Applied anatomy of thorax
advertisement

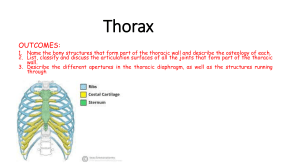
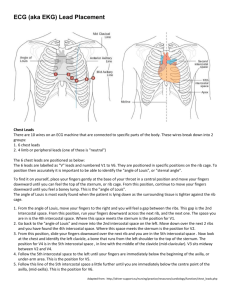
DR. ARAVINDAKSHAN.G.K. APPLIED ANATOMY OF THORAX The following bony prominences can usually be palpated in the living subject: • superior angle of the scapula (T2) • upper border of the manubrium sterni, the suprasternal notch (T2/3) • spine of the scapula (T3) • sternal angle (of Louis)— the transverse ridge at the manubrio-sternal junction (T4/5) • inferior angle of scapula (T8) • xiphisternal joint (T9) • lowest part of costal margin—10th rib (the subcostal line passes through L3). • The manubrium corresponds to the 3rd and 4th thoracic vertebrae and overlies the aortic arch, and that the sternum corresponds to the 5th to 8th vertebrae and neatly overlies the heart. • The spinous processes of all the thoracic vertebrae can be palpated in the midline posteriorly, but it should be remembered that the first spinous process that can be felt is that of…. C7 (the vertebra prominens). • The position of the nipple varies considerably in the female, but in the male it usually lies in the 4th intercostal space about 4in (10cm) from the midline. • The apex beat, which marks the lowest and outermost point at which the cardiac impulse can be palpated, is normally in the left 5th intercostal space 3.5in (9cm) from the midline (just below and medial to the nipple). • The trachea is palpable in the suprasternal notch midway between the heads of the two clavicles. It commences in the neck at the level of the lower border of the cricoid cartilage and runs vertically downwards to end at the level of sternal angle of Louis. The Ribs The chest wall of the child is highly elastic and therefore fractures of the rib in children are rare. The Intercostal Spaces CHEST WALL The sternum and the marrow biopsy. Under a local anesthetic, a wide-bore needle is introduced into the marrow cavity through the anterior surface of the bone. The sternum may also be split at operation to allow the surgeon to gain easy access to the heart, great vessels, and thymus. THE RIBS 1. Rib fractures. 2. Cervical rib. 3. Rib excision. 4. Rib Contusion. THE INTERCOSTAL NERVES 1. Skin Innervation of the Chest Wall and Referred Pain. 2. Herpes Zoster. 3. Area of Anesthesia. Thoracic Vertebrae • Fractures of the spine most commonly involve T12. • The cause is usually a flexion– compression type of injury (for example, a fall from a height landing on the feet or buttocks, or a heavy weight falling on the shoulders), • If, in addition to compression, there is forceful forward movement, one vertebra may displace forward on its neighbour below with either dislocation or fracture of the articular facets between the two and with rupture of the interspineous ligaments. • Moreover the bodies of T5 & T8 are worth nothing; and have relation with the descending aorta. If the descending aorta becomes aneurysmally dilated, these four vertebral bodies become eroded by its pressure. COSTAL CARTILAGES 1. Chest Cage Distortion. 2. Chest Trauma. 3. Flail Chest. 4. Fractured Sternum. 5. Traumatic Injury to the Back of the Chest. 6. Traumatic Injury to the Chest and Abdominal Viscera. The Diaphragm The diaphragm is the dome shaped septum dividing the thoracic from the abdominal cavity. has two portions 1. peripheral muscular. 2. centrally placed aponeurosis. The Diaphragm • Openings in the diaphragm The three main openings in the diaphragm are: – 1 the aortic (at the level of T12) which transmits the abdominal aorta, the thoracic duct and often the azygos vein – 2 the oesophageal (T10) which is situated between the muscular fibres of the right crus of the diaphragm and transmits, in addition to the oesophagus, branches of the left gastric artery and vein and the two vagi – 3 the opening for the inferior vena cava (T8) which is placed in the central tendon and also transmits the right phrenic nerve. THE DIAPHRAGM 1. 2. 3. 4. 