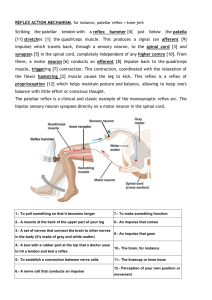
Emergency Nurses CARE
advertisement

TOMASITO M. DEMEGILLO JR, RN. MAN EMERGENCY NURSING Is a specialty area of the nursing profession like no other. Provide quality patient care for people of all ages, emergency nurses must possess both general and specific knowledge about health care. Emergency nurses must be ready to treat a wide variety of illnesses or injury situations, ranging from a sore throat to a heart attack. II. HISTORICAL DEVELOPMENT OF EMERGENCY NURSING The Emergency Nurses Association (ENA) Is the specialty nursing association serving the emergency nursing profession through research, publications, professional development, and injury prevention. ENA's mission is to provide visionary leadership for emergency nursing and emergency care. ENA is an organization seeking to define the future of emergency nursing and emergency care through advocacy, expertise, innovation, and leadership. Emergency Nurses CARE (EN CARE) (Virginia, USA) Is a not-for-profit organization with more than 6,000 trained emergency health care professionals who volunteer their time in their local communities in 50 states. EN CARE's mission is to reduce preventable injuries and deaths by educating the public to increase awareness and promote healthy lifestyles. The ENA Foundation (ENAF) (Illinois, USA) Is the philanthropic arm of ENA and its affiliates. Provides support for emergency nursing scholarships, research, and injury prevention. (Note: Applicants must be members of ENA) Philippine Society of Emergency Care Nurses, Inc. (PSECN) (Emergency Medical Services Department Philippine General Hospital Taft Avenue, Manila) Is a duly-recognized specialty organization of the Philippine Nurses Association (PNA). The current president is VIRGINIA DUCUSIN III. TRIAGE [French, from trier, to sort, from Old French.] Is the process of determining the priority of patients' treatments based on the severity of their condition. A method of quickly identifying victims who have immediately life-threatening injuries and who have the best chance of surviving. Emergent Divided into two: 1.Immediate - unstable and requiring attention within 15 minutes. Examples: Airway obstruction/compromise (actual or potential) Uncontrolled bleeding Shock 2. Urgent - temporarily stable but requiring care within a few hours. Examples: Threatened loss of limb or eyesight Multiple long-bone fractures. Nonemergency Situations - would require intervention, however, could stand significant delay. Examples: Walking wounded. Single long-bone fractures. Closed fractures. Soft tissue injuries without significant bleeding. Facial fractures without airway compromise. IV. Roles of Emergency Nurse A. Care Provider Emergency nurses care for patients and families in hospital emergency departments, ambulances, helicopters, urgent care centers, cruise ships, sports arenas, industry, government, and anywhere someone may have a medical emergency or where medical advances or injury prevention is a concern. B. Educator Emergency nurses provide education to the public through programs to promote wellness and prevent injuries, such as alcohol awareness, child passenger safety, gun safety, and domestic violence prevention. C. Manager Emergency nurses also work as administrators, managers, and researchers who work to improve emergency health care.They find time to provide excellent care for pts. D. Advocate Emergency nurses defend or plead a cause or issue on behalf of another. A nurse advocate has a legal and ethical obligation to safeguard the patient’s interests and rights. The Patient’s Bill of Rights a.k.a Patient Care Partnership Developed by the American Hospital Association in 1972 Goal is to promote the public’s understanding of their rights and responsibilities as consumers of health care. V. Qualifications of ER Nurse A Graduate of Bachelor of Science in Nursing A Registered Nurse Knowledgeable and Skillful for technology and equipments used in emergency care setting Must have a basic understanding of triage nursing Must be calm and collected under pressure and must be sympathetic to patients and their families They must be detail-oriented, as doctors' orders must be carried out instantly and correctly in emergency rooms. They must also be able to emotionally handle the daily sight of physical suffering and the reality that some patients may not be able to be saved, despite everyone's best efforts. VI. Legal Issues Affecting the Provision of Emergency Nursing CONSENT NEGLIGENCE CONFIDENTIALITY AUTONOMY GATHER EVIDENCE TREATMENT MALPRACTICE FIDELITY REPORT DECISION MAKING VII. Management of Care ANTHROPOMETRIC – is the measurement of the human individual for the purposes of understanding human physical variation. 1. Weight Accurate weight is required for: Pregnant patients Infants Children Elderly individuals Patients who have been prescribed certain medications Scale Should be placed in a spot that the patient is comfortable with Measured in pounds or kilograms Types: Balance beam scale Digital scale Dial scale 2. Height Can be measured using a Movable ruler on the back of most balance beam scales Graph ruler mounted on the wall Parallel bar moved down against the top of the patient’s head The Three Types of Scales Used in Medical Offices Include the Digital, Dial, and Balance Scale VIII. Safety & Infection Control Disease can be directly transmitted in two ways: A. Vertical disease transmission – passing a disease causing agent vertically from parent to offspring, such as perinatal transmission. B. Horizontal disease transmission – from one individual to another in the same generation (peers in the same age group). AIRBORNE TRANSMISSION Occurs when bacteria or viruses travel on dust particles or on small respiratory droplets that may become aerosolized when people sneeze, cough, laugh, or exhale. They hang in the air much like invisible smoke. They can travel on air currents over considerable distances. Examples: - Anthrax (inhalational) - Smallpox - Tuberculosis - Measles - Pertussis (whooping cough) - Chickenpox - Influenza Airborne Precautions: Be in a different room from the person who is ill, with a closed door in between. 2. If you need to be in the same room, wearing a mask may help for a brief exposure. 3. Covering the mouth or nose when coughing or sneezing decrease the risk of transmission. 1. DROPLET TRANSMISSION Occurs when bacteria or viruses travel on relatively large respiratory droplets that people sneeze, cough, drip, or exhale. They travel only short distances before settling, usually less than 3 feet. They can be spread directly if people are close enough to each other. The droplets land on hands, toys, tables, mats, or other surfaces, where they sometimes remain infectious for hours. Examples: Common cold Diphtheria Influenza Meningitis Mumps Pertussis (whooping cough) Plague Rubella Strep (strep throat, scarlet fever, pneumonia) Droplet Precautions: 1. Frequent hand washing help prevent transmission. 2. Covering the mouth or nose when coughing or sneezing decreases droplet transmission. 3. Using disposable towels and cups reduces the risk for infection. 