Scrotum Pathology
advertisement

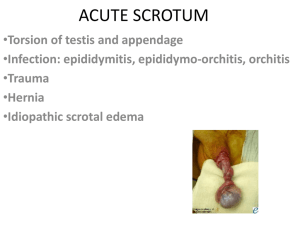
SCROTUM PATHOLOGY Hydrocele May be primary or secondary An abnormal collection of serous fluid between the two layers of tunica vaginalis. Scrotal calcification often seen The ultrasound image on the left demonstrates a normal tunica vaginalis surrounding the testis. On the right, the left testis is surrounded by a hydrocele. Notice the parietal layer of the tunica vaginalis apposed to the testis and the large fluid filled space and parietal layer. This is a large hydrocele, which is only partially demonstrated on this view. http://www.ceessentials.net/images/ultrasoundTestes/image022.jpg Primary hydrocele o Congenital hydrocele caused by the failure of the processus vaginalis to close by the end of the first year of life. o An idiopathic hydrocele, no apparent cause for the hydrocele in the adult. Secondary hydrocele o Usually exists secondary to an infection, trauma or tumour. o May present with debris or septum. o differential diagnosis: pylocele Spermatocele Haematocele Varicocele Abnormal dilation and tortuosity of the veins of the pampiniform plexus. the vessel diameter is increased when over 2mm.(3mm) may be primary or secondary Left ultrasound image demonstrates engorged veins of a varicocele using the “valsalva maneuver to increase intravenous pressure. The ultrasound image on the right demonstrates these small anechoic lesions that are generally greater than 2 mm. http://www.ceessentials.net/images/ultrasoundTestes/image028 a & b.jpg Primary (idiopathic) o Due to incompetent valves of the spermatic vein which allow blood to flow back into the pampiniform plexus. o It is a common cause of infertility and predominately occurs of the left side. Secondary o Due to increased external pressure on the spermatic vein, or tributaries. o The cause maybe renal, abdominal neoplasm or a retro peritoneal mass. o If a new varicocele is detected on the right and is not decompressable an extension of the examination is made to try and find the cause of compression. Epidermoid Cyst (can be present in other areas) Usually presents as a painless mass or nodule. It is a rare benign tumour. Ultrasonically an epidermoid cyst is a well circumscribed hypoechoic mass with internal echoes, often described as concentric rings of alternating echogenicity. There typically is an echogenic capsule, which is smooth walled. No vascularity detected. The remainder of the testis has a normal ultrasound appearance Scrotal Hernia herniation of the abdominal contents, caused by the failure of the peritoneal pouches to obliterate, communication remains between the peritoneal sac and tunica vaginalis. Scrotal hernias may contain peritoneum, intestine or omentum. The patient usually presents with pain and swelling. These ultrasound images show echogenic, linear/ tubular structures (intestine) within the left scrotal sac, just above the left testes, extending to the left inguinal canal s/o left inguinal hernia. http://www.ultrasound-images.com/admin/uploads/inguinal-hernia-3b.jpg On ultrasound there maybe evidence of extension of a mass through the inguinal canal especially with movement, (ie valsalva). Adenomatoid Tumour Is the most common extra testicular tumour. Usually arises in the epididymal head but can present elsewhere in the epididymis, testicular tunica or the spermatic cord. Generally a painless mass over 5mm, on ultrasound it is usually a well defined solid mass which is separate to the testis. it has a varied echogenic appearance and maybe homogenous, hyperechoic or hypoechoic with respect to the testis. Vascularity within the lesion maybe identified. Tail of the epididymis shows a well circumscribed hypoechoic mass http://imagingsciencetoday.com/sites/default/files/styles/galleryformatter_slide/public/ figure21207483392312.jpg Intratesticular Cyst Usually presents as a solitary lesion adjacent to the mediastinum. The size is variable and it offers the usual typical cyst appearance, anechoic, posterior enhancement, thin walled and a well defined border. Sagittal image of the left testicle demonstrates ectasia of the rete testes (solid arrow) with intratesticular cysts (dashed arrow). http://www.mghradrounds.org/clientuploads/march_2006/us_scrotum.jpg Epididymal Cysts Cystic lesions on the epididymis are very common. two main types which are undistinguishable with ultrasound 1. spermatoceles- usually single, often associated with infection or trauma 2. epididymal cyst- maybe multiple Both are common in the epididymal head. http://www.ewingurologyclinic.co.uk/images/NewImages/XRaySlides/Epididy malCyst01LG.jpg Sperm Granuloma Clinically present as a painful area at the site of previous surgery (vasectomy) or trauma. Ultrasound presentation is of rounded solid hypoechoic mass/es adjacent or within the epididymis. They are believed to be caused by the leakage of sperm into the surrounding tissues. Sperm granuloma with a hypoechoic non vascularized round mass in the epididymal tail http://www.ultrasoundcases.info/files/Jpg/20942.jpg Scrotal abscess Ultrasound presentation is of a hypoechoic complex fluid collection containing low level echoes. may occur due to: 1. A complication of epidiymo-orchitis common in diabetics missed testicular torsion, infected haematoma. 