Forbes_-_Tracts_chart
advertisement

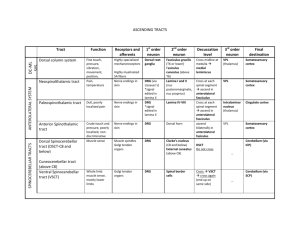
Tracts that indirectly influence LMNs: Cortico-ponto-cerebellar tract Cerebello-rubro-thalamocortical tract Corticorubrospinal tr Inferior olivary nucleus Cerbral cortex communicates with contralateral cerebellum -Afferent -Cerebellum learning about muscles Cerebellum indirectly influences motor control -Efferent -Feedback In cats Descending pyramidal: Skilled voluntary movements; piano, typing. Terminate on motor and sensory neurons, motor is more important. Effects concentrated on UMNs in hands, otherwise lots of interneurons. Little effect on posture and background muscle tone. MOTOR Corticospinal tract: LCST -All SC levels -Innervates limbs VCST -Only to thoracic lvls -Innervates axial musc. -Decussates @ lvl of termination in anterior white commissure Corticobulbar tract: -Cerebral cortex -White matter of cerebral cortex -Internal capsule -Cerebral crus -Basilar pons -Pyramid -Pyramidal decussation (X) -Lateral column of cord -Gray matter of cord terminates on LMNs (in ventral/anterior horn) or interneurons. CONTRA - Dorsal CST more significant than ventral CST. -Cerebral cortex -White matter of cerebral cortex -Internal capsule -Cerebral crus (X) -Basilar pons (X) -Pyramid (X) Terminate bilaterally on all levels of brainstem (bulb) -Facial motor nuclei get contralateral corticobulbar input only. Somatotopy: Legs are Lateral in LCST & ST. DCML is organized as you are (hands at side – arms outside, legs inside) LLS C U TT DCML LCST SLTC SL T C ST Lesions: LMN lesions = lowered! muscle mass, muscle tone, reflexes, downgoing toes (no Babinski) UMN lesions = up! muscle tone, DTRs, toes up (+ Babinski) Other supraspinal descending: Maintain posture, muscle tone, gross muscle activities. Excitatory and in hibitory effects on LMN balance eachother. B/C NO direct connection between cerebellum & LMNs Vestibulospinal tract Reticulospinal tract (RST) (medial and lateral) CEREBELLAR Raphe spinal tract Medial longitudinal fasciculusMLF (med. vestibulospinal tr.) -Runs w/ VST -posture & balance -MS pts = diplopia Intersegmental fibers: In spinal cord are essential for coordinating spinal reflexes that involve multiple Fasciculus Proprius cord segments. Septomarginal tract Fasciculus interfascicularis Cerebellum influences LMNs; upright posture, balance. Gymnastics, diving. Descending autonomics. Cerebellum influences LMNs; posture, muscle tone. Segmental spinal cord integration; walking, running. SOMATIC motor control. Modulates pain by mimicing opium alkaloids. Medullary reticular formation origin. Terminates in substantia gelatinosa. Coordinates head and eye movements related to equilibrium. Ascending to CN III, IV, VI nuclei. Descending to cervical levels of ventral horn. Input from vestibular nuclei. Damage to MLF causes lack of coordination of eye movements. - intranuclear opthalmoplegia damage to MLF incoordination of eye movements, esp medial- lateral ipsilateral eye can’t move past midline Immediately surrounds the gray matter. Ascends and descends, fibers vary in length. Descending branches of large diameter dorsal root primary afferents. Descending branches of large diameter dorsal root primary afferents. ASCENDING: Spinocerebellar: -Large diameter 1’ afferents, unconscious proprioception, sensory, intimate association with motor control. -Medial division dorsal root 2 Neurons! Dorsal spinocerebellar tract: DSCT Cuneocerebellar tract: CCT Ventral spinocerebellar tract: VSCT 1’ lower extremity input 1’ cell body in DRG 1’ axons in fasciculus gracilis 2’ cell body in Clark’s nuclues Uncrossed Ipsilateral input to cerebellum ICP 1’ upper extremity input 1’ cell body in DRG 1’ axons in fasciculus cuneatus 2’ cell body lat cuneate nucleus Uncrossed Ipsilateral input to cerebellum ICP 1’ lower extremity input 1’ cell body in DRG 1’ axons in fasciculus gracilis 2’ cell body base of ventral horn Crosses and recrosses Primarily ipsilateral input to cerebellum SCP Ascending SENSORY Anterolateral Ascending: Spinothalamic: 3 Neurons! Raphe runs w/ ST (PAIN) Spinoreticular Spinotectal Dorsolateral Ascending: Dorsal column medial leminiscus 3 Neurons! F. gracilis – input from mid thoracic and below F. cuneatus – input from mid thoracic and above Lesions: ST: Loss of Pain & Temp / 2 segments below lesion / CONTRA DCML: Loss of discriminative touch, conscious proprioception & vibration / Below level of lesion / IPSI if in SC & CONTRA if above nuc g/c Consious awareness of pain and temperature. 1’ input from small afferent fibers associated with free nerve endings. 1’ cell body in DRG Enters through the lateral division of the dorsal root. Ascend 1-2 segments in Lissauer’s tract. 2’ cell body in ipsilateral dorsal horn Decussation in ventral white commissure 3’ thalamus (CONTRA) Indirect transmission of pain. Ascending reticular activation system and level of consiousness. Alternate route to cerebellum and brainstem. Conscious awareness of discriminative touch, pressure, proprioception, vibration. 1’ input from large afferent fibers associated with sensory receptors. 1’ cell body in DRG Enters through the medial division of dorsal horn 2’ cell body in cuneate or gracilis nucleus Decussation in internal arcuate fibers of medial leminiscus 3’ thalamus