PowerPoint
advertisement

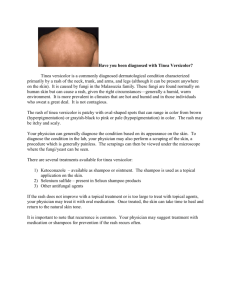
Cutaneous Fungal Infections Susan Massick, MD OSU Dermatology Learning Objectives Identify and diagnose cutaneous fungal infections Plan treatment approaches for dermatophyte skin infections What are Dermatophytes? Dermatophytes: fungi that digest keratin Geophilic: soil keratin Zoophilic: animal keratin Anthrophilic: human keratin Infection limited to keratin structures Stratum corneum Hair Nails Types of Dermatophyte Infections Tinea Capitis Tinea Corporis Tinea Cruris Tinea pedis and Onychomycosis Tinea Versicolor Common genera: Microsporum, Trichophyton, and Epidermophyton Tinea Capitis: Scalp Ringworm Common fungal infection in children, especially African American children Trichophyton tonsurans is most common anthrophilic organism to cause tinea capitis in U.S. Microsporum canis is most common zoophilic organism to cause tinea capitis in U.S. Clinical Manifestations of Tinea Capitis Patches of alopecia with erythema and scaling Small black dots Diffuse dandruff Kerion formation due to severe inflammation Physical exam: Round patchy alopecia with mild scale Physical exam: Black dot formation Physical exam: Kerion Physical exam: Diffuse scaliness Diagnosis of Tinea Capitis Diagnosis can be established by KOH and fungal culture Wood’s lamp can identify certain dermatophytes via fluorescence M. canis T. tonsurans + fluorescence - fluorescence Endothrix: Spores within the hair shaft Hair shaft Spores Ectothrix: Spores outside hair sheath Hair Shaft Spores outside hair sheath Wood’s lamp with fluorescence Treatment of Tinea Capitis Tinea capitis must be treated with oral therapy First line treatment: griseofulvin, which disrupts fungal microtubule formation Other alternative oral medications include terbinafine, fluconazole, and itraconazole Add shampoos, such as selenium sulfide, cicloprox, or ketoconazole, to decrease transmissibility of infection Tinea Corporis Also called ringworm Red scaly ring with central clearing May involve trunk, arms, legs, neck Physical exam (T. corporis): annular scaly red ring with central clearing Tinea Corporis: Diagnosis and Treatment Most common fungal etiologies: Trichophyton rubrum, Microsporum canis, and Trichophyton mentagrophytes Diagnosis can be made by KOH exam Can treat with topical antifungals for local disease and systemic oral antifungals, such as terbinafine or griseofulvin, if widespread KOH skin scraping: Fungal filaments Tinea Cruris Also known as “jock itch” Presents as chronic brown to red patches in groin folds and upper/inner thighs Rare before puberty, more common in men Often spares scrotum, penile shaft, glans penis Physical exam (T. cruris): Red patch in groin with sparing of penis and scrotum Tinea Cruris Should be differentiated from candidiasis, which is typically bright red, often involves scrotum, glans penis, may manifest satellite pustules Common fungal etiologies include Trichophyton rubrum, Trichophyton mentagrophytes, Epidermophyton floccosum Usually responds to topical antifungal therapy Tinea Pedis Extremely common fungal infection of skin of feet Commonly called “athlete’s foot” Similar fungal organisms that cause tinea cruris: Trichophyton rubrum and mentagrophytes Tinea pedis: Presentation and Treatment Moccasin type causes redness and scaling of soles and sides of feet Interdigital type produces white macerated fissures between the toes, usually 4th-5th spaces Bullous type produces small blisters on sole of foot Often responds to topical antifungal agents, such as topical terbinafine Physical exam: Moccasin type T. pedis Physical exam: T. pedis Onychomycosis Fungal infection of nails, or tinea unguium When toenails involved, often associated with tinea pedis May produce yellow or white discoloration of toenails with dystrophy or separation of nail from nailbed Nails may become thickened or develop white powder under the nail Fungal etiology is similar to tinea corporis: T. tonsurans, T. rubrum Physical exam: Onychomycosis Green nail: Pseudomonas infection Treatment of Onychomycosis Usually requires systemic antifungal agents with terbenafine being most effective. Itraconazole is less effective. Topical antifungals are less effective Tinea pedis cannot be effectively treated long term unless onychomycosis is also eliminated. Tinea versicolor (TV) Due to an overgrowth of a yeast (Pityrosporum ovale), which thrives on lipids, such as sebum Tinea versicolor (TV) usually presents as hypo or hyperpigmented macules with very fine scale on upper chest, upper back, shoulders Hypopigmentation is due to dicarboxylic acid produced by the yeast, which inhibits melanin formation Physical exam: T. versicolor Physical exam: T. versicolor Tinea versicolor: Diagnosis and Treatment Diagnosis made on physical exam and KOH scraping with characteristic “spaghetti and meatballs” appearance of hyphae and spores Treat with antifungal shampoos, such as selenium sulfide or ketoconazole, and/or with single doses of oral ketoconazole Tinea versicolor: KOH scraping Summary: Dermatophyte Infections Very common superficial fungal infections Often named for the body location targeted Tinea capitis, corporis, cruris, pedis Most common dermatophytes T. tonsurans, rubrum, mentagrophytes and M. canis Physical exam often characteristic, can confirm with KOH scraping and fungal culture Treatment with topical/oral antifungals Thank you for completing this module If you have any questions contact: David.Carr@osumc.edu Survey We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module. The survey is both optional and anonymous and should take less than 5 minutes to complete. Survey