OB/Gyn Grand Rounds: What Can the
advertisement

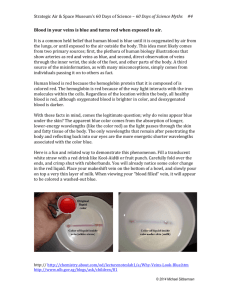
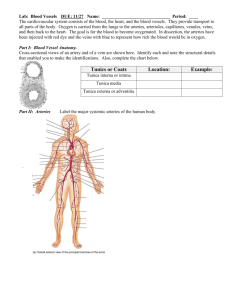
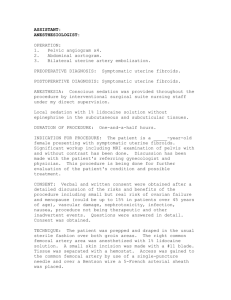
OB/Gyn Grand Rounds: What Can the Interventionalist Do for Your Patients Thea Moran, MD Asst Professor Louisiana State University New Orleans, LA Disclosures • I have no disclosures to make What can the IR do for the OB/Gyn service? • • • • • • 1. Uterine fibroid embolization 2. Nonfibroid uterine artery embolization 3. Prepartum uterine artery embolization 4. Pelvic congestion syndrome 5. Fallopian tube recanalization 6. Endovenous ablation of varicose veins 1. Uterine fibroid embolization • Fibroids, or leiomyomas, are benign smooth muscle tumors of the uterus occurring in reproductive age women. • Most common benign tumors of the female genital tract although many are without symptoms • Fibroids are most frequent in 30-40 year olds and involute after menopause • Goal of UFE is selective infarction of symptomatic fibroids Symptoms • Menstrual abnormalities – Menorrhagia • Most frequent indication • Symptom most responsive • DDX: adenomyosis, endometrial polyps, endometrial hyperplasia, endometrial CA – Menometrorrhagia – Worsening of menstrual cramps • Pressure symptoms – Pressure sx related to the bladder, ureter, bowel, or nerves – DDX: ovarian and abdominal masses, infection, endometriosis, adenomyosis; fibroid torsion, degeneration or prolapse; PID, endometriosis, adenomyosis, pelvic congestion syndrome, GU/MSK/GI causes Symptoms • • • • Dyspareunia Increasing pelvic or abdominal girth Needed premyomectomy, hysterectomy for fibroids Infertility or miscarriages with no other discernible cause – Controversial Contraindications • • • • • • • • • Severe anaphylactoid reaction to contrast Uncorrectable coagulopathy Severe renal insufficiency Pregnancy Gynecological malignancy Active pelvic infection/inflammatory disease Prior pelvic radiation Microvascular disease Pedunculated or mucosal fibroids – Expulsion, cervical impaction Uterine artery anatomy • First branch of anterior division of internal iliac artery • 3 segments • Descending segment goes along pelvic wall • Transverse segment goes to the midline • Ascending segment along the uterus Uterine artery anatomy • Cervicovaginal artery • Perforating arteries, terminal branches to the fallopian tubes and ovaries • Inferior vesicle artery has common origin • Can have completely or partially absent uterine artery which can be bilateral Uterine artery anatomy Ovarian artery anatomy • 1 ovarian artery per ovary • Originate from aorta a few cms below renal artery origins • 4% of women have ovaries supplied 100% by the uterine artery – Nikhil C Patel, Interventional Radiology Secrets. Ovarian artery anatomy • 46% have uterine-ovarian artery anastomoses * • 5-10% have angio vis anastomoses * – Ovarian blush – Avoid nontarget embolization • Normal diameter: 1 mm • * Nikhil C Patel, Interventional Radiology Secrets Uterine-ovarian anastomosis Preoperative work up • History, pelvic exam, informed consent • CBC, FSH (day 3), chem 7, PT/PTT/INR • Pelvic US – Usually for screening and sufficient – Uterine and fibroid volumes, fibroid position • Pelvic MRI – Better definition of fibroids, uterus c/w US, evaluate for adenomyosis and other pathology – CE MRA help planning of UFE • Demonstrates vascular supply to fibroids • PAP smear – R/o cervical CA Preop work up • Endometrial biopsy – R/o endometrial cancer – US and MRI can’t definitively evaluate endometrial thickness – Intermenstrual or irregular bleeding, postmenopausal women with vaginal bleeding – All women over 40 yo with menorrhagia • D/c GnRH analogues several weeks preop – Fibroids enlarge Patient consultation • Does the patient desire future childbearing? • Weigh treatment options • Severity of symptoms severe enough physically and/or psychologically to warrant invasive therapy especially since most fibroids involute after menopause Treatment options • Medical – NSAIDS, OCP • Mild symptoms – GnRH • Moderate symptoms • Decreases estrogen which causes fibroid degeneration after 3 months of therapy • Noninvasive, short term relief of symptoms, good for perimenopausal women, adjuvant therapy preoperatively • Not to be given indefinitely • Surgical – Severe symptoms – Open, laparoscopic or hysteroscopic techniques • Hysterectomy – Complete cure, r/o possibility of future neoplasm, facilitates postmenopausal HRT, invasive Treatments