4. Cleaning or disinfecting commonly touched infected surfaces (doorknobs, faucet handles, shared toys, mats in daycare) can also help. CONTACT TRANSMISSION Requires some form of touch to spread an infection. It is divided into two: Direct contact transmission - involves immediate contact between two people (or with an animal). b. Indirect contact transmission - involves fomites ; an object that becomes contaminated by touch then spreads the infection by touch. a. Examples: Abscesses Diphtheria (cutaneous) Lice Scabies Athlete’s foot Conjunctivitis (“pink eye”) Contact Precautions: Avoid direct contact with infected person especially when there is a break in the skin. Frequent hand washing Surface disinfecting can interrupt some disease transmission. Avoid sharing hairbrushes, combs, and hats. REVERSE TRANSMISSION The patient is being protected from the nurse and all the people in contact with the patient. Examples: - Immunocompromise patients - Cancer patients undergoing chemotherapy IX. Prevention & Early Detection ASSESSMENT 1. Glasgow Coma Scale Is a neurological scale that aims to give a reliable, objective way of recording the conscious state of a person for initial as well as subsequent assessment. Generally, brain injury is classified as: o Severe GCS ≤ 8 o Moderate GCS 9 – 12 o Minor GCS ≥ 13 and above The GCS has limited applicability to children, especially below the age of 36 months (where the verbal performance of even a healthy child would be expected to be poor). Pediatric Glasgow Coma Scale - a separate yet closely related scale, was developed for assessing younger children. 2. Palpatory The sensory skills developed by trained physicians and used in diagnosis and manipulative techniques. 3. Pulse Pressure Is the difference between the systolic and diastolic pressure. It represents the force that your heart generates each time it contracts. In a person with a systolic blood pressure of 120 mmHg and a diastolic pressure of 80 mmHg, the pulse pressure would be 40 mmHg. When the Pulse Pressure is greater than 60 mm Hg there is an increased incidence of adverse cardiovascular events especially in the older population. Several studies have identified that high pulse pressure: Causes more artery damage compared to high blood pressure with normal pulse pressure ii. Indicates elevated stress on a part of the heart called the left ventricle iii. Is affected differently by different high blood pressure medicines i. 4. Level of Consciousness (LOC) Is a measurement of a person's arousability and responsiveness to stimuli from the environment. Levels: Conscious - Oriented to time, place, name and date. Somnolent - Shows excessive drowsiness and responds to stimuli only with incoherent mumbles or disorganized movements. Obtunded - Has decreased interest in their surroundings, slowed responses, and sleepiness. Stuporous - People with an even lower level of consciousness, stupor, only respond by grimacing or drawing away from painful stimuli. Comatose - Do not even make this response to stimuli, have no corneal or gag reflex, and they may have no pupillary response to light. 5. Reflexes 1. Stretch or Deep Tendon Reflexes (DTRs) Measurement of the DTRs reflects the integrity of the reflex at specific spinal levels as well as the cerebral cortex function. For valid responses, the limbs should be relaxed and the muscles partially stretched. Elicit the reflex by applying a short, quick blow of the reflex hammer onto the muscle’s insertion tendon. Use a relaxed hold on the reflex hammer. Use the pointed end of the reflex hammer when testing a smaller target such as thumb on the tendon site. Use the flat end of the reflex hammer when the target is wider or to diffuse the impact and prevent pain. Compare the right and the left sides – the response should be equal. The reflex response is graded on a 4 – point scale as follows: 4+ Very brisk, hyperactive with clonus, pathologic 3+ Brisker than average, may be pathologic 2+ Average, normal 1+ Diminished, low normal 0 No response Abnormal Findings: Clonus is a set of rapid, rhythmic contractions of the same muscle. Hyperreflexia is the exaggerated reflex seen when the patient has upper motor neuron lesions (e.g., stroke). Hyporeflexia is the absence of a reflex. This is a lower motor neuron problem (e.g., spinal cord injury). a. Biceps Reflex (C5 to C6) Support the patient’s forearm. Use he patient’s forearm on yours. To relax and partially flex the patient’s arm. Place your thumb on the biceps tendon and strike a blow on your thumb. Use the pointed end of the reflex hammer. Normal response is contraction of the biceps muscle and flexion of the forearm. b. Triceps Reflex (C7 to C8) Instruct the patient to let the arm fully relax as you suspend it by supporting the upper arm. Strike the triceps tendon directly just above the elbow. Use the pointed end of the reflex hammer. Normal response is extension of the forearm. c. Brachioradialis Reflex (C5 to C6) Hold the patient’s thumb to suspend the forearm in relaxation. Strike the forearm directly about 2 to 3 cm. above the radial styloid process. Use the pointed end of the reflex hammer. Normal response is flexion and supination of the forearm. d. Quadriceps Reflex (“Knee Jerk”) (L2 to L4) Let the lower legs dangle freely to flex the knee and stretch the tendons. The popliteal area (back of the knee) should be few inches away from the edge of the bed. Place your hand above the patient’s knee. Strike the tendon directly just below the patella. Use the flat end of the reflex hammer. Normal response is extension of the lower leg. Contraction of the quadriceps (muscle of the thighs) may also be palpated. Note: if the patient is unable to sit, place him/her in supine position. Use your own arm as a lever to support the weight of one leg against the other leg. (Place your arm under the patient’s knee near you, and your hand above the knee of the other leg). . Achilles Reflex (“Ankle Jerk”) (L5 to S2) Position the patient with the knee flexed and the hip externally rotated. Hold the foot in dorsiflexion, and strike the Achilles tendon directly. Normal response is plantar flexion against your hand. Note: For the patient in supine position, flex one knee and support that leg. (Place the leg to be tested on top of the other leg, and externally rotated to have easy access on the Tendon of Achilles). Dorsiflex the foot and tap the tendon. f. Clonus. Test for clonus when the reflexes are hyperactive. Support the lower leg (under the knee) with one hand. With the other hand, move the foot up and down a few times to relax the muscle. Then, stretch the muscle by briskly dorsiflexing the foot. Hold the stretch. Normal response is no further movement is felt. Abnormal Finding: When clonus is present, you feel and see rapid, rhythmic contractions of the calf muscle and movement on the foot. A hyperactive reflex with sustained clonus (lasting as long as the stretch is held) occurs with upper motor neuron disease. 2. Superficial (Cutaneous) Reflexes These reflexes test the sensory receptors in the skin. The motor response is localized muscle contraction. a. Abdominal Reflexes – Upper (T8 to T10), Lower (T10 to T12) Place the patient is supine position with the knees slightly bent. Use the handle end of the reflex hammer, or a wood applicator tip, or the end of a split tongue blade to stroke the skin of the abdomen. Move from the side of the abdomen to the midline at both the upper and lower abdominal levels. Normal response is ipsilateral (same side) contraction of the abdominal muscle, with an observed deviation of the umbilicus toward the stroke. Abnormal Finding: Superficial reflexes are absent in diseases of the pyramidal tracts (e.g., stroke). b. Cremasteric Reflex (L1 to L2) This is not routinely done. It is done only on an unconscious male patient. Lightly stroke the inner aspect of the thigh with handle of reflex hammer or tongue blade. Normal response is elevation of the ipsilateral testis. Abnormal Finding: Absent in both upper motor neuron (UMN) and lower motor neuron (LMN) lesions. c. Plantar Reflex (Babinski Reflex) (L4 to S2) Position the thigh in slight external rotation. Use the handle of the reflex hammer to lightly stroke the lateral side of the foot from the hee, upward and inward across the ball of the foot (“inverted J fashion”). Normal response is plantar flexion of the toes and inversion and flexion of the forefoot (Negative Babinski Reflex). Abnormal Finding: Dorsiflexion of the big toe and fanning of all toes (positive Babinski). This indicates UMN disease of