Endocrinology teaching ppt copyright free
advertisement

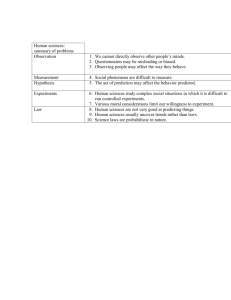
Phase 2A Endocrinology Charlotte Allan Joe Hardwick The Peer Teaching Society is not liable for false or misleading information… Diabetes Mellitus Type 1 • Autoimmune destruction of pancreatic beta cells in the islets of Langerhans • Antibodies present for several years before onset of symptoms • T cell mediated • Associated with other autoimmune conditions • Around 300,000 patients in the UK • Usually presents in under 25s, often before puberty The Peer Teaching Society is not liable for false or misleading information… Signs and Symptoms • • • • • • • • Thirst (polydipsia) Polyuria Nocturia Weight loss Fatigue Blurred vision Nausea Decreased concentration • Hyperglycaemia (>11mmol/L) • Glucosuria • Ketonuria The Peer Teaching Society is not liable for false or misleading information… Treatment • Insulin • Delivered via subcutaneous injection • Usually a basal/bolus regime – basal = long acting bolus = short acting The Peer Teaching Society is not liable for false or misleading information… Diabetic Ketoacidosis • Lack of insulin means glucose cannot be used as a source of energy • Therefore fat has to be used instead • A by product of fat breakdown are ketone bodies, and these build up, leading to excess ketones in the blood • Ketones are acidic, hence leading to ketoacidosis • Peripheral lipolysis -> ↑circulating FFA -> hepatic conversion to ketones -> acidosis • Hyperglycaemia leads to osmotic renal diuresis and dehydration, which worsens the acidosis The Peer Teaching Society is not liable for false or misleading information… Causes of DKA • • • • Undiagnosed T1DM Interruption of insulin therapy Stress Intercurrent illness – surgery/infection The Peer Teaching Society is not liable for false or misleading information… DKA Signs and Symptoms • • • • • • Very dehydrated Vomiting – worsens dehydration Sunken eyes Deep rapid breathing (Kussmaul) Acetone smell on breath (pear drops) Altered consciousness The Peer Teaching Society is not liable for false or misleading information… DKA Investigations & Treatment • • • • Blood glucose - >11mmol/L Ketonaemia pH <7.3 with bicarb < 15 Glucosuria/ketonuria (delayed sign) • • • • • • Find and treat any suspected infection Replace fluid and electrolytes – Saline with potassium Replace insulin Restore acid/base balance over 24 hours Monitor fluid balance Potassium given to avoid hypokalaemia on reintroduction of insulin The Peer Teaching Society is not liable for false or misleading information… Type 2 Diabetes • • • • Polygenic and environmental aetiology Beta cell mass <50% at diagnosis Increased insulin resistance Decreased insulin secretion • Risk factors: obesity, calorie and alcohol excess, lack of exercise, male, high triglycerides • Approximately 3 million patients in the UK • Another 1 million undiagnosed The Peer Teaching Society is not liable for false or misleading information… Diagnosis of T2DM • Symptoms less prominent than T1DM Often detected on screening: • Fasting glucose >7mmol/L • Random glucose >11.1mmol/L • HbA1C >48mmol/L • OGTT: Fast overnight, give 75g glucose, measure glucose before and 2/24 after. >11.1mmol is positive • For diagnosis: symptoms of hyperglycaemia AND one raised blood glucose reading, OR • Raised blood glucose on 2 separate occasions The Peer Teaching Society is not liable for false or misleading information… Other Hyperglycaemia • Impaired glucose tolerance = fasting glucose <7mmol/L and OGTT 7.7-11mmol/L • Impaired fasting glucose = fasting glucose 6-7 Gestational diabetes: • Occurs in 4% of pregnancies • RF: >25yr, obesity, FH, non-caucasian • Issues: increased birth weight, neonatal hypoglycaemia • OGTT at 6/52 post-partum The Peer Teaching Society is not liable for false or misleading information… Hyperosmolar Hyperglycaemic State (HHS) • • • • • History of approx. 