options • Myomectomy – Preserves uterus and future childbearing – Bleeding c/o if multiple fibroids – High recurrence rate (20-25%) » Nikhil C Patel, Interventional Radiology Secrets. • UFE – Severe symptoms – Uterus retained, all myoma treated at once, noninvasive – Postembolization syndrome, potential for contrast reaction, possibility of no symptom relieve and lack of comparative data – No conclusive data on the effect of this treatment on fertility Patient preparation • • • • • Usually needs at least a 23 hr admit Serum pregnancy test Foley catheter Vigorous hydration Prophylactic antibiotics – Cefazolin 1 g; if PCN allergic – vancomycin 1 g IV • Antiemetic and pain meds given • PCA pump instructions given • Have intraprocedural meds available – Conscious sedation, toradol, zofran Procedure • • • • Both groins prepped with CFA access Pelvic angiogram with catheter inferior to the renal artery Selective uterine artery angiogram Superselective angiogram with catheter tip in the transverse portion of the uterine artery past the cervicovaginal branch • Embolic agent injected – Ivalon/PVA/Biospheres 700 um – Inject until stasis w/o hypervascularity – Avoid reflux, nontarget embolization – Preserve flow in the main uterine and ovarian arteries – +/- f/u with Gelfoam plug in uterine artery • More consistently associated with preserved fertility • Control angiogram • Repeat procedure on opposite side followed by pelvic angiogram Postprocedure management • Pain management! – Severe for 12-24 hrs with gradual decrease over 7 d – Usually needs a PCA pump initially – Antipyretics, antiinflammatory meds and antiemetics • Vigorous hydration until po intake is adequate • OK to d/c patient when po intake adequate and pain control via po meds – Nothing in vagina for 3 wks – Call MD if F/C, foul smelling d/c, worsening pain, other signs of infection Results • • • • • • Less blood loss, shorter hospital stay, fewer major complications Technical success rate 98% * 90% need no further treatment * 85% improvement in bleeding symptoms * 90% improvement in mass effect symptoms * 40% decreased in fibroid and uterine size * • * Nikhil C Patel, Interventional Radiology Secrets. Complications • Postembolization syndrome – Most frequent complication (15-30%) • Nikhil C Patel, Interventional Radiology Secrets. – Pain, fever, N/V, malaise, leukocytosis – Clinically differentiated from infection • Infection: vaginal d/c or if fever, pain, malaise are progressive – Broad spectrum antibiotics, blood cultures – Acetominophen, hydration • Ovarian failure – >45 yrs • Fibroid expulsion with vaginal impaction – Submucosal fibroid – May need D&C Complications • Inadvertent sarcoma embolization – More likely to be incomplete infarction • Tumor continues to grow • No change in prognosis with 3-6 month delay • Radiation risks are minimal • PE, pain with rehospitalization, failure of procedure to correct sx • Sepsis, severe ischemia, fibroid necrosis – Most dreaded complication – Persistent fever, progressive or unrelenting abdominal pain, purulent d/c – Risk of uterine rupture – May need emergent hysterectomy • Death Postdischarge • Percocet with toradol – Analgesia, antiinflammatory, antipyretic • Compazine – Antiemetic • Stool softener – Analgesics constipate • Serum FSH 3 days after 1st period – If periods do not resume, random FSH • GYN f/u – 1-4 wks and 6 mos • Pelvic US – 3, 6 and 12 mos • +/- f/u MRI at 6 mos 2. Nonfibroid UAE • Pelvic angiogram with selective internal iliac artery angiogram pre and post embolization • Postop ie hysterectomy arterial bleeding – Extravasation, pseudoaneurysm or AVF – If localized - coil • Postpartum and tumor bleeding – Do not see extravasation or pseudoaneurysm – Tumors may appear relatively avascular • Particulates sized 3-500 um – Uterine atony • Gelfoam uterine arteries 3. Prepartum uterine artery embolization • Lessens blood loss in patients with placenta previa or accreta or an atonic uterus • Occlusion balloon catheters (Boston Scientific 8.5-11 mm) placed into each internal iliac artery from each groin predelivery on the day of the delivery – Syringe with predetermined amount of saline attached – Epidural placed beforehand • Catheter length protruding outside of patient is marked • Patient transferred to delivery room • Infant delivered • Balloons inflated • Placenta delivered 4. Pelvic congestion syndrome • Female equivalent of testicular varicocele • Dilated gonadal and