the corticospinal (or pyramidal) tract. Note: Positive Babinski is normal only among infants, which disappears by age 1 year. SUMMARY OF PATHOLOGIC (ABNORMAL REFLEXES) Reflex Method of Testing Abnormal Response and Indications 1. Babinski Stroke lateral aspect and across ball of foot. Extension of great toe, fanning of toes - Corticospinal (pyramidal) tract disease, e.g., stroke and trauma 2. Oppenheim Using heavy pressure with your thumb and index finger, stroke anterior medial tibial muscle. Same as above 3. Gordon Firmly squeeze calf muscles Same as above 4. Hoffman With patient’s hand relaxed, wrist dorsiflexed, fingers slightly flexed, sharply flick nail of distal phalanx of middle or index finger. Clawing of fingers and thumb. - Corticospinal (pyramidal) tract disease, e.g., stroke and trauma 5. Kernig In supine position, raise leg straight or flex thigh on abdomen, then extend knee. Resistance to straightening (because of hamstring spasm), pain down posterior thigh - Meningeal irritation, e.g., meningitis infections 6. Brudzinski With one hand under the neck and other hand on patient’s chest, sharply flex chin on chest. Watch hips and knees. Resistance and pain in neck, with flexion of hips and knees. OBTAINING SPECIMEN 1. Stool → A stool analysis is a series of tests done on a stool (feces) sample to help diagnose certain conditions affecting the digestive tract . → These conditions can include infection (such as from parasites, viruses, or bacteria), poor nutrient absorption, or cancer. 2. Urine → Urine test checks different components of urine, a waste product made by the kidneys. → The test can give information about your health and problems you may have. 3. Sputum → A sputum culture is a test to detect and identify bacteria or fungi (plural of fungus) that are infecting the lungs or breathing passages. → A sample of sputum is placed in a container with substances that promote the growth of bacteria or fungi. → If no bacteria or fungi grow, the culture is negative. → If organisms can cause infection grow, the culture is positive. COMPLETE BLOOD COUNT One of the most commonly ordered blood tests. The complete blood count is the calculation of the cellular (formed elements) of blood. CAPILLARY BLOOD GAS Capillary Blood is an attractive substitute sample that is routinely used in some clinical settings. The gold-standard sample for blood-gas analysis is arterial blood obtained via an indwelling arterial catheter or by arterial puncture. Blood-gas analyzers measure blood pH, and the oxygen and carbon-dioxide tensions of blood. Blood-gas analysis is helpful for assessment and monitoring of patients suffering a range of metabolic disturbances and respiratory diseases. ELECTROCARDIOGRAPH Derived from the Greek electro,(electrical activity), cardio, (heart), and graph, ("to write“). Is a transthoracic interpretation of the electrical activity of the heart over time captured and externally recorded by skin electrodes. It is a noninvasive recording produced by an electrocardiographic device. ECG works mostly by detecting and amplifying the tiny electrical changes on the skin that are caused when the heart muscle "depolarizes" during each heart beat. At rest, each heart muscle cell has a charge across its outer wall, or cell membrane. Reducing this charge towards zero is called depolarization, which activates the mechanisms in the cell that cause it to contract. Different types of ECGs can be referred to by the number of leads (3- lead, 5- lead, and 12- lead) 12-lead ECG Is one in which 12 different electrical signals are recorded at approximately the same time and will often be used as a on-off recording of an ECG, typically printed out as a paper copy. 3- and 5-lead ECGs Tend to be monitored continuously and viewed only on the screen of an appropriate monitoring device. Example: - During an operation or whilst being transported in an ambulance. PLACEMENT OF ELECTRODES Feature Description Duration RR interval The interval between an R wave and the next R wave . 0.6 to 1.2s P Wave During normal atrial depolarization, the main electrical vector is directed from the SA node towards the AV node, and spreads from the right atrium to the left atrium. This turns into the P wave on the ECG. 80ms PR Interval The PR interval is measured from the beginning of the P wave to the beginning of the QRS complex. The PR interval reflects the time the electrical impulse takes to travel from the sinus node through the AV node and entering the ventricles. The PR interval is therefore a good estimate of AV node function. PR Segment The PR segment connects the P wave and the QRS complex. This coincides with the electrical conduction from the AV node to the bundle of His to the bundle branches and then to the Purkinje Fibers. This electrical activity does not produce a contraction directly and is merely traveling down towards the ventricles and this shows up flat on the ECG. The PR interval is more clinically relevant 120 to 200ms 50 to 120ms QRS Complex The QRS complex reflects the rapid depolarization of the right and left ventricles. They have a large muscle mass compared to the atria and so the QRS complex usually has a much larger amplitude than the P-wave. 80 to 120ms J-Point The point at which the QRS complex finishes and the ST segment begins. Used to measure the degree of ST elevation or depression present. N/A ST Segment The ST segment connects the QRS complex and the T wave. The ST segment represents the period when the ventricles are depolarized. It is isoelectric. 80 to 120ms T Wave The T wave represents the repolarization (or recovery) of the ventricles. The interval from the beginning of the QRS complex to the apex of the T wave is referred to as the absolute refractory period. The last half of the T wave is referred to as the relative refractory period (or vulnerable period). 160ms ST Interval The ST interval is measured from the J point to the end of the T wave. 320ms QT Interval The QT interval is measured from the beginning of the QRS complex to the end of the T wave. A prolonged QT interval is a risk factor for ventricular tachyarrhythmias and sudden death. U Wave The U wave is hypothesized to be caused by the repolarization of the interventricular septum. They normally have a low amplitude, and even more often completely absent. They always follow the T wave and also follow the same direction in amplitude. If they are too prominent we suspect hypokalemia, hypercalcemia or hyperthyroidism usually. J Wave The J wave, elevated J-Point or Osborn Wave appears as a late delta wave following the QRS or as a small secondary R wave . It is considered pathognomonic of hypothermia or hypocalcemia. 300 to 430ms N/A X. Coping, Adaptation, and Psychological Adaptation DIET THERAPY Is an effective method of healing, especially when utilized as a complementary method of care. Is used for people who are trying to increase or decrease their body weight, have a sensitive digestion system that may be prone to allergies, who may not be able to digest certain foods, or are trying to overcome vitamin or mineral deficiencies. Types: 1.Ayurveda Diet Is an ancient Indian practice that works to prevent disease and rejuvenate the body. → Treat every part of the body, mentally and physically, through diet and meditation. → 2. Macrobiotics Diet → Is recommended for people suffering from cancer or other chronic diseases because it emphasizes eating low-fat, high-fiber food that is wholesome and minimally processed. The National Cancer Institute conducted a study showing that 90 percent of cancer in humans can be attributed to environmental causes. Food may be one of these causes. To prevent illness and boost the immune system → Eat a diet containing plenty of fresh fruit, vegetables and whole grains. → Reduce consumption of saturated and unsaturated fats and ditch caffeine and alcohol as much as possible. Nutrition Also called nourishment or aliment Is the provision, to cells and organisms, of the materials necessary (in the form of food) to support life. Many common health problems can be prevented or alleviated with a healthy diet. There are six major classes of nutrients: 1. 