The QIRC Trial - Department of Mathematics and Statistics
advertisement

Power Considerations in the
“Quality Initiative in Rectal
Cancer” Trial Design
by Eddy Rempel
May 13, 2005
SOSGSSD 2005
Presentation Outline
• Research on TME
• QIRC Trial
• Factors impacting power
• Sample Size Calculations
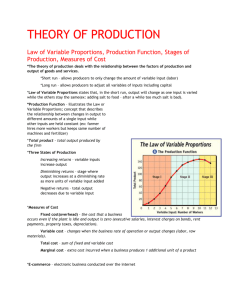
Motivation for Total Mesorectal
Excision (TME) Research
• Refinement of rectal cancer surgery
• Removal of lymph node bearing tissue
• Retains autonomic nerves
• preserving bowel, bladder, and sexual function
• Reduces need for radiation and chemotherapy
• Great patient outcomes in Europe
• 5000 rectal cancers diagnosed in Ontario per year
Rectal Cancer Patient Back View
TME – Total Mesorectal Excision x-ray
Parietal Fascia
Visceral Fascia
Seminal
Vesicles
TME Recurrence Rates in Europe:
TME versus Conventional Surgery
TME
England
Netherlands
Sweden
5%
4.1%
11%
Surgery +
Chemo +
Radiation
13.5%
11.5%
27%
• MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision for rectal cancer. Lancet 1993;
341(8843):457-460.
• SRCT. N Engl J Med 1997; 336(14):980-7.
• Kapiteijn E, et al. Preoperative radiotherapy combined with total mesorectal excision for
resectable rectal cancer. N Engl J Med 2001; 345(9): 638-46.
Outcome Measures for Radiation
Groups in English Hospital
Radiation No Radiation
Basingstoke Medical Centre
(N=35)
(N=115)
Number of local recurrences
17.1%
2.6%
Permanent colostomy
17.1%
6.1%
Simonovic M, Sexton R, Rempel E, Moran BJ, Heald BJ. Optimal preoperative
assessment and surgery for rectal cancer may greatly limit the need for radiotherapy.
British Journal of Surgery (August 2003) Volume: 90 , Issue: 8 , Date: August 2003
TME Pilot Study
at Three Hospitals in Ontario
Cases
PreIntervention
PostIntervention
Full Intervention
Cases
87
48
39
Colostomies
15
11
4
22.9%
10.3%
Rate
Partial Intervention
Cases
33
12
21
Colostomies
11
4
7
33.3%
33.3%
Rate
The QIRC Trial
•
CIHR funding – October 2001
•
Randomized Control Trial
•
Experimental arm surgeons trained in TME by workshop,
operative demonstrations, post operative questionnaires
•
Control arm surgeons learn as usual – no limitation on
learning and practicing new techniques including TME
•
Primary outcomes – rates of permanent colostomy, local
recurrence, long-term survival
QIRC Trial Randomization
• Clustered design – Patients within Hospitals
• Hospitals randomized to experimental or control arm
• Surgeons in experimental arm hospitals trained in TME
• No training of control arm surgeons
• Consecutive patients – no randomization of patients
• Clinically relevant difference from experimental to control
arm outcome proportions
Approximating Binomial with
Normal Distribution
• CLT the binomial approaches the normal
asymptotically
• Good approximation when
p+/- (p(1-p) / n)½ in (0,1)
• Even small n is close to normal
•e.g. p=.3 requires only n=10 and p=.08 requires n=46.
Mendenhall W, Wackerly D, Scheaffer RL. Mathematical Statistics with Applications, 4th
ed. p. 326, PWS-KENT Publishing Company, 1990.
