Antimicrobial Agents (Sulfonamides and Quinolones)
advertisement
")
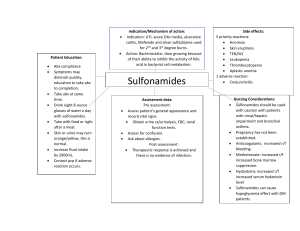
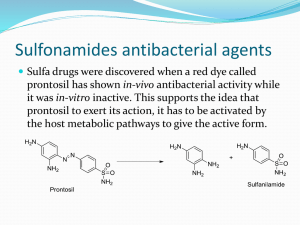
Antimicrobial Agents (Sulfonamides and Quinolones) Prof. R. K. Dixit Pharmacology and Therapeutics K.G.M.U. Lucknow dixitkumarrakesh@gmail.com Objectives After completion of this lecture you will be able to – Know about sulphonamides • • • • • • Types (Classification) MOA Combination with Trimethoprim or Pyrimethamine Uses ADRs, DDI, and Contraindications Special points – Know about Quinolones • • • • • Types (Classification) MOA Uses ADRs, DDI, and Contraindications Special points Suphonamides (Sulfonamides) [F=USA, Ph=UK] First antimicrobial agents effective against bacteria Prontosil Red (sulfonamide chrysoidine dye) – by- Domagk – for – streptococcal infection. Broken down in body – into- Sulfanilamide (Active against bacteria) Use increased –Overuse- Development– Resistance Rarely used (alone) today due to ◦ Availability of safer and effective antibiotics ◦ Resistant Sulfonamides today used as combination Trimethoprim (Cotrimoxazole) as antiBacterial Pyrimethamine (Cotrimazine) as anti-Malarial. TB in PM Sulfonamides (Chemistry) • Derivatives of • Sulfanilamide (p-Aminobenzene sulfonamide) • Individual member differs in nature of N1substitution. • N1substitution governs– Pharmacokinetic properties • Free amino group at - (N4)–antibacterial activity. DK- 41 Sulfonamides (Members) Short Acting (4-8hrs) •Sulfisoxazole •Sulfadiazine•Less protein bound, •Penetrates BBB- Meningitis •Acetylated product is less soluble and cause for crystalluria Intermediate acting (8-12 hrs) •Sulfammoxazole •Sulfamethoxazole – •Combination with Trimethoprim, FDC ( Cotrimoxazole) • High fraction is acetylated and may lead to Crystalluria Long acting (> 12 hrs) •Sulfadoxine •Very high plasma protein binding and slow renal excretion, •Longest acting, •Used in malaria, Toxoplasmosis, Pneumocystis, •In combination with Pyrimethamine, •Sulfamethoxypyrazine Special purpose Sulfonamides Sulfacetamide•Ocular drops Mafenide – •Active in presence of •Pus and Pseudomonas •Produces severe burning •Have Carbonic Anhydrase Inhibitor activity •Can alkalinize urine, •Produce Acidosis, & Hyperventilation Silver sulfadiazine – • Releases silver ions (antimicrobial ), • Burn dressing, • May be absorbed Sulfasalazine – (Sulfapyridine + 5-ASA) • Used in • Rheumatoid arthritis • Ulcerative colitis and Triple Sulfa = •Sulfamethazine •Sulfadiazine •Sulfamerazine MetDiaMerza Sulphasalazine = •5Amino Salicylic Acid (Used for Ulcerative Colitis) + •Sulphapyridine (Used for Rheumatoid Arthritis) Sulfasalazine Sulfapyridine Absorbed, Useful in RA, Produces ADR 5-Amino Salicylic Acid Not absorbed, Anti-inflammatory in GIT, Useful in IBD (UC, and Crohn’s disease), Suphonamides (MOA) • Bacteria synthesize folic acid from PABA • Sulfonamide is – Structural analogue of PABA and – Inhibit Dihydrofolic Acid Synthetase • Dihydrofolic acid by Dihydrofolic acid synthetase. • Tetrahydrofolic acid by Dihydrofolic acid reductase • Tetrahydrofolic acid for synthesis of RNA, DNA • PABA antagonizes action of Sulfonamides • Pus is rich in PABA, (Purines, Pyrimidines). • Procaine local anesthetic releases PABA and reduces Sulfonamides action • Human cells –Utilize preformed Folic Acid and –Enzymes less affinity for Sulphonamides. Sulfonamides (MOA) PABA + Dihydropteridine Dihydropteroic acid Synthetase Static Sulfonamides (PABA analogues) Sulfomethoxazole (Bacterial) Sulfadiazine (Bacterial) Sulfodoxine (Malarial) Dihydropteroic acid Glutamate + Cotrimoxazole Dihydrofolate Reductase Folic Acid Cidal Dihydrofolic Acid Dihydrofolate Reductase (Mammalian) Cotrimazine Timethoprim (Bacterial) / Pyrimethamine (Malarial) Static Tetrahydrofolic Acid RNA DNA Proteins Nucleic Bases Amino Acids Suphonamides Resistance is due to •Increased production of PABA •Folate synthetase affinity Less •Adoption of alternate pathway in folate metabolism Spectrum •Primarily bacteriostatic •Both Gram positive and gram negative Pharmacokinetics•Orally absorbed •PPB is variable (10-95%) •Cross Placenta •Metabolized by Acetylation •By microsomal acetyl transferase •Acetylated metabolites inactive but •Produce Crystalluria Adverse effects •Crystalluria •Dose related Tt. Fluid, Alkalizers •Fixed Drug Reaction, Hypersensitivity •Stevens-Johnson syndrome, •Photosensitization, •Hepatitis •Contact Dermatitis •Haemolysis in G-6-P-D