptococcus young adults, significant incidence gonococcal arthritis Elderly & immunocompromised gram -ve organisms Anaerobes more common with penetrating trauma ROUTES OF INFECTION Risk factors • Pre-existing joint disease • Prosthetic joints • Low SE status, IV drug abuse, alcoholism • Diabetes, steroids, immunosuppression/HIV • Previous intra-articular steroid injection DIAGNOSIS • Synovial fluid aspiration – Volume/viscosity/cellularity/a ppearance – Gram stain/culture – Absence of organism does not exclude septic arthritis – Polarised light microscopy (crystals). Crystals don’t exclude septic arthritis. – NB suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics DIAGNOSIS • Always blood cultures • Significant proportion blood cultures + ve in absence of + ve synovial fluid cultures • FBC ESR & CRP • BUT absence of raised WBC, ESR or CRP not exclude diagnosis of sepsis - if clinical suspicion high always treat Antibiotic treatment of septic arthritis • Local and national guidelines • Liaise with micro. guided by gram stain • Don’t wait for cultures to start empiric antibiotic treatment • Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks Joint drainage & surgical options • Medical aspiration, surgical aspiration via arthroscopy or open arthrotomy • Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement QUESTIONS?