2. 3. 4. 5. 6. Carbohydrates Fats Minerals Protein Vitamins Water These nutrient classes can be categorized as either: 1. Macronutrients (needed in relatively large amounts) 2. Micronutrients (needed in smaller quantities) MACRONUTRIENTS Includes carbohydrates, fats, fiber, protein, and water. The macronutrients (excluding fiber and water) provide structural material (amino acids from which proteins are built, and lipids from which cell membranes and some signaling molecules are built) and energy. Carbohydrates May be classified as monosaccharides, disaccharides, or polysaccharides depending on the number of monomer (sugar) units they contain. They constitute a large part of foods such as rice, noodles, bread, and other grain-based products. Complex Carbohydrates It take slightly longer to digest and absorb because their sugar units must be separated from the chain before absorption. Simple Carbohydrates Are absorbed quickly, and therefore raise blood-sugar levels more rapidly than other nutrients. Carbohydrates are not essential to the human diet, as they are relatively low in vitamins and minerals, and energy can be provided from excess fats and proteins in the diet. FIBER Is a carbohydrate (or a polysaccharide) that is incompletely absorbed in humans and in some animals. When it is metabolized it can produce four Calories (kilocalories) of energy per gram. Dietary fiber consists mainly of cellulose, a large carbohydrate polymer that is indigestible because humans do not have the required enzymes to disassemble it. Whole grains, fruits (especially plums, prunes, and figs), and vegetables are good sources of dietary fiber. Dietary fiber helps reduce the chance of gastrointestinal problems such as constipation and diarrhea by increasing the weight and size of stool and softening it. There are two subcategories: 1. Insoluble fiber Found in whole-wheat flour, nuts and vegetables, especially stimulates peristalsis (the rhythmic muscular contractions of the intestines which move digesta along the digestive tract). 2. Soluble fiber Found in oats, peas, beans, and many fruits, dissolves in water in the intestinal tract to produce a gel which slows the movement of food through the intestines. This may help lower blood glucose levels because it can slow the absorption of sugar. Additionally, fiber, perhaps especially that from whole grains, is thought to possibly help lessen insulin spikes, and therefore reduce the risk of type 2 diabetes. FAT It is consists of several fatty acids (containing long chains of carbon and hydrogen atoms), bonded to a glycerol. They are typically found as triglycerides (three fatty acids attached to one glycerol backbone). It may be classified as saturated or unsaturated depending on the detailed structure of the fatty acids involved. Saturated fats It is from animal sources It is typically solid at room temperature (such as butter or lard), Have all of the carbon atoms in their fatty acid chains bonded to hydrogen atoms. Unsaturated fats Example is vegetable oil it is considered healthier Typically liquids (such as olive oil or flaxseed oil) Have some of these carbon atoms double-bonded, so their molecules have relatively fewer hydrogen atoms than a saturated fatty acid of the same length. It may be further classified as monounsaturated (one double-bond) or polyunsaturated (many double-bonds). Trans fats Are a type of unsaturated fat with trans-isomer bonds These are rare in nature and in foods from natural sources They are typically created in an industrial process called (partial) hydrogenation. Protein Are the basis of many animal body structures (e.g. muscles, skin, and hair). They also form the enzymes that control chemical reactions throughout the body. Each molecule is composed of amino acids, which are characterized by inclusion of nitrogen and sometimes sulphur (these components are responsible for the distinctive smell of burning protein, such as the keratin in hair). The body requires amino acids to produce new proteins (protein retention) and to replace damaged proteins (maintenance). Sources of dietary protein include meats, tofu and other soy-products, eggs, legumes, and dairy products such as milk and cheese. Excess amino acids from protein can be converted into glucose and used for fuel through a process called gluconeogenesis. The amino acids remaining after such conversion are discarded in urine. Water Is excreted from the body in multiple forms; including urine and feces, sweating, and by water vapour in the exhaled breath. Therefore it is necessary to adequately rehydrate to replace lost fluids. Early recommendations for the quantity of water required for maintenance of good health suggested that 6–8 glasses of water daily is the minimum to maintain proper hydration. For healthy hydration, the current EFSA (European Food Safety Authority) guidelines recommend total water intakes of 2.0 L/day for adult females and 2.5 L/day for adult males. These reference values include water from drinking water, other beverages, and from food. About 80% of our daily water requirement comes from the beverages we drink, with the remaining 20% coming from food. MICRONUTRIENTS Are minerals and vitamins Minerals Are the chemical elements required by living organisms, other than the four elements carbon, hydrogen, nitrogen, and oxygen that are present in nearly all organic molecules. The term "mineral" is archaic, since the intent is to describe simply the less common elements in the diet. Are often artificially added to the diet as supplements; the most famous is likely iodine in iodized salt which prevents goiter. Macrominerals Many elements are essential in relative quantity They are usually called "bulk minerals“ Some are structural, but many play a role as electrolytes 1. Calcium 2. Chlorine as chloride ion 3. A common electrolyte, but also needed structurally (for muscle and digestive system health, bone strength, some forms neutralize acidity, may help clear toxins, provides signaling ions for nerve and membrane functions) Very common electrolyte Magnesium Required for processing ATP and related reactions (builds bone, causes strong peristalsis, increases flexibility, increases alkalinity) 4. Phosphorus Required component of bones; essential for energy processing 5. Potassium A very common electrolyte (heart and nerve health) 6. Sodium A very common electrolyte; not generally found in dietary supplements, despite being needed in large quantities, because the ion is very common in food: typically as sodium chloride, or common salt. Excessive sodium consumption can deplete calcium and magnesium, leading to high blood pressure and osteoporosis. 7. Sulfur For three essential amino acids and therefore many proteins (skin, hair, nails, liver, and pancreas). Sulfur is not consumed alone, but in the form of sulfurcontaining amino acids. Trace Minerals Many elements are required in trace amounts, usually because they play a catalytic role in enzymes. 1. Cobalt Required for biosynthesis of vitamin B12 family of coenzymes. Animals cannot biosynthesize B12, and must obtain this cobalt- containing vitamin in the diet. 2. Copper Required component of many redox enzymes, including cytochrome c oxidase. 3. Chromium Required for sugar metabolism 4. Iodine Required not only for the biosynthesis of thyroxine, but probably, for other important organs as breast, stomach, salivary glands, thymus. 5. Iron Required for many enzymes, and for hemoglobin and some other proteins. 