periuterine veins with symptoms – Dyspareunia, menstrual abnormalities, vulvar varices, LE varicose veins – Sx worse late in the day, when upright, with sexual arousal and during menstruation. • Condition of childbearing age • Reflux of blood into the gonadal veins • More common on the left • Predisposing conditions – Prior pregnancy, nutcracker syndrome, tubal ligation, IUD Indications • Indications: – Chronic pelvic symptoms with o/w negative w/u – Pelvic varicosities with appropriate symptoms – Lower extremity varicose veins recurrent immediately after adequate surgical treatment – Severe labial/perineal varicosities • Contraindications: – Severe anaphylactoid reaction to contrast – Uncorrectable coagulopathy – Severe renal insufficiency – Phobia to medical implants – Inadequately treated pelvic pain of other cause Preprocedural preparation Assessment • Detailed clinical assessment by gynecologist • Diagnostic testing – Diagnostic laparoscopy, pelvic US, CT and/or MRI – Dilated gonadal and pelvic veins may be underestimated if patient is supine • Normal diameter of gonadal veins is <or= 5 mm • Diameter can easily >10 mm when abnormal • Clinical assessment by vascular specialist if varicose veins are the 1ary problem Dilated gonadal vein Dilated pelvic veins Patient education • Pelvic congestion syndrome is controversial • Often see dilated veins in parous women w/o sx and no dilated veins in women with sx • Not all patients respond to embolization or may take up to 6 months to respond • Most women treated with embolization experience some relief if rigorous clinical and imaging screening is employed Gonadal vein anatomy • L gonadal vein empties into LRV • R gonadal vein empties into the IVC inferior to the RRV • Many variations in anatomy and confluences • Ascend on psoas with ureters and gonadal arteries Alternative treatments • Medical management – GnRH analogs, birth control pills, pain medicines • Surgical management – Ligate ovarian veins via laparoscope – Hysterectomy Patient preparation • Timing of the procedure with respect to menstrual or pain cycle is unimportant • Outpatient • Informed consent • Peripheral IV • Conscious sedation Invasive diagnostics • • • • • • • • • • Venography is the definitive diagnostic imaging modality Jugular>femoral and basilic vein access 5-7 F sheath Catheter into peripheral left renal vein Table tilted upright to 45 degrees Contrast hand injected – Reflux, identify collaterals, renal vein pathology, variant anatomy Positive study – Patulous, easy to select vein orifices – Retrograde flow into the pelvis and uterine plexus – Slow contrast washout Move to the opposite gonadal vein If the ovarian venograms are negative - B internal iliac venograms Control injection in the renal vein after embolization Embolization • Coils are the best known and most documented – Embolize as distal as possible to within 2 cm from the renal vein – Coils placed during Valsalva and are slightly larger than the diameter of the gonadal vein – Be aware of anatomic variants and collaterals – Spasm, coil migration, vessel perforation • Other possible agents – Detachable balloons, glue, sotradecol, hot contrast Postprocedure management • • • • Observe at bed rest for >60 mins Consider f/u CXR D/c to responsible party Acetominophen/codeine for 3 days enough Results and complications • Technical success up to 100% * • 70-90% with some improvement * • Postembolization syndrome in up to 90% * – N/V, fever, pain – Can be confused for infection • Transient pelvic pressure or pain – Pelvic venous thrombosis • * Lindsay Machan, Handbook of Interventional Radiologic Procedures, 3rd edition. 5. Fallopian tube recanalization • Relieve obstruction(s) in the internal female reproductive tract causing infertility. • Infertility: inability to conceive after 1 yr of unprotected intercourse (6 mos if pt >35 yo). – 15-20% of reproductive age couples * – Female factors alone account for 35%; female with male factors account for another 20% * • 20-40% of female infertility due to fallopian tube disease – Lindsay Machan, Handbook of Interventional Radiologic Procedures, 3rd edition. • Supported by the American Fertility Society – 1st line treatment in patients with confirmed proximal tubal obstruction • Amy S Thurmond, RadioGraphics 2000;20:1759-176. • * Elizabeth E Puscheck, emedicine: Infertility. Indications • Proximal unilateral or bilateral fallopian tube occlusion confirmed by HSG, selective