Lung Sounds An Assessment of the Patient in Respiratory Distress
advertisement

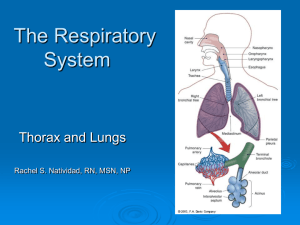
Lung Sounds An Assessment of the Patient in Respiratory Distress Michael Ciccarelli, DO December 12, 2006 Introduction • Lungs major function – Provide continuous gas exchange between inspired air and blood in the pulmonary circulation Anatomy of Respiratory System • • • • • • Nasopharynx Larynx Trachea Bronchi Bronchioles Alveoli Anatomy • Respiratory tract extends from mouth/nose to alveoli • Upper airway filters airborne particles, humidifies and warms inspired gases • Lower airway serves for gas exchange Anatomy Blood Supply • Lungs have a double blood supply – Pulmonary circulation for gas exchange with the alveoli (pulmonary artery with subdivisions) – Bronchial arteries arising from descending aorta supplies lung parenchyma Contributors of Respiration • Controlled in the brainstem • Mediated by muscles of respiration – Diaphragm primary muscle of inspiration – Accessory muscles of inspiration • SCM • Scalenes • Intercostals • Expiration is a passive process from elastic recoil of lung and chest wall, with passive diaphragm relaxation Mechanism for Breathing • Pressure gradient required to generate air flow – Diaphragm contracts, descends and enlarges thoracic cavity – Intra-thoracic pressure decreases – Air flows through tracheobronchial tree into the alveoli expanding lungs Technique for Respiratory Exam • NEED ORDERLY PROCESS • Before beginning, if possible: – Quiet environment – Proper positioning (patient sitting for posterior thorax exam, supine for anterior thorax exam) – Bare skin for auscultation – Patient comfort, warm hands and diaphragm of stethoscope, be considerate of women (drape sheet to cover chest) • • • • Inspect Palpate Percuss Auscultate Initial Respiratory Survey • Observe the patient’s breathing pattern – Rate (normal vs. increased/decreased) – Depth (shallow vs. deep) – Effort (any sign of accessory muscle use, inspect neck) • Assess the patient’s color – cyanosis Normal Respiratory Rates – Infant 30-60 – Toddler 24-40 – Preschooler 22-34 – School-age child 18-30 – Adolescent 12-16 – Adult 10-20 Pertinent History – Any chronic conditions • Asthma, COPD, CHF, DM – Exposure to new medication • ACE-Inhibitor, Abx – Recent change in diet • Peanuts, Strawberries – Substance abuse/Overdose • Opioid abuse, ASA toxicity – Prior DVT, PE – Recent trauma to chest Inspection • Note the shape of the chest and the way it moves – Deformities or asymmetry • Increased AP diameter in COPD – Abnormal retractions of interspaces during respiration • Lower interspaces, supraclavicular in acute asthma exacerbation – Impaired respiratory movement • Flail Chest and paradoxical movement with rib fx’s Palpation • Identify tender areas – Bruising with rib fx • Observe for appropriate chest wall expansion • Feel for tactile fremitus symmetrically – palpable vibrations transmitted to chest wall – use ulnar surface of hand, say “ninety-nine” – decreased with COPD, pleural effusions, PTX Percussion • Helps to identify if underlying tissues are air-filled, fluid-filled, or solid – Hyperextend middle finger of either hand and press against chest wall – Strike with flexed middle finger of opposite hand • Always percuss symmetrically on chest wall Percussion Notes • Flatness – Thigh • Dullness – Liver • Resonance – Lung • Hyperresonance – None • Tympany – Stomach, puffed cheek Percussion • Dullness replaces resonance when fluid or solid tissue replaces air containing lung – – – – PNA Pleural Effusions Hemothorax Tumor • Unilateral Hyperresonance – Pneumothorax • Generalized Hyperresonance – COPD Auscultation • • • • 12 anterior locations 14 posterior locations Auscultate symmetrically Should listen to at least 6 locations anteriorly and posteriorly Breath Sounds • Normal – – – – Tracheal Bronchial Bronchovesicular Vesicular • Abnormal – Absent/Decreased – Bronchial • Adventitious – – – – – Crackles (Rales) Wheeze Rhonchi Stridor Pleural Rub Normal Breath Sounds • Created by turbulent air flow • Inspiration – Air moves to smaller airways hitting walls – More turbulence, Increased sound • Expiration – Air moves toward larger airways – Less turbulence, Decreased sound • Normal breath sounds – Loudest during inspiration, softest during expiration Normal Breath Sounds • Tracheal – Very loud, high pitched sound – Inspiratory = Expiratory sound duration – Heard over trachea • Bronchial – – – – Loud, high pitched sound Expiratory sounds > Inspiratory sounds Heard over manubrium of sternum If heard in any other location suggestive of consolidation Normal Breath Sounds • Bronchovesicular – Intermediate intensity, intermediate pitch – Inspiratory = Expiratory sound duration – Heard best 1st and 2nd ICS anteriorly, and between scapula posteriorly – If heard in any other location suggestive of consolidation • Vesicular – Soft, low pitched sound – Inspiratory > Expiratory sounds – Major normal BS, heard over most of lungs Transmitted Voice Sounds • If abnormally located bronchial or bronchovesicular breath sounds assess transmitted voice sounds with stethoscope – Ask the patient to say “Ninety-nine”, should normally be muffled, if heard louder and clearer this is bronchophony – Ask the patient to say “ee”, should normally hear muffled long E sound, if E to A change this is egophony – Ask the patient to whisper “Ninety-nine”, should normally hear faint muffled sound, if louder and clearer sounds are heard this is whispered pectoriloquy • Increased transmission of voice sounds suggests that air filled lung has become airless Adventitious Breath Sounds • Crackles (Rales) – – – – Discontinuous, intermittent, nonmusical, brief sounds Heard more commonly with inspiration Classified as fine or coarse Normal at anterior lung bases • Maximal expiration • Prolonged recumbency – Crackles caused by air moving through secretions and collapsed alveoli – Associated conditions • pulmonary edema, early CHF, PNA Adventitious Breath Sounds • Wheeze – Continuous, high pitched, musical sound, longer than crackles – Hissing quality, heard > with expiration, however, can be heard on inspiration – Produced when air flows through narrowed airways – Associated conditions • asthma, COPD Adventitious Breath Sounds • Rhonchi – Similar to wheezes – Low pitched, snoring quality, continuous, musical sounds – Implies obstruction of larger airways by secretions – Associated condition • acute bronchitis Adventitious Breath Sounds • Stridor – Inspiratory musical wheeze – Loudest over trachea – Suggests obstructed trachea or larynx – Medical emergency requiring immediate attention – Associated condition • inhaled foreign body Adventitious Breath Sounds • Pleural Rub – Discontinuous or continuous brushing sounds – Heard during both inspiratory and expiratory phases – Occurs when pleural surfaces are inflamed and rub against each other – Associated conditions • pleural effusion, PTX Causes of decreased or absent breath sounds • • • • • • Asthma COPD Pleural Effusion Pneumothorax ARDS Atelectasis Case #1 • Dispatch Information – 62 yo female with progressive SOB over past 48 hours • PMH – 40 pack year smoking history – On home O2 – Some type of lung problem • VS – O2 sat 78% on 2L O2 NC, RR 26, T 98.1 • Physical Exam – – – – Barrel shaped chest Decreased BS B/L Diffuse expiratory wheezing B/L lung fields Digital cyanosis and clubbing noted What is this patient’s condition and appropriate treatment prior to ED arrival? Case #2 • Dispatch Information – 18 yo male with confusion and multiple episodes of vomiting • PMH – No past medical history – Denies recent drug use or overdose • VS – T 98.3, RR 32, HR 116, O2 sat 98% RA • Physical Exam – – – – Appears Lethargic Dry Mucous Membranes Deep, rapid breathing Lungs CTA B/L • Additional Findings – FS 450 What is this patient’s condition and appropriate treatment prior to ED arrival? Case #3 • Dispatch Information – 74 yo male with progressive SOB over past week • PMH – – – – Poor historian, no family available for information Difficult time sleeping on 4 pillows States sees a heart doctor, however, not taking pills At house full bottles of Coreg, Lisinopril, and Lasix • VS – RR 30, O2 sat 82% RA, T 98.4 • Physical Exam – – – – Rapid, shallow breathing Accessory muscles of respiration use Crackles are auscultated at B/L bases B/L LE pitting edema to knees What is this patient’s condition and appropriate treatment prior to ED arrival? Case #4 • Dispatch Information – MVA rollover on Rt. 4 in East Greenbush • • • • 25 yo male unrestrained driver significant intrusion into driver door + LOC, GCS 13 at present • PMH – EtOH abuse • VS – RR 28, O2 sat 76% RA • Physical Exam – multiple bruises on B/L chest wall – paradoxical movement of L chest wall – absent breath sounds on L side What is this patient’s condition and appropriate treatment prior to ED arrival? Case #5 • Dispatch Information – 42 yo female with difficulty breathing and facial swelling over past hour • PMH – HTN – NKDA or food allergies – Started Lisinopril for BP 1 month ago • VS – HR 108, RR 28, O2 sat 86% RA, T 98.4 • Physical Exam – Perioral facial and lip swelling – Inspiratory stridor on auscultation What is this patient’s condition and appropriate treatment prior to ED arrival?