Identification and Management of Children at Risk
advertisement

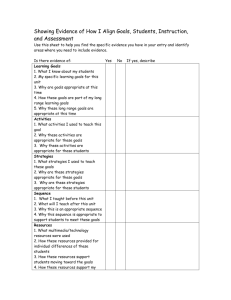
Identification & Management of Children at Risk Presented by: Dr. Nanolla Yazdani, School Psychologist A. Goal B. Understanding of emotionally disturbed child C. Identification of Emotional Disability D. Management of emotionally disturbed child E. Treatment December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 2 In-depth understanding, identifying, and managing, Children with Emotional Disabilities December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 3 1. Reports from Bazelon Center for Mental Health, Washington DC. 2. Comparison of identification rate, IDEA, 2004 December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 4 • Students with mental and emotional disorders have been cited as among the most under-identified and underserved students with a disability. • Lack of resources and concern about costs that the district might incur, lack of access to mental health services for identified children, stigma concerning the label of emotional disturbance and desire to remove troublesome children perceived as not having a “real disability” may all contribute to overall low identification rates for children with mental and emotional disorders. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 5 • Effective prevention of school failure depends crucially on early recognition and provision of services for troubled children. Delaying identification results in children requiring more intensive IDEA services once they are identified. • State education agencies and local schools should collaborate with mental health agencies to design coordinated systems of care that use resources from both systems to meet the comprehensive needs of children with mental and emotional disorders, including those identified as emotionally disturbed under IDEA. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 6 • National IDEA identification of children with emotional disturbance - 0.74% • National IDEA identification of children with other health impairments - 0.4% • U.S. Surgeon General's identification of children with mental disorder + extreme functional impairment 5% • U.S. Surgeon General's identification of children with mental disorder + significant functional impairment 11% • Highest state rate (Minnesota, Vermont) - 1.92% • Lowest state rate (Arkansas) - 0.10% December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 7 1. State Policies Regarding Individuals with Disabilities Education Act Amendments of 2004 (what is EmD?) 2. Pattern that can serve as a cue December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 8 “A condition exhibiting one or more of the following characteristics over a long period of time and to marked degree that adversely affects a child’s educational performance.” December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 9 • An inability to learn that cannot be explained by intellectual, sensory, or health factors • An inability to build or maintain satisfactory interpersonal relationships with peers or teachers • Inappropriate types of behavior or feelings under normal circumstances • A general pervasive mood of unhappiness or depression and/or • A tendency to develop physical symptoms or fear associated with personal or school problems IDEA, 2004 December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 10 Emotional disturbance includes schizophrenia. The term does not apply to children who are socially maladjusted, unless it is determined that they have an emotional disturbance. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 11 DSM-IV-TR: Mental disorder is conceptualized as clinically significant behaviors or psychological syndromes or patterns that occur in an individual and are associated with present distress, disability or with significantly increased risk of suffering death, pain, disability, or important loss of freedom. (Diagnostic and Statistical Manual for Mental Disorders, 2000) December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 12 • Withdrawal, avoidant, insecure behaviors, selfconscious • Anxiety, excessive worries, preoccupation • Excessive motor movement • Problem with relationship • Attention-problems, poor comprehension • Lack of empathy, manipulation • Attention seeking behaviors • Perception of reality • Rituals, obsessivecompulsive December 2012 • Problems with authority figures • Persistent complaint of being ill • Blaming others • Regressive and acts like younger child • Self-distractive, risk-taking behaviors • Depressive mood, lack of interest or pleasure, irritability • Physical change (weight, grooming, sleep, interaction, appetite) Office of Instructional Enhancement and Internal Operations/Office of Special Education 13 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. Preoccupation with details of certain thoughts Hopelessness Poor coping mechanism to stressors Impulsivity Unrealistic sense of power Deceitfulness/bullying Difficulties with relationships Anxiety and aggression/Poor resistance to anger impulse Pattern of disruptive behaviors Possible delusion or hallucination Aggressiveness expressed is grossly out of proportion Suicidal or homicidal ideation Deliberate engagement with distraction of properties December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 