1 wk Often elderly patient Common initial presentation of T2DM Marked dehydration and glucose >35mmol/L Acidosis absent as they have sufficient insulin to prevent excessive fat breakdown Treatment: • Rehydrate with saline IVI over 48hours • Replace potassium • Wait 1 hour before using insulin as it may be unnecessary The Peer Teaching Society is not liable for false or misleading information… Hypoglycaemia • Commonest endocrine emergency • Plasma glucose <3mmol/L • Sweating, anxiety, hunger, tremor, dizzy, confusion, irritability, drowsiness, seizure, coma • Most common cause is insulin treatment in T1DM combined with.. Increased activity, missed meal, accidental/non-accidental OD Treatment: • Oral sugar then starch • If unable to swallow – 25-50ml IV glucose 50% or glucagon IM if no IV access The Peer Teaching Society is not liable for false or misleading information… Diabetic Complications MACROVASCULAR Vascular disease – chief cause of death • MI – 4x risk • Stroke – 2x risk • Address other RF – smoking/diet/HTN etc. MICROVASCULAR Nephropathy • Leading cause of dialysis and kidney transplant • High urine albumin:creatinine ratio indicates early renal disease and increased vascular risk • Treatment: control BP, restrict dietary protein, ARB, ACE-I, spironolactone The Peer Teaching Society is not liable for false or misleading information… Diabetes Complications MICROVASCULAR Retinopathy • Background – microaneurysms (dots), haemorrhages (blots) and hard exudates • Pre-proliferative – cotton wool spots (infarcts), haemorrhages, venous beading • Proliferative – new vessels formed • Maculopathy – new vessels form on disc or ischaemic areas, proliferate, bleed, fibrose, can detach retina Laser photocoagulation is used to stop the production of angiogenic factors. Used in proliferative retinopathy/maculopathy The Peer Teaching Society is not liable for false or misleading information… Diabetic Feet Ischaemia • Absent foot pulses – may need doppler • May need angioplasty/stents Neuropathy • Decreased sensation – stocking distribution • Absent ankle jerk reflex • Deformity • Ulceration – painless, punched out • Burning pain in feet at night • Regular chiropody • Relieve pressure with therapeutic shoes & bed rest • Monitor for cellulitis – may need antibiotics The Peer Teaching Society is not liable for false or misleading information… Thyroid TRH = thyrotropin releasing hormone TSH = thyroid stimulating hormone (AKA thyrotropin) The Peer Teaching Society is not liable for false or misleading information… Hyperthyroidism • Excess free T3 and T4 • Grave’s disease is the most common cause • 5% caused by solitary toxic adenoma/nodule The Peer Teaching Society is not liable for false or misleading information… Grave’s Disease • • • • 2/3 of cases of hyperthyroidism F:M = 9:1 Usually presents at 40-60yrs Circulating IgG antibodies bind to TSH receptors on the thyroid, causing smooth thyroid enlargement and increased hormone production – especially T3 • Triggers – stress, infection or childbirth • RF: vitiligo, T1DM, Addison’s The Peer Teaching Society is not liable for false or misleading information… Symptoms of Hyperthyroidism • • • • • • • • • • Diarrhoea Weight loss Increased appetite Increased sweating Heat intolerance Palpitations Tremor Irritability Labile emotions Oligomenorrhoea +/- infertility The Peer Teaching Society is not liable for false or misleading information… Signs of Hyperthyroidism • • • • • • • • Fast/irregular pulse – SVT/AF Warm, moist skin Fine tremor Palmar erythema Thin hair Lid lag Lid retraction Goitre The Peer Teaching Society is not liable for false or misleading information… Grave’s Specific Signs Eye signs • Exopthalmos • Opthalmoplegia – weakness or paralysis of extraocular muscles - Pretibial myxoedema – oedematous swellings above lateral malleoli Thyroid acropachy – clubbing, painful finger and toe swelling The Peer Teaching Society is not liable for false or misleading information… Management • Blood Tests: TFTs – T3/4 elevated, TSH suppressed • • • • • Block & Replace – carbimazole (anti-thyroid) & thyroxine (T4) Titration of carbimazole only SE of carbimazole = agranulocytosis Radio-active Iodine Thyroidectomy & replacement thyroxine • Emergency treatment = Beta blockers to reduce symptoms then carbimazole • In pregnancy carbimazole is teratogenic so propylthiouracil is used instead • Wait four weeks after starting medication before re-testing The Peer Teaching Society is not liable for false or misleading information… Hypothyroidism • Usually primary, from thyroid disease, but may be secondary to reduced TSH from a pituitary disorder • Autoimmune, associated with anti-thyroid antibodies leading to lymphoid infiltration of the gland and eventual atrophy and fibrosis. • Reduced T3/T4 and high TSH • Association with other autoimmune conditions The Peer Teaching Society is not liable for false or misleading information… Signs & Symptoms • • • • • • • • • • • Tiredness Weight gain Cold intolerance Constipation Dry skin Dry, thin hair Bradycardia Slow-relaxing reflexes Low mood Menorrhagia Hoarse voice The Peer Teaching Society is not liable for false or misleading information… Treatment • Replace with levothyroxine until TSH is within normal and patient is asymptomatic The Peer Teaching Society is not liable for false or misleading information… Hashimoto’s Thyroiditis • • • • • • • • • • Autoimmune attack of the thyroid gland F:M 7:1 Usually middle aged, with family history Associated with other AI conditions Goitre to lymphocytic infiltration and fibrosis TPO (thyroid peroxidase) and/or thyroglobulin antibodies are responsible Complication: thyroid lymphoma Diagnosis: TPO antibody detection Symptoms of hypothyroidism, often with a hard, non-painful goitre Treatment: Levothyroxine The Peer Teaching Society is not liable for false or misleading information… Thyroid Cancer • 70% papillary, 20% follicular, 5% medullary (C cells) • F:M 3:1 • Thyroid nodules in 90% • Commonly metastasises to lung, liver, brain & bone • Treatment: total thyroidectomy with post-op radioactive iodine ablation • Lifelong levothyroxine treatment, titrated to suppress TSH – reduces recurrence The Peer Teaching Society is not liable for false or misleading information… Adrenal Glands The Peer Teaching Society is not liable for false or misleading information… The Peer Teaching Society is not liable for false or misleading information… Goodness Me Frank Gets Really Angry The Peer Teaching Society is not liable for false or misleading information… Cushing’s Syndrome Clinical state of glucocorticoid excess in the blood = Too much cortisol Usually iatrogenic, due to steroid or ACTH administration The Peer Teaching Society is not liable for false or misleading information… Cushing’s Syndrome ACTH dependent: • Pituitary dependent (Cushing’s disease) • Ectopic ACTH-producing tumours • ACTH administration Non-ACTH dependent: • Adrenal adenoma • Adrenal carcinoma • Glucocorticoid administration The Peer Teaching Society is not liable for false or misleading information… Cushing’s Syndrome Symptoms: • Weight gain – central obesity • Thin skin • Easy bruising • Stretch marks • Red puffy, round face • Tanned skin (Cushing’s disease only) • Muscle weakness • Depression • Tiredness The Peer Teaching Society is not liable for false or misleading information… Cushing’s Syndrome Signs • Impaired glucose tolerance • Hypertension • Pathological fractures – secondary to osteoporosis • Hypokalaemia • Striae • Proximal myopathy The Peer Teaching Society is not liable for false or misleading information… Cushing’s Syndrome Investigations: 48 hour low dose dexamethasone test: • ACTH depressed: non-ACTH dependent SCAN ADRENALS • ACTH unchanged: ACTH dependent SCAN PITUITARY Treatment: • Must have cortisol controlled before surgery or radiotherapy • Transphenoidal surgery to remove pituitary tumour in Cushing’s Disease +/- radiotherapy • Adrenal tumour resection for non-ACTH dependent The Peer Teaching Society is not liable for false or misleading information… The Peer Teaching Society is not liable for false or misleading information… Conn’s Syndrome • Excess mineralocorticoids in the blood stream – too much aldosterone • Usually caused by an aldosterone producing adrenal adenoma • More common in young females Signs & Symptoms: • Muscle weakness • Tiredness • Polyuria • Nocturia • Hypertension • Hypokalaemia The Peer Teaching Society is not liable for false or misleading information… Conn’s Investigations: Stop beta blockers, spironolatone, ACE-I, ARBs all may affect results and should be stopped • Aldosterone elevated • Renin is depressed • Adrenal CT/MRI to distinguish bilateral adrenal hyperplasia and adenoma Treatment: • Laparoscopic surgery to remove adenoma • Spironolactone for bilateral adrenal hyperplasia The Peer Teaching Society is not liable for false or misleading information… Adrenal