salpingography or laparoscopy – Needs evaluation by infertility specialists and gynecologist • Reocclusion after surgical reversal of tubal ligation Contraindications • Active PID • Severe tubal or peritubal pathology not amenable to laparoscopic or open repair • Severe uterine deformity or large masses making catheterization difficult • Distal tubal occlusion • Intrauterine adhesions (severe) • Severe anaphylactoid reactions to contrast media Preprocedure evaluation by IR • Review imaging/surgical studies • Patient education – Patient’s partner present – R/o other contributing male or female factors – State procedure is nonoperative alternative or adjunct to surgery or assisted fertility procedures – Discuss possible procedural complications ie tubal perforation, infection – F/u after missed period or positive pregnancy test • Ectopic pregnancy risk Alternative treatments • Microsurgery – Has been the treatment of choice for tubal occlusion – High cost and morbidity • In vitro fertilization – High cost, time consuming – Pregnancy rate 10-15% • Amy S Thurmond, RadioGraphics 2000;20:1759-176. Patient preparation • Schedule as outpatient during the follicular phase – After1st 3-5 days after bleeding has stopped • Avoids refluxing blood into the tubes or peritoneum – Before day 14 of her cycle • Ensures patient is not pregnant • Doxycycline 100 mg BID started 1-2 days prior and continued for 5 days after the procedure • Informed consent • Peripheral IV • Conscious sedation – Atropine 0.5 mg IM optional to prevent vasovagal sx Procedure • • • • • Lithotomy position with pelvis elevated Sterilely prepare the perineum Insert speculum and clean the cervix HSG with H2O soluble contrast Positive HSG – 5 F catheter selects the occluded ostium – Contrast injected through the introducing catheter • May be enough to restore patency Procedure • Proximal tubal occlusion further confirmed – 3 F catheter inserted coaxially through the 5 F catheter and obstruction is probed with an 0.018 wire • 3 F catheter advanced over the wire through the obstruction • Inject to confirm distal tube patency • If patency restored, remove 3 F system and inject through 5 F catheter to confirm patency • Manipulations are then done on the opposite side if appropriate • Final HSG through 5 F catheter with tip in the uterus – If the 1st tube opened is not patent, probably spasm, not indication to reopen • Average radiation dose to ovaries same as for a BE or IVP Steps in salpingography and fallopian tube recanalization courtesy of Imaging.consult.com (2008 Elsevier). Steps in salpingography and fallopian tube recanalization courtesy of Imaging.consult.com (2008 Elsevier). Postprocedure management • • • • • Observe for 60 mins Vaginal cramping and spotting for 1-2 d Avoid intercourse for 1 day Use pads for the next cycle Consult infertility specialist for treatment of other infertility d/o Tubal patency results • Tubal patency results – Technical success in 71%-92% • Amy S Thurmond, RadioGraphics 2000;20:1759-176. – Up to 100% success in idiopathic proximal tubal obstruction * – 44-77% success in occluded tubes after tubal ligation * – 77-82% success with SIN but technically more difficult * • Pregnancy results – Variable – Average reported pregnancy rate is 30% (9-47%) * • Reflects other factors contributing to infertility ie associated distal tubal disease, d/o of ovulation or sperm production • Most occur within the 1st 6 mos • Compare favorably with those of microsurgery • * Lindsay Machan, Handbook of Interventional Radiologic Procedures, 3rd edition. Complications and Follow Up • Complications – Tubal perforation – 2% * • Usually those with h/o proximal tubal surgery or severe SIN • No clinical sequelae – Ectopic pregnancy 1-5% * – Pelvic infection – Radiation exposure • Follow up – Reevaluation and reopening if not pregnant by 6 mos • 25% of reopened tubes reocclude by this time * • * Lindsay Machan, Handbook of Interventional Radiologic Procedures, 3rd edition. 