14 What is the most popular unacceptable and dangerous symptom in American Schools? December 2012 Different Forms of VIOLENCE Office of Instructional Enhancement and Internal Operations/Office of Special Education 15 1. Mood Disorders 2. Substance-Related Disorders 3. Personality Disorders 4. Adjustment Disorders; Disruptive Behavior Disorder 5. Impulse Control Disorders 6. Schizophrenia or other Psychotic Disorders 7. ADHD, CD,ODD; Educational Problems 8. Sexual and Gender Identity Disorders December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 16 • • • • Retention Absences Summer school Change in schools, number of schools • Suspensions • Bus suspensions • Leaving school early, attending partial day December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 17 • Syndrome vs. Symptom (establishing diagnosis) • Diagnostic Criteria • Provisional Approach • Behavioral Problems vs. Pathological Symptoms December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 18 December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 19 1. Functional Behavioral Assessment (FBA)/Identification 2. Planning 3. Intervention 4. Referral December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 20 • Behavioral Problems (may have a symptom) • Pathological symptoms (criteria for clinical impression has met) • Impact on learning (mild, moderate, and severe) December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 21 1. Implementation of Functional Behavioral Assessment (FBA). This problem-solving process identifies the student’s problem behavior and its function. 2. Teacher, counselor and school psychologist, collaboratively identify, isolate, and assess the impact of the problem behavior on the student’s learning process. 3. The school psychologist or counselor identifies underlying causes and functions of problem behavior. 4. Problem behavior will be analyzed based on its function, location, frequency, duration, and intensity (degree of its impact on the learning process). December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 22 • Management plan (intervention) will be drawn based on FBA. • Management plan (intervention) will be utilized in Tier 1 and Tier 2. • Progress of management plan (intervention) will be monitored. • Individual and group therapy will be conducted to facilitate Tier 1 and Tier 2. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 23 • Clinical Interview will be conducted with child, teacher, counselor, and parent. • Formal Assessment (Behavioral and Emotional Rating Scale 2nd Edition) will be administered to draw initial phase for establishment of base line for problem behavior. • The Problem Documentation will be provided to complete the final phase of base line establishment. • Develop the FBA and communicate with the team members. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 24 Problem Documentation: Describe the problem Behavior(s) in each location below. Frequency: Indicate the frequency of the problem behavior. Hourly/daily/weekl y Duration: How long Impact on Learning: List below 1. High Impact (Disruptive or dangerous) 2.Moderate (disrupts own learning process) 3. Mild (annoying) School: Indicate source Home: Indicate source Community: Indicate source December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 25 Testing!!!!!!!!!!!!!!!!!!!!! What is missing? December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 26 Problem Behavior Concrete definition Carlos is aggressive. Report by teacher He hits other students during recess when he doesn’t get his way. Trish is disruptive. Report by teacher She makes irrelevant and inappropriate comments during class session. John is hyperactive. Report by teacher and mother 1.He completes only small portion of his work at home. 2.He blurts out answers in the class. 3.He leaves his assigned seat. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 27 1. Frequency 2. Duration 3. Intensity (Educational Impact) December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 28 • Intervention should be research based. • Intervention should be based on Bio-Psycho-SocialEnvironmental Mode. • Intervention should deal with the function and the cause of behavior. • The modified behavior should be overt, measurable, and objective. • Intervention should rectify skill deficit, desire deficit, and performance deficit problems. • Interventions should deal with the problem behavior. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 29 A graphical display of baseline and intervention modalities should be available in the student’s file. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 30 In TST process, if Tier 1, Tier 2, and Tier 3 did not rectify the problem behavior(s), the student should be referred for initial evaluation for EmD. December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 31 • Treatment should be viewed in a systemic fashion that involves prevention and intervention. • Treatment should be multifaceted and comprehensive. • Intervention and prevention should be planned by a team (educators, parents, children, and counselors). December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 32 Questions and Discussions Thanks for being here December 2012 Office of Instructional Enhancement and Internal Operations/Office of Special Education 33