Insufficiency Addison’s disease: • Destruction of entire adrenal cortex – reduced mineralocorticoids, glucocorticoids and sex steroids all reduced • Autoimmune Hypothalamic-pituitary disease: • Inadequate ACTH – insufficient glucocorticoids, but adequate mineralocorticoids due to RAAS Long term steroid therapy: • Leads to hypothalamic-pituitary-adrenal suppression if not reduced at appropriate rate The Peer Teaching Society is not liable for false or misleading information… Addison’s Disease • Associated with other AI diseases: Type 1 DM, pernicious anaemia and thyroiditis • • • • THIN TANNED TIRED TEARFUL • Other symptoms: N/V/D, headaches, muscle pain and lightheadedness • Very rare • Females>Males The Peer Teaching Society is not liable for false or misleading information… Addison’s Disease Investigations • Short ACTH stimulation test Impaired cortisol response confirms hypoadrenalism • MRI adrenals Treatment • In emergency (V low BP) – give hydrocortisone and fluids • Long term – glucorticoid (hydrocortisone) and mineralocorticoid (fludrocortisone) replacement. Titrate until patient is asymptomatic The Peer Teaching Society is not liable for false or misleading information… Addisonian Crisis • Severe hypotension with dehydration precipitated by intercurrent illness, infection, surgery or trauma • Treat with IVI and hydrocortisone The Peer Teaching Society is not liable for false or misleading information… Phaeochromocytoma • Rare catecholamine-producing tumour • Usually within the adrenal medulla • Excessive catecholamines may produce life-threatening hypertension and cardiac arrhythmias • Associated with Multiple Endocrine Neoplasia 2 (MEN2), Neurofibromatosis type 1 and Von-Hippel Lindau Syndrome • Commonly present in patients aged 30-50 • Often bilateral The Peer Teaching Society is not liable for false or misleading information… Phaeochromocytoma Symptoms • Headache • Profuse sweating • Tremor • Palpitations Signs • Hypertension • Postural hypotension • Neurofibromas • Café au lait spots The Peer Teaching Society is not liable for false or misleading information… Phaeochromocytoma Investigations • 24 hour urinary catecholamines (metadrenaline & normetadrenaline) • Plasma catecholamines • CT/MRI adrenals Treatment • Surgical resection of tumour • Pre-surgery: Alpha blockade (mirtazapine) THEN beta blockade (propanolol) The Peer Teaching Society is not liable for false or misleading information… Diabetes Insipidus • Cranial DI Deficiency of ADH Causes: familial, idiopathic, tumour, infection, post-surgery (most common, often transient) • Nephrogenic DI Failure to respond to ADH Causes: familial, idiopathic, renal disease, hypokalaemia, drugs The Peer Teaching Society is not liable for false or misleading information… Diabetes Insipidus • • • • • • Polyuria Nocturia Polydipsia Urine output = up to 15L daily Decreased skin turgor Signs of dehydration The Peer Teaching Society is not liable for false or misleading information… Diabetes Inspidus Investigations • High plasma osmolality WITH low urine osmolality • Hypernatraemia • High 24 hr urine volume • Failure of urinary concentration with fluid restriction • Fluid deprivation test: Give desmopressin: If urine osmolality rises = cranial DI If urinary osmolality is unchanged = nephrogenic DI The Peer Teaching Society is not liable for false or misleading information… Diabetes Insipidus Treatment: • Cranial DI = Intranasal desmopressin • Nephrogenic DI = Reverse cause, polyuria may be helped by thiazide diuretics e.g. bendroflumethiazide The Peer Teaching Society is not liable for false or misleading information… SIADH Syndrome of Inappropriate ADH Secretion • Important, but overdiagnosed cause of hyponatraemia Concentrated urine (↑ Na, ↑osmolality) + Hyponatraemia with low plasma osmolality Without: • Hypovolaemia • Oedema • Diuretics The Peer Teaching Society is not liable for false or misleading information… SIADH Causes: • Malignancy • CNS disorders – stroke, SAH, SDH, post neurosurgery • TB • Pneumonia • Drugs – opiates, SSRIs Treatment: • Treat cause and restrict fluid • Consider salt +/- loop diuretic if severe • Vaptans – e.g. tolvaptan – promote water excretion without loss of electrolytes, rarely used The Peer Teaching Society is not liable