6. Endovenous ablation of varicose veins • In 1994, half the adult population had minor stigmata of venous disease with 50-55% being women and fewer than half of the adult population have visible varicose veins with 20-25% of these being women – Wesley K Law et al, emedicine: Varicose Veins. • Risk factors: heredity, h/o DVT, female, parity, standing, hormones, aging, obesity, constipation, leg trauma • Sx: swelling, pain, cramps, fatigue, heaviness • Can progress to pigmentation changes, dermatitis and/or venous hypertension • Indications for treatment: cosmesis, aching, leg heaviness or fatigue, superficial thrombophlebitis, external bleeding, edema, skin changes • Result from valvular incompetence – Valvular incompetence cannot be reversed – Best treatments: control sx or remove the veins Greater (L) and lesser ® saphenous veins Treatment options • Conservative treatment: compression stockings, avoid standing, exercise • Surgery is the traditional tx – Ligation/stripping • Best known – Stab phlebectomy – Endoscopic powered phlebectomy or perforator ligation – Valvuloplasty, valve transplantation or transposition • Transcutaneous laser and high intensity pulsed light – Superficial telangiectasias • Percutaneous options – Endovenous ablation and US guided sclerotherapy Endovenous ablation • Thermal energy causes contraction of vessel wall collagen and/or fibrotic obliteration of the vessel lumen • Laser and RFA are thermal modalities • Goals: eliminate highest point of reflux, ablate incompetent venous segment • Contraindications: arterial disease, infection, active venous ulceration, central venous obstruction, hypercoagulable syndromes, occluded/absent deep veins, lymphedema, nonambulatory patient, poor general health, venous thromboembolism • Greater saphenous vein is vein most often treated • Careful patient selection and evaluation needed • Preprocedure US • Superficial varicosites mapped – Patency/competency of the GSV, LSV, major superficial draining veins, perforators, deep venous system Procedure • GSV accessed at the knee • Long vascular sheath advanced to the saphenofemoral junction • Tumescent anesthesia – Dilute (0.25-0.5%) lidocaine along GSV course in the fascial sheath • Ablation device through sheath until below saphenofemoral junction with device protruding out the end of the sheath 2 cm below SFJ • Device withdrawn through vein from SFJ to access site – Laser • Thin optical fiber causes steam bubbles which indirectly causes vein injury • Various laser energies available • Sheath and fiber pulled back at an average rate of 2 mm/s to deliver 70 J/cm Procedure • Average length of time to treat 45 cm vein segment using 810 nm laser: 3-5 min; 7.5 mins for 1320 nm laser * – RFA • Electrodes through catheter directly contact the vein wall and heat the vein to 85-90 degrees • Impedance and hence maintenance of temperature, dictates how rapidly the catheter is withdrawn • Average length of time to treat 45 cm vein segment: 18-24 mins * • Ablation device turned off before removing through skin • * http://www.closurefast.com/howitworks/ Postprocedure management • Compression stockings (30-40 mm Hg) for 1 wk • Immediate ambulation, avoid vigorous activity • US at 3-7 d – Confirms closed vein • US at 4-6 wks – Clinical and sonographic resolution – Residual venous tributaries treated with sclerotherapy Results and complications • Initial closure successful in 95-100% – Steven E Zimmel et al, emedicine: Varicose Vein Treatment with Endovenous Laser Therapy. • Initial closure successful in 83.5-88.2 % of RFA patients with the initial VNUS Closure system * • Initial closure successful in 100% of RFA patients with VNUSClosureFAST system * – Has shortened RFA procedure time to that comparable to laser • * Helane S. Fronek, The Fundamentals of Phlebology: Venous Disease for Clinicians, 2nd edition. Complications • Symptoms post tx: – Common – Access site bruising, moderate LE discomfort, tightness/pulling peaking in 5-7 d – Resolves in 1-3 wks • Complications: – Overall rare – Superficial thrombophlebitis, nerve injury, burns, DVT Sclerotherapy • Telangiectasias, reticular veins and varicosities • Follow up to invasive venous therapy • Contraindications: unable to ambulate, at risk for or concurrently have a DVT, hypercoagulable states, allergic reaction to sclerosants, difficulty ambulating, deep venous outflow obstruction, severe systemic illness, peripheral arterial insufficiency • Small syringe injects 0.5-1 cc sclerosant via 25 G needle • Agents: hypertonics or osmotics, detergents and toxins – Sodium tetradecyl sulfate is the most common agent in the US – Foamed detergents: easier US vis, less dilution, lower concentration, fewer side effects • Compression stockings (20-40 mm Hg) for 3-14 d, low level lower extremity exercise • Potential complications: swelling, pain, hyperpigmentation, DVT, thrombophlebitis skin necrosis, nerve injury and anaphylaxis