6. Manganese (processing of oxygen) 7. Molybdenum Required for xanthine oxidase and related oxidases 8. Nickel Present in urease 9. Selenium Required for peroxidase (antioxidant proteins) 10. Vanadium Is required for some lower organisms. 11. Zinc Required for several enzymes such as carboxypeptidase, liver alcohol dehydrogenase, and carbonic anhydrase Vitamins Some vitamins are recognized as essential nutrients, necessary in the diet for good health. Vitamin D is the exception: It can be synthesized in the skin, in the presence of UVB radiation. Certain vitamin-like compounds that are recommended in the diet, such as carnitine, are thought useful for survival and health, but these are not "essential" dietary nutrients because the human body has some capacity to produce them from other compounds. Moreover, thousands of different phytochemicals have recently been discovered in food (particularly in fresh vegetables), which may have desirable properties including antioxidant activity. Vitamin deficiencies may result in disease conditions, including goiter, scurvy, osteoporosis, impaired immune system, disorders of cell metabolism, certain forms of cancer, symptoms of premature aging, and poor psychological health. Excess levels of some vitamins are also dangerous to health (notably vitamin A), and for at least one vitamin, B6, toxicity begins at levels not far above the required amount. Deficient or excess levels of minerals can also have serious health consequences. RANGE OF MOTION EXERCISES (ROM) Is the movement of joint through its full ROM to prevent contractures and increase or maintain muscle tone/ strength. Types: 1. 2. 3. 4. Active – carried out by the client Passive – carried out by the nurse without assisstance from the client. Active assistive – client moves body part as far as possible and nurse completes remainder of movement. Active resistive – contraction of muscles against an opposing force Instructions on ROM Exercises: Learn passive ROM exercises from the person's caregiver. Practice the exercises with the caregiver first. The caregiver can make sure you are doing the exercises right. Caregivers can also show you the easiest way to do the exercises so you do not get hurt or tired. Raise the person's bed to a height that is comfortable for you. This will help keep you from hurting your back or other muscles. Make sure the wheels of the bed or wheelchair are locked before you start the exercises. Do all ROM exercises smoothly and gently. Never force, jerk, or over-stretch a muscle. This can hurt the muscle or joint instead of helping. Move the joint slowly. This is especially important if the person has muscle spasms (tightening). Move the joint only to the point of resistance. This is the point where you cannot bend the joint any further. Put slow, steady pressure on the joint until the muscle relaxes. Stop ROM exercises if the person feels pain. Ask the person to tell you right away if he feels any pain. Watch for signs of pain if the person is unable to talk. The exercises should never cause pain or go beyond the normal movement of that joint. Make ROM exercises a part of the person's daily routine. Do ROM exercises at the same time every day. Do them while bathing the person or while the person watches TV. This will make the time go faster and help the person relax more. Follow the caregiver's orders. The person's caregiver will tell you how many times per day you should do ROM exercises. The caregiver will tell you how many repetitions (number of times) you should do exercises on each joint. THANK YOU & GOD BLESS! GOODLUCK FOR THE RETURN DEMONSTRATION..c”,) • TOMASITO M. DEMEGILLO JR., RN. MAN How to deal with combative/ Psych. Pt. XI. Basic Care Comfort ENEMA Is the procedure of introducing liquids into the rectum and colon via the anus. The increasing volume of the liquid causes rapid expansion of the lower intestinal tract, often resulting in very uncomfortable bloating, cramping, powerful peristalsis, a feeling of extreme urgency and complete evacuation of the lower intestinal tract. It can be carried out as treatment for medical conditions, such as constipation, fecal impaction and surgical procedure such as sigmoidoscopy or colonoscopy. Types of Enema Solutions: Water/Water with mild hand soap 2. Mineral Oil - functions as a lubricant and stool softener, but which often has the side effect of sporadic seepage from the patient's anus which can soil the patient's undergarments for up to 24 hours. 3. Isotonic Saline - least irritating to the rectum and colon, having a neutral concentration gradient. 1. 1. Fleet Enema/ Clyss-go Useful as a laxative in the relief of constipation, and as a bowel evacuant for a variety of diagnostic, surgical and therapeutic indications. When administered rectally as an enema, they produce a watery evacuation of the bowel. Provides cleansing action and induces complete emptying of the left colon usually in 2 to 5 minutes. Contraindications: Should not be used when the following medical problems exist: o Appendicitis (or symptoms of), o Intestinal blockage o Ulcerative colitis o Ileitis o Heart disease o Rectal bleeding o High blood pressure o Kidney disease Children: Not recommended for infants under 6 months of age BANDAGE Is a piece of material used either to support a medical device such as a dressing or splint, or on its own to provide support to the body. Is available in a wide range of types, from generic cloth strips, to specialized shaped bandages designed for a specific limb or part of the body. Types: Gauze bandage The most common type of bandage It is a simple woven strip of material, or a woven strip of material with a Telfa absorbent barrier to prevent adhering to wounds, which can come in any number of widths and lengths. It can be used for almost any bandage application, including holding a dressing in place. Compression bandage Describes a wide variety of bandages with many different applications. a. Short stretch compression bandages Are good for protecting wounds on one's hands, especially on one's fingers. Are applied to a limb (usually for treatment of lymphedema or venous ulcers). Is capable of shortening around the limb after application and is therefore not exerting everincreasing pressure during inactivity. This dynamic is called resting pressure and is considered safe and comfortable for long-term treatment. The stability of the bandage creates a very high resistance to stretch when pressure is applied through internal muscle contraction and joint movement.This force is called working pressure. b. Long stretch compression bandages Have long stretch properties, meaning their high compressive power can be easily adjusted. They also have a very high resting pressure and must be removed at night or if the patient is in a resting position. Triangular bandage Also known as a cravat bandage Is a piece of cloth cut into a right-angled triangle, and often provided with safety pins to secure it in place. It can be used fully unrolled as a sling, folded as a normal bandage, or for specialized applications, as on the head. One advantage of this type of Bandage is that it can be makeshift and made from a fabric scrap or a piece of a t-shirt. Tube bandage Is applied using an applicator, and is woven in a continuous circle. It is used to hold dressings or splints on to limbs, or to provide support to sprains and strains, and it stops the bleeding. CASTS DEFINITION Is a temporary immobilization device which is made up of gypsum sulfate, unhydrous by calcination when mixed with water swells and forms into a hard cement. FUNCTIONS 1. To immobilize 2. To prevent or correct deformity 3. To support, maintain and protect realigned bone 4. To promote healing and early weight bearing PRINCIPLES 1. A cast is applied with padding applied first. -wadding sheet -roll of cotton -stockinette 2. Apply it to include the joint above and joint below the injured part. 3. Apply it in circular motion and mold it as you do the procedure using the palm of your hands. 