Approximating Binomial with
Normal Distribution
Normal Approximation of the Binomial Distribution
Normal Approximation of the Binomial Distribution
Binomial
Normal
Binomial
Normal
Binomial
Normal
pdf/pmf
pdf/pmf
46
0.08
n
p
168
0.08
5
0.10
0.2
0.0
0
0.05
0.1
0.0
pdf/pmf
15
n
p
10
4
0.5
0.15
0.3
n
p
0.20
0.4
Normal Approximation of the Binomial Distribution
0
1
2
X
3
4
0.0
0
10
20
30
40
X
p+/- (p(1-p) / n)½ in (0,1)
0.2
0.4
0.6
p
0.8
1.0
Hypothesis Test
Test that there is a clinical relevant difference between the
outcome proportions in the two arms.
H0: pe – pc = 0 vs. Ha: |pe – pc| >= d
where
pe is the proportion with outcome in the experimental arm
pc is the proportion with outcome in the control arm
Test Level and Power
a= P(D>k under H0: d=0) =
P(Z>za), Z~N(0,1)
g=1-b= P(D<k under Ha: d>d) =
P(Z<=-zb)
Test Statistic
X ~N(np,np(1-p))
P=X/n ~N(p,p(1-p)/n)
Assume pooled variance
Var[D] = {pe(1-pe)+pc(1-pc)}/n
k=za {pe(1-pe)+pc(1-pc)}½ n-½
k=zg {pe(1-pe)+pc(1-pc)}½ n-½
Sample Size in Clustered
Randomized Control Trial
The sample size of each arm
n = (za+zg)2 sp2 / d2
where
a is the level of the test
g=1-b, and b is the power of the test
sp2 = (pe(1-pe) + pc(1-pc))*k the variance of a single case
d=pe–pc the difference between arm proportions
Donner A, Klar N. Methods for comparing event rates in intervention studies when the
unit of allocation is a cluster. Am J Epid 1994; 140:279-89.
Intra-Class Correlation
•ICC proportion of total variance that is attributed to
between clusters variation
r = S nipi(1-pi)
(m-1)p(1-p)
where ni and pi are the cluster size and proportion,
and m and p are the average cluster size and
proportion when cluster sizes are not too variable
•Then inflation factor
k = [1-(1-m)r]
Power sensitivity to variables
•Differences in Proportions
•Intra-class correlation
•One or Two-sided Tests
•Sample Size
Power of Clinically Relevant
Difference Test
Normal A pproximation of Control and Experimental Proportions
4
Control
Experimental
k
2
1
0
density
3
d
0.2
n
168
icc 0.04
Power0.634
-0.2
0.0
0.2
0.4
0.6
0.8
Distribution of Estimated Arm Proportions
1.0
1.2
Effect of Difference in Proportions
Normal Approximation of Control and Experimental Proportions
5
d
n
icc
Power
0.6
168
0.04
1
0
1
1
2
2
density
4
d 0.01
n 168
icc 0.04
Power0.063
3
Control
Experimental
k
3
4
Control
Experimental
k
0
density
Normal Approximation of Control and Experimental Proportions
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
1.2
-0.2
0.0
0.2
0.4
0.6
0.8
Distribution of Estimated Arm Proportions
Distribution of Estimated Arm Proportions
d= pe – pc
.01
.20
.60
Power
.063
.634
1.000
1.0
1.2
Effect of Intra-Class
Correlation on Power
Normal Approximation of Control and Experimental Proportions
Normal Approximation of Control and Experimental Proportions
Control
Experimental
k
3
5
Control
Experimental
k
d
0.2
n
168
icc 0.1
Power0.381
density
3
1
2
0
1
0
density
2
4
d
0.2
n
168
icc 0.02
Power0.792
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
-0.2
1.2
Distribution of Estimated Arm Proportions
0.0
0.2
0.4
0.6
0.8
Distribution of Estimated Arm Proportions
r
.02
.04
.10
Power
.792
.634
.381
1.0
1.2
Effect of One or Two Sided Tests
Normal Approximation of Control and Experimental Proportions
4
0.2
d
n 168
icc 0.04
Power0.745
1
0
1
2
density
3
d 0.2
n 168
icc 0.04
Power0.634
3
Control
Experimental
k
2
4
Control
Experimental
k
0
density