for false or misleading information… Growth Hormone Regulation The Peer Teaching Society is not liable for false or misleading information… Acromegaly • • • • Growth hormone stimulates soft tissue and skeletal growth Before epiphyseal fusion excess GH Gigantism After epiphyseal fusion excess GH Acromegaly Almost always due to a GH secreting pituitary tumour (somatotroph adenoma) The Peer Teaching Society is not liable for false or misleading information… Acromegaly Symptoms: • Hands and feet become larger and broader (spade like) • Unable to remove rings • Thickened, sweaty, greasy skin, especially on the face • Prominent jaw • Interdental separation • Changes can be gradual, so may go unnoticed • Vocal cords thickened – voice deepens • Tiredness • Muscle weakness The Peer Teaching Society is not liable for false or misleading information… Acromegaly Signs: • Hypertension • Impaired glucose tolerance • Bitemporal hemianopia (David and Goliath) The Peer Teaching Society is not liable for false or misleading information… Acromegaly Investigations: • GH level – non-specific if elevated • GTT – diagnostic if no suppression of growth hormone (growth hormone is usually inhibited by glucose) • IGF-1 is usually raised • MRI – pituitary adenoma Treatment: • Transphenoidal surgery +/- radiotherapy • Somatostatin receptor agonists e.g. octreotide • Dopamine agonists e.g. bromocriptine • GH antagonists - pegvisomant The Peer Teaching Society is not liable for false or misleading information… Disorders of Calcium Metabolism • Serum calcium levels are mainly regulated by parathyroid hormone (PTH) and vitamin D • Hypercalcaemia is much more common than hypocalcaemia Parathyroid Hormone: • 4 parathyroid glands, situated on posterior thyroid • PTH secreted from the chief cells of these glands • PTH increases, as ionised calcium falls, and vice versa • Has several major actions all of which raise serum calcium The Peer Teaching Society is not liable for false or misleading information… Parathyroid Hormone The Peer Teaching Society is not liable for false or misleading information… Hypercalcaemia Causes: • Most common - excess PTH, malignancy • Other - excess vit D, excess Ca intake, drugs Signs & symptoms: • Mild hypercalcaemia is often asymptomatic • General – tiredness, malaise, dehydration • Renal – colic from stones, polyuria, haematuria • Bone pain • Abdominal pain • Symptoms of underlying cause e.g. malignancy often advances with bone metastases The Peer Teaching Society is not liable for false or misleading information… Hypercalcaemia Investigations: Biochemistry: • Serum PTH • ABG • Renal function • 24hr urinary calcium • Alk Phos Imaging: • Abdo Xray • DEXA bone scan • PTH imaging The Peer Teaching Society is not liable for false or misleading information… Cause 1: Hyperparathyroidism Primary Hyperparathyroidism: Usually caused by parathyroid adenoma or more rarely carcinoma or hyperplasia PTH Calcium Phosphate PTH Appropriate? ↑ ↑ ↓ X Treatment: No effective medical therapies at present, high fluid intake should be maintained, a high calcium and vit D intake avoided and exercise encouraged. The Peer Teaching Society is not liable for false or misleading information… Cause 1: Hyperparathyroidism Secondary Hyperparathyroidism: Physiological compensatory hypertrophy, secondary to hypocalcaemia, e.g. CKD, vit D deficiency PTH Calcium Phosphate PTH Appropriate? ↑ ↓ ↓ ✔️ Treatment: Medical treatment is the mainstay, the underlying condition needs treating. Treatment in CKD includes phosphate binders, calcium supplementation, vit D and calcimimetics. The Peer Teaching Society is not liable for false or misleading information… Cause 1: Hyperparathyroidism Tertiary Hyperparathyroidism: Autonomous parathyroid hyperplasia after longstanding secondary hyperparathyroidism, usually due to renal failure PTH Calcium Phosphate PTH Appropriate? ↑ ↑ ↑ X Treatment: Calcimimetics may be used. Total or subtotal parathyroidectomy is the recommended treatment. The Peer Teaching Society is not liable for false or misleading information… Cause 2: Malignancy Lytic bone metastases, myeloma or activation of osteoclast activating factor by the tumour PTH Calcium Phosphate PTH Appropriate? ↓ ↑ -- ✔️ Raised alk phos… indicates ↑ bone