4. Support it with the palm. CONTRAINDICATIONS: o Pregnancy o Skin diseases NURSING CARE 1. Assess neurovascular status. - pain, swelling, discoloration, cool skin, paresthesia, slow capillary refill, diminished or absent pulse, paralysis. 2. Assess skin integrity. - odor, drainage 3. Handle cast with the palm of hands especially during drying time. 4. Encourage isometric exercises for the muscles of the casted extremities. 5. Turn the client every 2 hours. (hip spica) 6. Encourage deep breathing and coughing exercises. (body cast) 7. Increase fluid intake. 8. Increase CHON and CHO in the diet. 9. No lotions, creams or oils use only alcohol. 10. Check for any complications. COMPLICATIONS: 1. Neurovascular compromise 2. Incorrect fracture alignment 3. Cast syndrome (body cast) - Probably results from hyperextension of the spine; characterized by nausea, abdominal pressure and vague abdominal pain. - Compression of superior mesenteric artery 4. Compartment syndrome - Vascular insufficiency and nerve and muscle compression due to unrelieved swelling - Bivalving or windowing 5. Infections Examples: LONG LEG CAST LONG ARM CAST SHORT LEG HIP SPICA CAST DOUBLE HIP SPICA CAST REMOVAL OF CASTS Instruments Needed: a. Cast cutter b. Spreader c. Knife d. Bandage scissors Nursing Care a. After the cast is removed, support the part and move the extremities gently. b. Observe the skin for any abrasions. c. Clean skin with mild soap and apply oil or lotion. POSITIONING It is a deliberative placement of the patient or a body part to promote physiologic and/or psychologic wellbeing. SUPINE POSITION Is a position of the body: lying down with the face up. When used in surgical procedures, it allows access to the peritoneal, thoracic and pericardial regions; as well as the head, neck and extremities. PRONE POSITION A position with the patient lying face down with arms bent comfortably at the elbow and padded with the arm boards positioned forward. FOWLER’S POSITION Is a standard patient position. It is used to relax tension of the abdominal muscles, allowing for improved breathing in immobile patients, and to increase comfort during eating and other activities. It is also used in postpartum women to improve uterine drainage. The patient is placed in a semi-upright sitting position (45-60 degrees) and may have knees either bent or straight. There are several types of Fowlers positions: a. Low Fowler’s b. Semi- Fowler’s c. High Fowler's. Low Fowler's Position Is when the patient's head is elevated 30-45 degrees. Semi- Fowler’s Position Is when a patient is lying in bed in a supine position with the head of the bed at approximately 30 degrees. Used for patients who are on tube feedings. High Fowler's Position Is when the patient's head is raised 60-90 degrees. Used when feeding a patient (especially one on feeding precautions), radiology needing to take a specific type of x-ray at the bedside, (at times) when a breathing treatment being given to the patient, when the patient is having difficulty breathing, dependent drainage after abdominal surgery, grooming, etc. STANDING POSITION Is a human position in which the body is held upright and supported only by the feet, referred to as an orthostatic state. SITTING POSITION Is a rest position supported by the buttocks or thighs where the torso is more or less upright. SQUATTING POSITION Is a posture where the weight of the body is on the feet (as with standing) but the knees are bent either fully (full or deep squat) or partially (partial, half, semi, parallel or monkey squat) It gives a greater increase of pressure in the pelvic cavity with minimal muscular effort. The birth canal will open 20 to 30% more in a squat than in any other position. It is recommended for the second stage of childbirth. TRENDELENBURG POSITION The body is laid flat on the back (supine position) with the feet higher than the head. Is a standard position used in abdominal, gynecological surgery, and for hypotensive patients. KNEE-CHEST POSITION A prone position in which the individual rests on the knees and upper part of the chest, assumed for gynecologic or rectal examination. Also called genupectoral position. DORSAL RECUMBENT POSITION Patient on the back, with lower limbs flexed and rotated outward. Used in vaginal examination, application of obstetrical forceps, and other procedures. LITHOTOMY POSITION Is a medical term referring to a common position for surgical procedures and medical examinations involving the pelvis and lower abdomen, as well as a common position for childbirth The patient is laid on the back with knees bent, positioned above the hips, and spread apart through the use of stirrups. SIM’S POSITION It is performed by having a patient lie on their left side, left leg extended and right leg flexed. Is usually used for rectal examination, treatments and enemas. ORTHOPNEIC POSITION A position assumed to relieve ORTHOPNEA (difficulty breathing except when in an upright position) The patient assumes an upright or semivertical position by using pillows to support the head and chest, or sits upright in a chair. ORTHOPNEIC TRENDELENBURG XII. Pharmacological & Parenteral ECART DRUGS Atropine Sulfate Sodium /luminal Aminophylline Buscopan 100mg/ ml Amoiordarone Dopamine 200 mg/ 5ml Epinephrine (DBL) Hemostan 500 mg/15cc Dobutamine 200 mg/5ml Benadryl 50 mg/ cc Lanoxin/ Digoxin 0.5/2 Xylocaine Mg. Sulfate 250 mg/ml Furosemide/ Lasix Nifedipine/ Calcibloc 5mg Diazepam Verapamil/ Isoptin 5mg/ml Calcium Gluconate 10mg/ml Magnesium Sulfate 4mg/ml Bricanyl 1cc Dormicum 15mg/2ml DRUG COMPUTATION 1. Oral and solid medication doses: Desired X quantity Stock 2. Intravenous Drip Rate: Total Number of milliliters ordered = number of ml/hr Number of Hours to run Total Vol. = cc/hr # of hours to run Briefly, #ml ordered = ml/hr #hr to run # of milliliter per hour X tubing drip factor = drops/min. Number of hour Briefly, ml/hr x TF = drops per minute #min INSULIN ADMINISTRATION ONSET PEAK DURATION 1 hr. 4 hrs. 8 hrs. INTERMEDIATE 2 hrs. 8 hrs. 16 hrs. LONG-ACTING 4 hrs. 16 hrs. 32 hrs. REGULAR VOLUMETRIC PUMP A device for administration of intravenous fluids with great accuracy. The Soluset Solution Set Comes complete with a 100mL calibrated burette, injection site on the burette with automatic shutoff valve, and a Y-Site 6" from the needle adapter end. 60 drops per mL drip chamber. S O L U S E T BLOOD TRANSFUSION BLOOD o A mixture of cells o A complex TRANSPORT mechanism Transport hormones Removes waste products Regulates body temperature Protects the body Promotes hemostasis Supplies oxygen COMPOSITION OF BLOOD Temperature 38˚C (100.4˚F) pH 7.35- 7.45 Specific Gravity 1.048- 1.066 Body Weight 7% 5 times the viscosity of water Volume - Male 5-6 Liters - Female 4-5 Liters Cellular Components: Formed elements of blood: 1. RBC = responsible for oxygen transport 2. WBC = play a major role in defense against microorganisms 3. Platelets = function in hemostasis National Blood Services Act of 1994 Also known as the Republic Act 7719 AN ACT PROMOTING VOLUNTARY BLOOD DONATION PROVIDING FOR AN ADEQUATE SUPPLY OF SAFE BLOOD, REGUALTING BLOOD BANKS, AND PROVIDING PENALTIES FOR VIOLATION THEREOF. BLOOD TRANSFUSION Is the process of receiving blood products into one's circulation intravenously. A life saving therapy for patients with a variety of medical and surgical conditions in need of blood. Early transfusions used whole blood, but modern medical practice commonly uses only components of the blood, such as red blood cells, white blood cells, plasma, clotting factors, and platelets. Blood Collection Methods: 1. Unrelated Donor ( Allogeneic) 2. Directed Donor 3. Autologous Donor (Self) Component Volume Recommended Hrs. of Transfusion WB 500ml 4 hours PRBC 250ml 1 hr. 30 min. – 2 