Normal Approximation of Control and Experimental Proportions
-0.2
0.0
0.2
0.4
0.6
0.8
1.0
Distribution of Estimated Arm Proportions
1.2
-0.2
0.0
0.2
0.4
0.6
0.8
Distribution of Estimated Arm Proportions
Test
2-sided
1-sided
Power
.634
.745
1.0
1.2
Sample Size Effect on Power
Normal Approximation of Control and Experimental Proportions
6
d 0.2
n 336
icc 0.04
Power0.903
1
0.5
2
1.0
density
4
5
d 0.2
42
n
icc 0.04
Power0.209
1.5
Control
Experimental
k
3
2.0
Control
Experimental
k
0
0.0
density
Normal Approximation of Control and Experimental Proportions
0.0
-0.2
0.2
0.4
0.6
0.8
1.0
1.2
-0.2
Distribution of Estimated Arm Proportions
0.0
0.2
0.4
0.6
0.8
Distribution of Estimated Arm Proportions
n
42
168
336
Power
.209
.634
.903
1.0
1.2
Power function of Difference
The Power(d) function of selected sample size, n
d= pe – pc
The units in the experimental and control arms are
considered independent the variance of d is the sum the
I estimated the overestimated the variance using p=.5 in
the variance calculation
Some Power (d) curves
0.6
0.4
0.2
Power
Power
Power
Power
Power
n=336
n=168
n=84
n=42
n=21
0.0
Power(difference)
0.8
1.0
Power Function of difference between two Proportions
0.0
0.2
0.4
0.6
Difference in Proportions
0.8
1.0
Permanent Colostomy Rates
•Colostomy rates
• vary widely (0 to 68%) in Ontario Hosp 10+ cases
• average 32.5%
• icc calculated icc=.039989 based on our sample
60
40
20
0
Colostomy Rate (%)
80
100
Colostomy
Rates
in
Ontario
Colostomy Rate by Rectal Cancer Hospital Case Volume in Ontario
0
50
100
Hospital Case Volume (April 1995- March 1998 )
150
Local Recurrence Rates
• found to range from 10 to 45% by surgeon in Edmonton
• we estimate to be 20% in Ontario
• no way to estimate icc
• use 4% – consistent with the icc of other colorectal
cancer surgery outcomes in Ontario
i.e. operative mortality and long-term survival
Theriault M, Simonovic M. Hierarchical Modeling in Cancer Outcomes. CIHR Annual
Research Conference, 2003.
Long-term Survival Rate
• surprisingly survival rates are not known
• estimated to be about 35%
• no way to estimate icc
• use 4% – consistent with the icc of other colorectal
cancer surgery outcomes in Ontario
i.e. operative mortality and long-term survival
• Cox proportional modelling is much more efficient than
modeling of fixed term survival binomial outcome
Theriault M, Simonovic M. Hierarchical Modeling in Cancer Outcomes. CIHR Annual
Research Conference, 2003.
Samples Size Inputs
• icc r= .04
• cluster size m=42
• Test level a=05 is standard
• Reviewers demand 2-sided test
• Power g=.8 to .9 is standard, we use .8
• We selected the calculated sample size of local
recurrence: n=336 and k=8 hospitals in each arm
Sample Size Requirements
Outcome
pc
pe
d
n
k
Colostomy
.30
.15
-.15
311
7.4
Recurrence
.20
.08
-.12
336
8.0
5-yr Survival
.35
.50
.15
440
10.5
Summary
• ICC has a huge impact on Power and hence on required
sample size
• Key parameters to calculate sample size must be
estimated, i.e. r and p for these outcomes has not been
published
• Grant reviewers demand 2-sided until the direction of
effect is well established
• Room for more work in applying these in medical
research
Acknowledgements
• Marko Simunovic MPH, FRCS(C)1,2,3
• Charlie Goldsmith, PhD2
1. Departments of Surgery, McMaster University
2. Clinical Epidemiology and Biostatistics, McMaster University
3. Juravinski Cancer Centre, Hamilton Health Sciences