2. systemic infection eg; mumps, influenza, tb 3. Septic dissemination from sinusitis, appendicitis. Color Doppler imaging imaging confirm marked increase in vascularity around both lesions suggesting marked hyperemia http://www.ultrasound-images.com/admin/uploads/TESTES-ABSCESS-1d.jpg Testicular torsion extravaginal torsion occurs in newborns possibly due to the motility of the entire vaginalis intravaginal torsion, occurs more commonly especially around puberty. Torsion occurs due to the rotation of the testis around the long axis of the spermatic cord. Torsion maybe complete or recurring. Presentation is of sudden severe pain with scrotal swelling and tenderness, often with associated nausea and fever. May present after extreme exertion or trauma. It is extremely painful and requires urgent surgical intervention to salvage the testis as no significant collateral circulation exists. The arterial and venous supply maybe interrupted which can lead to ischaemia and haemorrhagic necrosis. Torsion may occlude only the venous supply not the artery. Ultrasound appearance varies, depending on the time of presentation. These two transverse ultrasound images demonstrate the normal blood flow through the left testicle. http://www.ceessentials.net/images/ultrasoundTestes/image018.jpg On color doppler imaging, the left testes shows absence of blood flow. The "snail sign" is also seen in the left testes, caused by swollen testes (shell of snail) and twisted, bulky spermatic cord (body and head of snail). http://www.ultrasound-images.com/admin/uploads/torsion-testes-1a.jpg Early presentation the testis and epididymis may have normal ultrasound appearance. The testis may appear enlarged, the epididymis may appear enlarged, the skin maybe oedematous and a hydrocele maybe present. Colour Doppler To aid in the diagnosis of testicular torsion we are looking for an absence of testicular flow. There maybe flow within the epididymis; this does not exclude testicular torsion. Always compare the flow within the unaffected testis, this will provide a good baseline for the colour sensitivity levels. Incomplete torsion may still present with some intratesticular flow. Torsion of the appendix testis is extremely painful and presents on ultrasound as a hyperechoic or hypoechoic mass with absent blood flow adjacent to the normal testis (normal perfusion) usually situated between the testes and epididymal head. Malignant Testicular Tumours 90% of testicular cancer begins in the germ cells; there are two types of germ cell tumours, o Seminomas o nonseminomas. seminomas make up 40% of all testicular germ cell tumours. Non seminomas are a group of cancers that include choriocarcinoma, yolk sac tumours, embryonal carcinoma and teratoma. They are usually an aggressive testicular tumour. Seminoma o usually in the 30 - 40 age group o Ultrasound demonstrates a solid mass with hypoechoic texture, maybe well defined and contained within the tunica albuginea. o An increased incident is noted with a patient history of undescended testis. abnormal hypoechoic left testicle when compared with the right. There are bilateral small hydroceles (h). https://www.meded.virginia.edu/courses/rad/gu/malepelvis/Images/seminomaleftvsright.jpghttps://www.meded.virginia.edu/courses/rad/gu/malepelvis/Images/seminomaleftvsright.jpg Embryonic cell o more aggressive than seminomas, occur in the 20 -40 age group, o Ultrasound demonstrates a solid irregular mass, with cystic degeneration and echogenic foci not usually contained by the tunica albuginea. o Frequently metastases. Choriocarinoma o Rare, but highly malignant with a peak incidence in the 20- 40 age group. o Metastases quickly. o Present sonographically with a mixed echogenicity due to necrosis, calcification may be present. Heterogenous solid cystic mass lesion in left testes. http://images.radiopaedia.org/images/629104/fbe0340f833e86334f1aa67d1fd755.jpg Teratoma o Two peak age groups: infancy and early childhood and 30’s age group. o Childhood teratomas usually benign. o Adult teratomas are generally malignant. With metastases to the lymph,bone and liver. o Ultrasound demonstrates an irregular solid mass containing cystic and, solid components. Echogenic calcification is often present. multiple cystic areas (arrow) measuring 2-15 mm. Cystic areas involved nearly the entire testis, leaving only a rim of normal testicular parenchyma (arrowhead). http://radiology.rsna.org/content/227/1/18/F23.medium.gif Non germ cell tumours o peak age of 20-50, o ultrasound presentation is of a usually small solid mass which maybe hypoechoic and may contain cystic components, examples are; leydig cell tumour; benign:malignant 9:1 (radiology review manual) sertoli cell tumour;generally benign ( radiology review manual) gonadoblastomas Metastatic disease o Malignant lymphoma is the most frequently encountered metastatic testicular disease. o It maybe bilateral. o Leukemia is the next most common metastaic neoplasm. o Lung and prostate,bladder,melanoma primary neoplasms will metastases to the testis, often multiple and bilateral. o childhood – neuroblastoma Testicular calcification Extra testicular o o o o More frequently encountered than intra testicular Usually associated with benign findings Often a solitary finding Tunica Vaginalis may calcify – linear calcification, scrotal pearl- loose body between membranes of Tunica Vaginalis o Calcification in or adjacent to epididymis is thought to be associated with chronic epididymitis ( a differential for this = granulatomas) o A haematoma or sperm granuolma- solitary echogenic focus within the epididymis Scrotal phlebolith or scrotal calculus with a mobile calcified structure with minor acoustic shadowing http://www.ultrasoundcases.info/files/Jpg/4243.jpg Tunica vaginalis or tunica albuginea calcification http://www.ultrasoundcases.info/files/Jpg/13936-11765.jpg Intra testicular o Testicular Microlithiasis- multiple scattered echogenic foci within the testis, usually between 1-3mm. The pattern and distribution may be variable. Aoustic shadowing usually not identified. Benign and malignant associations. o A cluster of calcifications seen within a hypoechoic area is a significant finding associated with chronic testicular infarction or testicular carcinoma. o A large calcified scar may signify a burnt out tumour. o Calcification associated with malignant tumours discussed under individual headings. o Phleboliths- benign calcification o Vascular calcification ultrasound images are diagnostic of testicular microlithiasis. Microlithiasis of testes is associated with higher incidence of intratubular germ cell neoplasia of testes and other tumors of this organ. http://www.ultrasound-images.com/admin/uploads/testes-microlithiasis-2d.jpg