5. Hiccup. Paralysis of the Diaphragm. Penetrating Injuries of the Diaphragm. Rupture of the Diaphragm. Acquired Herniae. THE CLAVICLE AND ITS RELATIONSHIP WITH THE THORACIC OUTLET 1. The Thoracic Outlet Syndromes. Disappearance or re-duction of the pulse, and possibly coldness and paleness of the hand, would indicate that the subclavian artery is being compressed by the scalene muscles and/or the first (or cervical) rib. THE BREASTS 1. Witch’s Milk in the Newborn. 2. Supernumerary and Retracted Nipples. 3. CA of breast. 4. Polythelia. 5. Micromastia. 6. Macromastia. 7. Gynecomastia. THE MEDIASTINUM A space in which is sandwitched in between the two pleural sacs. THE MEDIASTINUM • Deflection of Mediastinum. • Mediastinitis. • Mediastinal Tumors or Cysts. The pleura • The cervical pleura can be marked out on the surface by a curved line drawn from the sternoclavicular joint to the junction of the medial and middle thirds of the clavicle; the apex of the pleura is about 1 in (2.5cm) above the clavicle. • The lines of pleural reflexion pass from behind the sternoclavicular joint on each side to meet in the midline at the 2nd costal cartilage (the angle of Louis). The right pleural edge then passes vertically downwards to the 6th costal cartilage and then crosses: • the 8th rib in the midclavicular line; • the 10th rib in the midaxillary line; • the 12th rib at the lateral border of the erector spinae. • On the left side the pleural edge arches laterally at the 4th costal cartilage and descends lateral to the border of the sternum, due, of course, to its lateral displacement by the heart. THE PLEURA • • • • • • • • • • Pleural Fluid. Pleurisy. Pneumothorax. Haemothorax. Empyema. Pluritis. Hydropneumothorax. Pyopneumothorax. Hemopneumothorax. By a stab wound or surgical wound. sternum 1. Injury 2. Aspiration for the bone marrow specimen. 3. Operations on the thymus gland The intercostal spaces 1. Local irritation of intercostal nerves by such conditions as Pott’s disease. 2. Intercostal nerve block. 3. Thoracotomy. trachea 1. 2. 3. 4. Tracheal tug. Tracheostomy. Tracheal displacement. Radiological findings. The lungs • The apex of the lung closely follows the line of the cervical pleura and the surface marking of the anterior border of the right lung corresponds to that of the right mediastinal pleura. • On the left side, however, the anterior border has a distinct notch (the cardiac notch) which passes behind the 5th and 6th costal cartilages. • The lower border of the lung has an excursion of as much as 2–3in (5–8cm) in the extremes of respiration, but in the neutral position (midway between inspiration and expiration) it lies along a line which crosses the 6th rib in the midclavicular line, the 8th rib in the midaxillary line, and reaches the 10th rib adjacent to the vertebral column posteriorly. • The oblique fissure, which divides the lung into upper and lower lobes, is indicated on the surface by a line drawn obliquely downwards and outwards from 1in (2.5cm) lateral to the spine of the 5th thoracic vertebra to the 6th costal cartilage about 1.5in (4cm) from the midline. • The line of the oblique fissure then corresponds to the position of the medial border of the scapula. • The surface markings of the transverse fissure (separating the middle and upper lobes of the right lung) is a line drawn horizontally along the 4th costal cartilage and meeting the oblique fissure where the latter crosses the 5th rib. Clinical Anatomy of Lung • Usually, the infectn of a segment remains restricted to it, although some infections like TB, may spread one segment to another. resection of a bronchopulmonary seg. removal of one lobe- Lobectomy removal of whole lung - Pneumonectomy • Tumour of upper lobe of lung causes certain press. Effects -venous engorgement & oedema of face & upper limb -Diminished pulse -Paralysis of the cupola -Hoarseness of voice etc. • Breath sounds from the upper lobe are best heared infront & those from the lower lobe best heared on the back. • The middle lobe does not reach the chest wall behind & auscultated infront b/n 4th and 6th ribs. • Breath sounds from all lobes are heared along the mid-axillary line. • Ds.s, such as silicosis, asbestosis, cancer and pneumonia interfere with the process of expanding the lung in inspiration. bronchi 1. Aspiration of foreign bodies. 2. Widening & distortion of the angle between the bronchi.