turnover, probably due to metastases Treatment: • Manage malignancy • IV bisphosphonates or calcitonin The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia Causes: • Increased phosphate (CKD or phosphate therapy) • Vitamin D deficiency (osteomalacia) • Hypoparathyroidism (post surgery, DiGeorge syndrome, severe hypomagnesiaemia) • Pseudo hypoparathyroidism – end organ PTH resistance • Drugs – bisphosphonates, calcitonin • Acute pancreatitis The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia Features: • Paraesthesia • Circumoral numbness • Cramps • Anxiety • Tetany If severe: • Convulsions • Laryngeal stridor • Dystonia • Psychosis • Papilloedema • Long QT Chvostek’s sign Trousseau’s sign The Peer Teaching Society is not liable for false or misleading information… Hypocalcaemia/Hypoparathyr oidism Investigations: • Clinical history is usually sufficient • Confirmed by low serum calcium • PTH level, PTH antibodies, renal function, vit D level, magnesium Treatment: • Vit D deficiency – give vit D3 • Oral calcium supplements • Hypoparathyroidism – calcium & vit D The Peer Teaching Society is not liable for false or misleading information… Hypokalaemia Causes: Acute – IV fluids without potassium, as the potassium enters the cells Chronic – Diuretics, hyperaldosteronism, drugs (mineralocorticoids, steroids), renal tubular acidosis, insulin treatment, vomiting, severe diarrhoea, villous adenoma, intestinal obstruction Features: Usually asymptomatic. If severe – muscle weakness and symptoms of hyponatraemia Increased frequency of ectopic beats in patients with heart disease The Peer Teaching Society is not liable for false or misleading information… Hypokalaemia Treatment: • Identify and treat underlying cause Dietary deficiency increase fruit and veg intake/ supplements Hyperaldosteronism spirinolactone & amiloride IV fluid replacement add potassium to fluid • Acute cases may resolve spontaneously • Withdrawal of diuretics or purgatives, alongside potassium supplements is usually all that is required • IV replacement, only in cardiac arrhythmias, muscle weakness or severe DKA – cardiac monitoring! The Peer Teaching Society is not liable for false or misleading information… Hyperkalaemia Causes: • Acute, self limiting hyperkalaemia appears after vigorous exercise • Decreased excretion: AKI, K sparing diuretics, ACE-I, NSAIDs, Addison’s • Increased cellular release: acidosis, digoxin toxicity, vigorous exercise The Peer Teaching Society is not liable for false or misleading information… Hyperkalaemia Features: • Serum K >7.0 mmol/L is a medical emergency, associated with ECG changes (tall tented T waves, wide QRS, flattened P waves) • Often aysmptomatic but may predispose to sudden death from cardiac arrest • Muscle weakness is often only symptom • May have Kussmaul breathing if acidotic • Hypotension/bradycardia The Peer Teaching Society is not liable for false or misleading information… Hyperkalaemia Treatment: • Illicit cause and treat • Immediate treatment – calcium gluconate and IV insulin + dextrose infusion • Deplete body K stores through polystyrene sulphonate resins with laxatives or an enema • Dialysis The Peer Teaching Society is not liable for false or misleading information… MEN MEN – Multiple endocrine neoplasia • Rare, inherited condition causing hormone secreting tumours • 2 types: 1 & 2 Type 1 • Diagnosis: More than 2 neuroendocrine tumours, plus the genetic mutation • Symptoms depend on tumour, gland involved, and hormones secreted • 95% have parathyroid hyperplasia/adenoma • 70% have pancreatic endocrine tumours (gastrinoma, insulinoma, somatostatinoma, VIPoma, glucagonoma) The Peer Teaching Society is not liable for false or misleading information… MEN Type 2 • Medullary thyroid carcinoma seen in 100% • Phaeochromocytoma seen in 50% • Parathyroid hyperplasia in 80% Treatment • Depends on tumour type • Can involve surgery or medications to reduce the appropriate hormone level The Peer Teaching Society is not liable for false or misleading information… Malignant Carcinoid Syndrome • The constellation of symptoms typically exhibited by patients with metastases from carcinoid (neuroendocrine) tumours. • These tumours usually secret excessive amounts of serotonin. • They arise from neuroendocrine