hrs. Platelets 50ml 10-15 min. Cryoprecipitate 20ml 5-10 min. FFP 200-250ml 5-10 min. Eligible Donor Must Be: 18 years old and above Weight at least 110 lbs. (50 kgs.) Free from skin diseases Not have donated in the past 56 days Have a hemoglobin level of at least : 12.5 g/dL(women) 13.5 g/dL (men) Ineligible Donor: AIDS Hepatitis Types of Cancer Hemophilia Have received clotting factor concentrations Acute Transfusion Reactions - Usually appear within the first 5- 15 minutes after the transfusion is started. Bloody Urine Chills Hypotension Severe low back/ flank or chest pain Low or absent UO Nausea and vomiting Dyspnea, wheezing Diaphoresis NURSES MUST BE: Assure the informed consent has been obtained before starting a transfusion Appropriate information to include in patient education includes: - Benefits - Risks - Alternatives to transfusion Document all patient education regarding transfusion therapy and the responses of patients and family members after teaching. Safety Precaution Make sure that you are protected by: -Wearing proper PPE - Always perform disinfection technique - If using sharps, do not recap needle - Always observe proper waste disposal according to your institutions policy - Make sure the blood bag is secured - Always double or triple check - Always perform HAND HYGIENE Transfusion Precaution Don’t add medicines to the blood Don’t transfuse the blood product if you discover a discrepancy in the blood number, blood slip type, or patient identification number. BEFORE TRANSFUSION When you received the delivery from the blood bank you should receive both the product and the transfusion record that corresponds to it. Inspect the following: Labels Integrity of unit Appearance DURING TRANSFUSION Administer the blood or component at the recommended rate Stay with the patient for the first few minutes of transfusion Review signs and symptoms of what the patient should report AFTER TRANSFUSION Continue to monitor patient for any signs and symptoms of reaction for at least one hour after the transfusion Obtain any ordered post- transfusion laboratory studies Note: The Registered Nurse shall follow these steps immediately after detecting signs and symptoms of an acute transfusion reaction. 1. Stop the transfusion immediately. 2. Change the I.V. tubing to prevent infusing more blood. Save the blood tubing and bag for analysis. 3. Administer normal saline solution to keep the vein patent (open). 4. Take and record the patient’s vital signs. 5. Notify the doctor. 6. Prepare for further treatment. 7. Complete transfusion reaction report and an incident report according to your facility’s policies and procedures. CHANGING OF IV LINES/ TUBINGS When to change IV Lines/ Tubings (trouble shooting)? 1. 1. Usually according to the hospital policy (usually 72 hours) Contamination is suspected and noted XIII. Reduction of Risk Potential ASSISTIVE DEVICES Is an umbrella term that includes assistive, adaptive, and rehabilitative devices for people with disabilities and also includes the process used in selecting, locating, and using them. It promotes greater independence by enabling people to perform tasks that they were formerly unable to accomplish, or had great difficulty accomplishing, by providing enhancements to or changed methods of interacting with the technology needed to accomplish such tasks. Cane - A stick used as an aid in walking or carried as an accessory. Types: a. single b. tripod cane c. quad cane Nursing Care: Teach client to hold cane in hand opposite affected extremity, and to advance cane at the same time the affected leg is moved forward. Walker 1. Mechanical device with four legs for support 2. Nursing Care Teach client to hold upper bars of walker at each side, then to move the walker forward and step into it. Crutches 1. Assure proper length. a. When client assumes erect position the top of crutch is 2 inches below the axilla, and the tip of each crutch is 6 inches in front and to the side of the feet. b. Client’s elbow should be slightly flexed when hand is on hand grip. c. Weight should not be borne by the axilla. 2. Crutch gaits a. Four point gait – used when weight bearing is allowed on both extremities. 1. advance right crutch 2. step forward with left foot 3. advance left crutch 4. step forward with right foot b. Two point gait – typical walking pattern 1. step forward moving both right crutch and left leg simultaneously. 2. step forward moving both left crutch and right leg simultaneously. c. Three point gait – used when weight bearing is permitted on one extremity only. 1. advance both crutches and affected extremity several inches, maintaining good balance. 2. advance the unaffected leg to the crutches, supporting the weight of the body on the hands. d. Swing – to gait – used for clients with paralysis of both lower extremities who are unable to lift feet from floor. 1. both crutches are placed forward 2. client swings forward to the crutches e. Swing- through gait – same indications as for swing – to gait 1. both crutches are placed forward 2. client swings body through the crutches SINGLE CANE TRIPOD CANE QUAD CANE Walker Crutches Carry: 1 man, 2 man, 3 man LOG ROLLING Is a maneuver used to turn a reclining patient from one side to the other or completely over without flexing the spinal column. The arms of the patient are folded across the chest, and the legs extended. A draw sheet under the patient is manipulated by attending health care team members or nursing personnel to facilitate the procedure. BED TRANSFER Is performed independently or with caregiver assistance depending on if the person has a low or high level of mobility. This technique requires some practice, but knowing the necessary actions for a safe transfer from a bed to a chair can increase self-reliance and decrease the risk of an injury. General Rules for Safe Patient Handling: Think first before initiating any patient activity Plan the activity Maintain the curve in your low back Get as close to the patient as possible when providing care • Get necessary assistance of another person or assistive equipment whenever possible • Keep your stomach tight and your head and shoulders up • • • • • Pivot or side step – DO NOT TWIST • Make sure the path is clear and the floor is dry • If transferring to a chair, make sure the chair is properly positioned • Always transfer the patient to their unaffected stronger side unless otherwise instructed by a Physical Therapist • Use your legs, not your back, when lifting • Bend your knees – never lift with your legs straight • Have the patient help you as much as possible, know their transfer and ADL status • Provide simple clear directions for the patient and explain what you are doing each step of the way • Use a draw sheet if the patient is heavy or can only minimally assist • Whenever possible, use your body weight and momentum to move the patient rather than just muscle strength • Place feet shoulder width apart or one foot in front of the other to provide a wide, solid base of support Equipments used in Bed Transfer: a. Hoyer Lifts For patients who are unable to provide their own assistance in the transfer b. Transfer boards Allow the user to slide slowly into a wheelchair For independent transferring c. Bed rails Act as stability bars to lift themselves off the bed and move at their own rate of transfer. For independent transferring d. Trapeze bar Act as stability bars to lift themselves off the bed and move at their own rate of transfer. For independent transferring You can put a free standing trapeze bar hovering above the bed or have an attached trapeze bar hang over the bed for disabled persons to pull themselves into position for resting, sitting or transferring without much or any assistance from caregivers. HOYER LIFTS TRANSFER BOARDS BED RAILS TRAPEZE BAR XIV. Physiologic Adaptation ABG READING Is taken