Document
advertisement

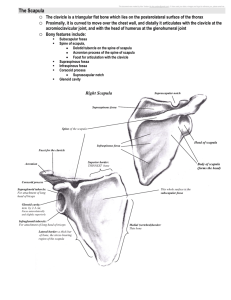
What is the Shoulder girdle? What is the importance of Shoulder Girdle Increase the ROM for Upper limb (up to 180°) Provide More space to reach for upper limb Provide an stable base for upper limb function What are the Joints of the Shoulder girdle? Four interdependent linkages for Shoulder Complex Functional Articulation: Scapulothorasic Joint (STJ) Anatomical Articulation: Sternoclavicular Joint (SCJ) Anatomical Articulation: Acromioclavicular Joint (ACJ Anatomical Articulation: Glenohumeral Joint (GHJ) Sternoclavicular Joint What is the role of Sternoclavicular Joint within shoulder girdle? Functional base for scapula Movement in Clavicle and SCJ Movement in Scapula Thoracic Can You Describe the Sternoclavicular Joint? Sternoclavicular Joint Consists of two saddle-shaped surfaces but A plane Synovial Joint 3 degree of freedom Joint Capsule 3 Major Ligaments A Joint Disc 4 joint’s area contact Clavicle Movement in SCJ is due to Sternocalvicular the change in contact area Disc between Manuberium Can you describe the function of Sternoclavicular Disc Joint? A fibrocartilage joint disk, or meniscus, that increases congruence between joint surfaces Acts like a hinge or pivot point during clavicle motion. Act like axis in the SCJ In Elevation/Depression Clavicle move against Manuberium and Disc Upper part of Disc act like axis) In Protraction/Retraction Disc and Clavicle Move against Manuberium Lower part of Disc act like axis the mechanical axis for these two movements located not at the SC joint itself but at the more laterally located costoclavicular ligament How the disc Joint does provide stability for SCJ? Disc has an Important Role in Joint Stability By Creation congruent between Joint surface By absorption coming stresses to the lateral end of clavicle Three-Compartment SC Joint Anatomic examination of the SC articulation has led to the proposal that there are three functional units 1. a lateral compartment between the disk and clavicle for elevation and depression; 2. a medial compartment between the disk and manubrium for protraction and retraction; 3. a costoclavicular joint for anterior and posterior long axis rotation. Sternoclavicular Joint Capsule and Ligaments The SC joint is surrounded by a fairly strong fibrous capsule but must depend on three ligaments for the majority of its support. These are the sternoclavicular ligaments, Can you name the Sternoclavicular Ligaments? Sternoclavicular Lig (Ant & Post) Costoclavicular Lig (Ant & Post) Inter Clavicular Lig What is the function of Sternoclavicular Ligaments? Sternoclavicular (Ant & Post) Lig Costoclavicular (Ant & Post parts) Lig Strengthening of Ant and Post part of Joint Prevent of Ant and Post Movements of Clavicle Very strong Lig Both parts resist against the 1) superior force from SCM and 2) against elevation of the lateral end of clavicle At the limit reach, they are responsible for inferior gliding of clavicle Post part prevent of inward movement of clavicle (absorb of forces acts on the Disc from arm) Inter Clavicular Lig Control 1) Depression of clavicle, 2) superior gliding of clavicle and protect subclavian artery and Brachial plexus and Weight bearing of upper arm by help of upper capsule Integrity of These elements Clavicle SCJ Disc Manuberium Ligaments Capsule PROVIDS Three Major functions for SCJ 1)Resist against Applied stress from Upper arm 2)Provide Mobility for Upper arm 3)Provide a Strength Base for Upper arm What are the Sternoclavicular Movements? Motions of any joint are typically described by identifying the direction of movement of the portion of the lever that is farthest from the joint. Elevation/Depression Protraction/Retraction Anterior/Posterior Rotation Can you describe Elevation/Depression movements? Occur around the Ant-Post Axis which located in Costoclavicula Lig In the plan that convex surface of clavicle glide against concave surface of manubrium and Disk Opposite Movement of medial part of clavicle Up to 48 degree Elevation and 15 degree Depression Elevation of clavicle accompanied by elevation of scapula and its upward rotation Small magnitudes of medial-lateral translation and superior/inferior translation in the medial aspect of clavicle Elevation and Depression Can you describe the Protraction/Retraction movements? Occur vertical axis locate in costoclavicula Lig In the plan that concave surface of clavicle glide against convex surface of manubrium In protraction, lateral end rotate anteriorly, and medial end slide anteriorly 15- 20 degree Protraction and 20-30 degree Retraction Pro/Ret of clavicle is accompanied by Pro/Ret of scapula Protraction and Retraction Can you describe the Anterior/Posterior Rotation? Occur around the longitudinal axis of clavicle intersecting AC and SC Joint An Spin movement saddle surface of medial part of clavicle and manuberium/first costal cartilage Movement start from neutral position only toward posterior rotation 35-55 ° Post Rot and 10 ° available Ant Rot It serve the last 30 degree of upward rotation of scapula. Posterior And Anterior Rotation ■ Sternoclavicular Stress Tolerance The Complex of bony segments, Capsuloligamentous structure, and the SC disk produce a joint with dual functions of mobility and stability. The SC joint contribute to upper limb mobility, and