deficiency •Kernicterus•Premature new born, Bilirubin in brain Sulphur Containing Drugs (Diuretics, COX-2 inhibitors, Protease inhibitors, Antileprotics) •Dapsone •Sulfonylurea (Antidiabetic) •Protease inhibitors (Anti HIV) •Carbonic Anhydrase inhibitors,, •Celecoxib, Valdecoxib (COX-2) •Loop diuretics, •Thiazides D S P Caught Lootera Thief Fixed Drug Reactions • Fixed drug reactions are so named because they recur at the same site with each exposure • Drugs causing fixed drug eruptions: – Trimethoprim, Sulfonamides , Cotrimoxazole – Fluconazole, Ciprofloxacin, Doxycycline, Clarithromycin, NSAIDs, Phenytoin, Cetirizine, Pseudoephedrine Fixed Drug Reactions • Usually develop within 30 minutes to 8 hours of taking the drug. • They are sometimes solitary at first, but with repeated attacks new lesions may appear and existing ones may increase in size. • Involves limbs, around mouth, eyes, genitalia and perianal areas • As healing occurs, crusting and scaling followed by brown colour at the site. Stevens–Johnson syndrome, • A form of toxic epidermal necrolysis (TEN) • Life-threatening skin condition, • Cell death causes the epidermis to separate from the dermis. • The syndrome is thought to be a hypersensitivity complex that affects the skin and the mucous membranes. • Begins with fever, sore throat, and fatigue, and commonly misdiagnosed • Ulcers and other lesions begin to appear in the mucous membranes, almost always in the mouth and lips, but also in the genital and anal regions. • Conjunctivitis of the eyes occurs in about 30% • Characterized by confluent epidermal necrosis with minimal associated inflammation. • An idiosyncratic, delayed-hypersensitivity reaction. • Slow acetylators, Immunocompromised, and patients with brain tumors undergoing radiotherapy with concomitant antiepileptics are among those at most risk. • Patients with sulfonamide-induced toxic epidermal necrolysis have been shown to have a slow acetylator genotype that results in increased production of sulfonamide hydroxylamine . • These drug metabolites may have direct toxic effects or may act as haptens that interact with host tissues, rendering them antigenic. • Causes • • • • • • Disorder of the immune system. The immune reaction can be triggered by drugs or infections. Genetic factors are associated with a predisposition to SJS The cause of SJS is unknown in one-quarter to one-half of cases. May be after viral infections, malignancies, medications. No reliable test to establish a link between a particular drug and SJS • A leading cause sulfa drugs. • Other drugs – Allopurinol, Barbiturates,Carbazepine,Valproate, Ethosuximide, Valdecoxib, Phenytoin, Lamotrigine, – Levofloxacin, Diclofenac,, Isotretinoin, Fluconazole, , sitagliptin, , Vancomycin, Pyrimethamine, Cefixime, Drug Interactions •Inhibit Metabolism & •Displace from protein binding site Increased Concentration of Other Drugs (Phenytoin, Tolbutamide, Warfarin, Methotrexate etc.) Uses •Rarely used alone •Some times for chronic UTI •Topical for conjunctivitis, Burn Cotrimoxazole Fixed Dose Combination (FDC) of Trimethoprim (Diaminopyridine) + Sulfamethoxazole (Sulfonamide) Preparation ratio 1:5 Ratio at site of action 1:20 Produce Sequential block •Combination is Cidal (Individual component static) • Why Sulfamethoxazole? – because of similar t1/2 ( half life 10 hrs) • Why Ration of 1:5? – Trimethoprim has large volume of distribution. – Optimum synergism at ratio 1: 20 at site of action. • Why not harming human cells? Trimethoprim is 50,000 times active against bacterial DHFRase Mammalian cells use preformed folic acid Spectrum •Gram Positive •Gram negative Resistance •Acquire DHFRase of lower affinity Adverse effects Drugs having Anti-folate actions •Pralatrexate •Pemetrexed •Proguanil •Pyrimethamine •Methotrexate •Trimethoprim •Same as sulfonamides •Renal toxicity •Teratogenicity •Trimethoprim, an antifolate enhance teratogenic effect •Bone marrow suppression ( in elderly) Drug Interactions •Same as sulfonamide •Cotrimoxazole + Diuretics – Chance of thrombocytopenia Uses of Sulphonamides and Cotrimoxazole •Faciomaxillary infections •RTI •UTI •Prostatitis •Typhoid •Bacterial diarrhea and dysentery •Pneumocystis infection in AIDS •Chancroid •Burn dressing Cotrimoxazole • Drug of Choice – Pneumocystis pneumonia – Nocardia – Yersinia enterocolitica • As Alternative – Salmonella typhi – Shigella, E.coli – Vibrio cholerae – Brucella – Atypical mycobacterium Thanks