cells, especially in the intestine • Carcinoids do not produce the malignant carcinoid syndrome until they are no longer confined to the small bowel or mesentery. They often spread to the liver. The Peer Teaching Society is not liable for false or misleading information… Malignant Carcinoid Syndrome Symptoms • Tumours grow slowly and symptoms may not appear for years • Alcohol intolerance and weight loss are common • Diarrhoea • Flushing of the face and neck • Wheezing, asthma, SOB • Palpitations, low BP, dizziness Diagnosis • Measure serotonin metabolite 5-HIAA in a 24 hr urine sample • Many foods contain serotonin which complicates the diagnosis • Imaging: Barium swallow, MIBG, CT, angiography and venous blood sampling The Peer Teaching Society is not liable for false or misleading information… Malignant Carcinoid Syndrome Treatment • Interferons and octreotide may help control humorally mediated symptoms. • Histamine blockers may be helpful • Serotonin antagonists can help control diarrhoea and malabsorption • Somatostatin may be helpful in preventing flushing • Complete surgical removal of all tumour tissues is the best treatment The Peer Teaching Society is not liable for false or misleading information… Quiz Which cells in the pancreas secrete insulin? And glucagon? Which immune cell mediates the AI response leading to T1DM? Name 2 conditions associated with T1DM The Peer Teaching Society is not liable for false or misleading information… Quiz 2 causes of DKA Name the type of breathing seen in DKA Emergency treatment of DKA The Peer Teaching Society is not liable for false or misleading information… Quiz Above what level does a random glucose need to be to diagnose diabetes? Why is acidosis present in DKA, but not HHS? 3 symptoms of hypoglycaemia How would you treat hypoglycaemia in an unconscious patient without IV access? The Peer Teaching Society is not liable for false or misleading information… Quiz In which type of retinopathy do you have new blood vessel formation? Does thyroxin mostly circulate as T3 or T4? What are the 2 specific eye signs found in graves disease? The Peer Teaching Society is not liable for false or misleading information… Quiz What is the anti thyroid hormone medication called? Where in the adrenals is cortisol produced? 48 hour low dose dexamethasone test, ACTH remains unchanged, do you scan pituitary or adrenals? The Peer Teaching Society is not liable for false or misleading information… Quiz Which hormone is produced in excess in Conn’s syndrome? Why in adrenal insufficiency secondary to hypothalamic pituitary disease do you have insufficient cortisol, but adequate aldosterone? 2 drug treatments for Addison’s (long term) The Peer Teaching Society is not liable for false or misleading information… Quiz Name 1 systemic disease that phaeochromocytoma is associated with. Pre-surgical treatment of phaeochromocytoma requires which 2 medications, in which order? What is the plasma and urine osmolality in diabetes insipidus? (high/low)? The Peer Teaching Society is not liable for false or misleading information… Quiz Through which route do you give desmopressin for DI? Which drug can be used in SIADH which promotes water excretion without loss of electrolytes? Which hormone counteracts the action of GHRH? The Peer Teaching Society is not liable for false or misleading information… Quiz What is the commonest cause of acromegaly? 2 signs of acromegaly? 2 drugs used to treat acromegaly? The Peer Teaching Society is not liable for false or misleading information… Quiz Which cells in the parathyroid secrete PTH? In primary hyperPTH is phosphate high or low? Is the PTH level appropriate in secondary hyperPTH? The Peer Teaching Society is not liable for false or misleading information… Quiz Name 2 causes of hypocalcaemia Which sign of hypocalcaemia is elicited by inflating a blood pressure cuff around the upper arm? What is the emergency treatment of acute hyperkalaemia? The Peer Teaching Society is not liable for false or misleading information… Quiz What are the ECG changes associated with hyperkalaemia? Which hormone is excessively secreted in malignant carcinoid syndrome? 2 symptoms of this condition The Peer Teaching Society is not liable for false or misleading information…