withstanding imposed stresses. Although the SC joint is considered incongruent, the joint does not undergo the degree of degenerative change common to the other joints of the shoulder complex. Dislocations of the SC joint represent only 1% of joint dislocations in the body. Acromioclavicular Joint Acromioclavicular Joints Characteristics Plan Synovial Joint 3 rotational and 3 transitional degrees of Freedom Weak capsular joint Joint Disc Two Major Ligaments Superior & Inferior Acromioclavicular ligaments Integration of joint surface Provide horizontal stability Coracoclavicular Lig. Its primary function included: Primary function of ACJ Primary function 1. Allow the scapula additional range of rotation on the thorax 2. Allow for adjustments of the scapula (tipping and internal/external rotation) in order to follow the changing shape of the thorax as arm movement occurs. 3. Allows transmission of forces from the upper extremity to the clavicle. Articular Surface and Joint Disc of ACJ The articular facets, considered to be incongruent, vary in configuration Intra-articular movements for this joint are not predictable. A Joint disk with variable in size between individuals exist in AC joint It plays as a “meniscoid” fibrocartilage remnant within the joint to develop each articulating surface during upper extremitymovement The Acromioclavicular Joint Acromioclavicular Capsule and Ligaments Capsule is weak and cannot maintain integrity of the joint without reinforcement by ligaments The superior acromioclavicular Lig are reinforced by aponeurotic fibers of the trapezius and deltoid muscles and assists capsule by Apposing articular surfaces Controlling A-P joint stability. The fibers of the superior AC ligament are the superior joint support stronger than the inferior Acromioclavicular Capsule and Ligaments Coracoclavicular Ligaments which divided into: Lateral portion, the trapezoid ligament, provides the primary restraint for the AC joint in the superior and inferior directions Medial portion, the conoid ligament. Provides the majority of resistance to posterior translatory forces applied to the distal clavicle. They are separated by adipose tissue and a large bursa Both portions of the coracoclavicular ligament limit upward rotation of the scapula at the AC joint Transfer Medially directed forces on humerus to the SCJ Transfer the rotational force of scapula to the clavicle and then cause Posterior Rotation at SCJ When a person bears weight on the arm, a medially directed force up the humerus (1) is transferred to the scapula (2) through the glenoid fossa and then to the clavicle (3) through the coracoclavicular ligament Acromioclavicular Motions The primary rotatory motions of AC joint are Internal/external rotation, Anterior/ posterior tipping or tilting, Upward/downward rotation These motions occur around axes that are oriented to the plane of the scapula rather than to the cardinal planes. Small translatory motions of AC joint included: Anterior/Posterior, Medial/Lateral, Superior/Inferior. Plane of AC joint Movements What movement does occur in the Acromioclavicular joint? 1- Internal and External Rotation Internal and External Rotation Occurs around an approximately vertical axis through the AC joint To Maintain contact of the scapula to horizontal curvature of the thorax during Protraction and Retraction To orient the glenoid fossa toward the plan of humeral elevation 30 degree the total ROM An Anterior/Posterior translatory movement Internal and External Rotation at AC joint Glenoid Fossa is the reference for naming the movement Because of the thorax curvature, Internal/External Rotation is a necessary movement for protraction and Retraction Anterior and Posterior Tipping Occurs around an oblique “coronal” axis of joint Ant. tipping will result in the acromion tipping forward and the inferior angle tipping backward during downward rotation and also Elevation of scapula Posterior tipping will rotate the acromion backward and the inferior angle forward. during upward rotation and also Depression of scapula To Maintain contact of the scapula with the contour of the rib cage and orient the glenoid fossa during arm flexion and abduction 30-40 degree the total ROM A Superior/posterior translatory movement Anterior and Posterior Tipping The superior aspect of scapula is the reference of naming the movement The acromion has slightly translatory anteriorly/posteriorly movement Upward and Down Ward Rotation at AC Joint Around an A-P axis (perpendicular to scapula) Direction of Glenoid Fossa is the reference for the naming the movement Acromion has a small medial/lateral Translatory movement 3-Scapula Upward and Downward Rotation Help to orient the glenoid fossa upward or downward Coraco-Clavicular Ligament limit this movement Posterior rotation of clavicle lax the lig So upward rotation can be done in the AC Joint 30 degree Upward Rot 17 degree Downward Rot Acromioclavicular Stress Tolerance AC joint is extremely susceptible to both trauma and degenerative change due to the its small and incongruent surfaces Degenerative change is common from the second decade with narrowed joint space by the sixth decade. Treatment of sprains, subluxations, and dislocations of this joint occupies a large amount of the literature on the shoulder complex Acromioclavicular Stress Tolerance Various classification of injury commonly Type I injuries consist of a sprain to the AC ligaments, Type II injuries typically have ruptured AC ligaments and sprained coracoclavicular ligaments Type III injuries result in rupture of both sets of ligaments, Types I, II, and III AC separations all involve inferior displacement of the acromion in relation to the clavicle caused by the loss of support from the coracoclavicular ligaments Acromioclavicular Stress Tolerance Various classification of injury commonly Type IV injuries have a posteriorly displaced lateral clavicle, often pressing into the trapezius posteriorly, with complete rupture of both the AC and coracoclavicular ligaments Type V injuries also involve an inferior displacement of the acromion and complete rupture of both sets of ligaments and are distinguished from type III by a severity of between three and five times greater coracoclavicular space than normal. Type VI injuries have an inferiorly displaced clavicle in relation to the acromion, with complete ligament rupture and displacement of the distal clavicle into a subacromial or subcoracoid position. Scapulothorasic Joint Rotation at AC Joint SCJ Elev/Dep and ACJ Rotation are necessary movements for Scapula Elevation and Depression ACJ Rotation and SCJ Elev and Post Rotation are the necessary movements for Scapular upward Rot Resting Position of scapula Position of Scapula on the Thorax 2 inches from the midline Between 2nd and 7th ribs 30-45 degree internally rotated from the coronal plane 10-20 degree anteriorly tipping from vertical 10-20 degree upward rotation, it is different among the individuals What is the Movement of Scapula? Elevation/Depression Protraction/Retraction Upward Rotation/Downward Rotation Scapula Upward and downward Rotation Upward rotation of the scapula plays a significant role in increasing the range of elevation of the arm Approximately 60º of upward rotation is available. Considering the closed-chain relationship between the SC, AC, and ST joints, they contribute to scapula upward/downward rotation by: SC joint elevation/depression, SC joint posterior/anterior rotation AC joint upward/downward rotation Most often, scapular upward/downward rotation results from a combination of the SC and AC motions. Scapula Upward and downward Rotation Scapula Elevation/Depression Scapular elevation and depression can be isolated by shrugging the shoulder up and depressing the shoulder downward. It is described as translatory motions Scapular elevation, occurs by elevation of the clavicle at the SC joint and requires Scapula adjustments in anterior/posterior tipping internal/external rotation at the AC joint to maintain the scapula in contact with the thorax Scapula Elevation/Depression Scapula Protraction/Retraction Scapula Protraction and retraction are described as translatory motions of the scapula away from or toward the vertebral column, respectively. However, if protraction occurred as a pure translatory movement, only the vertebral border of the scapula would remain in contact with the rib cage. In reality during protraction, scapula follows the contour of the ribs by rotating internally and externally at the AC joint and clavicular protraction and retraction at the SC joint So, glenoid fossa facing anteriorly with the full contact of scapula with the rib cage Scapula Protraction/Retraction Scapula Internal/External rotation Scapular internal and external rotation are normally not overtly identifiable on physical observation but are critical to its movement along the curved rib cage. The Movement normally accompany protraction/ retraction of the clavicle at the SC joint Isolated Scapula Int rotation at the AC joint, cause Prominence of the vertebral border of scapula Loss of contact of scapula with the thorax. Which is referred to clinically as scapular “winging” Excessive Int rotation may be indicative of pathology or poor neuromuscular control of the ST muscles. Pathologic Scapula Internal Rotation Scapula Anterior/Posterior Tipping Anterior/Posterior tipping is normally not obvious on clinical observation and yet is critical to maintaining contact of the scapula against the curvature of the rib cage Movement occurs at the AC joint Isolated excessively Ant/Post Tipping at the AC joint will result normally will accompany anterior/posterior rotation of the clavicle at the SC joint in prominence of the inferior angle of the scapula Ant. tipped scapula may occur in pathologic situations (poor neuromuscular control) or in abnormal posture. Pathologic Scapula Anterior Tipping What are the Scapulathorasic Functions? Final function of this Joint 1. Adjustment of gelenoid direction 2. To Increased ROM for upper arm 3. To Provide an Strong Base to control Rolling and gliding Movements for Humorous Surface Scapulothorasic Stability Scapula Stability on the thorax is provided by 1. The structures that maintain integrity of the linked AC and SC joints such as ligaments, capsule and joint disc. 2. The muscles that attach to both the thorax and scapula maintain contact between these surfaces 3. These muscles also provide stabilization by pulling or compressing the scapula to the thorax. The scapula, with its associated muscles and linkages, performs mobility and stability functions so well that it serves as a premier example of dynamic stabilization in the human body