to measure the Ph of arterial blood. Ph of the arterial blood is normally between 7.35 and 7.45. A Ph above or below this range is dangerous to a patient. Normal ABG Range 1. Ph - 7.35-7.45 2. PaCO2 - 35-45 mm/hg 3. HCO3 - 22-26 mm/hg 4. PaO2 80-100 mm/hg - The oxygen level in the arterial blood. pH Alkalosis Acidosis PCO2 Acidosis HCO3 Alkalosis Acidosis PCO2 HCO3 - Respiratory (Lungs) - Metabolic (Kidney) Alkalosis OXYGEN THERAPY 1. Nasal Cannula It a device used to deliver supplemental oxygen or airflow to a patient or person in need of respiratory help. This device consists of a plastic tube which fits behind the ears, and a set of two prongs which are placed in the nostrils. Oxygen flows from these prongs. Is connected to an oxygen tank, a portable oxygen generator, or a wall connection in a hospital via a flow meter. It carries 1–6 liters of oxygen per minute The oxygen fraction ranges from 24% to 35% 2. Face Mask Are made up of clear, pliable plastic or rubber that can be molded to fit the face. They are designed to cover the nose and mouth There are several holes in the sides of the mask (exhalation ports) to allow the escape of exhaled carbon dioxide. It carries 5-8 Liters per minute The oxygen fraction ranges from 40% to 60% NEBULIZATION Drawing into the respiratory tract, a non- volatile drug, transformed into a fine mist with the use of nebulizer, or aerosol apparatus. Purpose: To deliver finer mist at a faster rate Special Considerations: 1. Administer the inhalation not too close to meal time 2. Give the therapy prior to coughing exercises or postural drainage. Reasons to avoid the treatment include: Increased blood pressure Increased pulse History of adverse reaction to the medication Equipments: Lined tray with: Nebulizer b. Prescribed drug c. Sterile syringe & needle or medicine glass d. Normal Saline Solution e. Spout with medicine container a. PROCEDURE: 1. Assemble the equipments 2. Measure the prescribed amount of drug with a syringe needle and place into the nebulizer’s drug compartment 3. Placed on a lined tray and bring to the client’s bedside 4. Connect the nebulizer directly into the electric outlet 5. Place client in fowler’s or sitting position if tolerated 6. Direct the nebulizer towards the client’s mouth and instruct to inhale the mist deeply through the mouth, pause and hold breath for 3-4 seconds. Exhale slowly through pursed lips. 7. Instruct client to continue until the solution is vaporized. Often, the effects of the treatment are most apparent 15-20 minutes later, and you may need assisted coughing or suctioning at that time. CHEST PHYSIOTHERAPY Sequence is usually positioning, percussion, vibration, & removal of secretions by coughing or suction. Chest Percussion Also called clapping or cupping It is done by forcefully striking the skin with cupped hands over specified congested lung area to mechanically dislodge tenacious secretions from the bronchial walls. It is carried out for only 1 or 2 min. or up to 5 min. over each area according to M.D.’s order. Vibration A series of vigorous quiverings produced through hand that are placed flat against the chest wall. It is used after percussion, to increase the turbulence of the exhaled air and thus loosen thick secretions. It can replace percussion if client is experiencing chest pain. It is often done 4 or 5 times during postural drainage. Postural Drainage The drainage by gravity, of secretions, from various lung segments. A wide variety of positions is necessary to drain all segment of the lung, but not all positions are required for every person. Only those positions that drain specific diseased areas are used. Each position is usually assumed for 10-15 min. Treatment is scheduled 30 min. to 1 hour before meals so that a client will not vomit the meal. Before treatments, bronchodilators or moisturizing nebulization therapy may be ordered. Things needed: Pillows to support the client comfortably in the required positions Tissues for expectorated secretions Sputum container for expectorated secretions Mouthwash to clean and freshen the mouth following the treatment Bed that can be placed in trendelenburg’s position Gown or pajama to prevent undue exposure and to protect the skin during percussion and vibration A towel to place over the area to be percussed to prevent discomfort DRAINAGE OF THE UPPER LOBES Three segments – the apical or uppermost segments and below them, the anterior and posterior segments. A. To drain the apical segments of the upper lobes Lie back at a 30 degrees angle Percuss and vibrate between the clavicles and above the scapulae B. To drain the posterior segments of the upper lobes Have client sit upright in a chair or bed with the head bent slightly forward. Percuss and vibrate the areas between the clavicles and the scapulae. C. To drain the anterior segments of the upper lobes Have client lie on a flat bed with pillows under the knees to flex them. Percuss and vibrate the upper chest below the clavicles down to the nipple line, except for women. DRAINAGE OF THE RIGHT MIDDLE LOBE AND LOWER DIVISION OF THE LEFT UPPER LOBE Two segments – lateral and medial. The lower division of the left upper lobe, called the lingual of that lobe, has two segments – superior and inferior To drain the Right Lateral and Medial Segments Elevate the foot of the bed about 15 degrees or 40 cm (15 in.), and have the client lie on the left side. Help the client to lean back slightly (about a quarter turn) against pillow extending at the back from the shoulder to the hip. A pillow may be placed between the knee for comfort. For male: Percuss and vibrate over the right side of the chest at the level of the nipple between the 4th and 6th rib. For female: Position the heel of your hand toward the axilla and your cupped finger extending forward beneath the breast to percuss and vibrate beneath the breast. To drain the Left Lingular Segments Elevate the foot of the bed about 15 degrees and have the client lie on the left side. Percuss the right side of the chest beneath the breast. To drain the lateral Basal Segments Have the client lie partly on the unaffected side and partly on the abdomen. Elevate the foot of the bed about 30 degrees or 45 cm (18in) or to the height tolerated by the client. An alternative is to elevate the hips with pillows. Percuss and vibrate the uppermost side of the lower ribs. To drain the Posterior Basal Segments Have client lie prone. Elevate the foot of the bed about 30 degrees or 45 cm ( 18in) or to the height tolerated by the client. Elevate the hip on two or three pillows to produce a jack knife position from the knees to the shoulders. Percuss and vibrate over the lower ribs on both sides close to the spine, but not directly over the spine or the kidneys. DRAINAGE OF THE LOWER LOBES Four Segments – superior, anterior basal, lateral basal, and posterior basal. To drain the Superior Segments Have client lie on the abdomen on a flat bed, and place two pillow under the hips. Percuss and vibrate the middle area of the back on both sides of the spine. To drain the Anterior Basal Segments Have client lie on the unaffected side, with the upper arm over the head. Elevate the foot of the bed about 30 degree or 45 cm (18 in), or to the height tolerated by the client. Place one pillow between the knee. Another under the head is optional. Percuss and vibrate the affected side of the chest over the lower ribs, inferior to the axilla. NASOGASTRIC TUBE Levin Tube is commonly used Is a common procedure that provides access to the stomach for diagnostic and therapeutic purposes. Purpose: –To provide feeding –To irrigate stomach ( gastric lavage) –For decompression –To administer medications –To administer supplemental fluids GASTROSTOMY Is a surgically created opening in the stomach. Is needed if you are not able to eat enough for adequate nutrition during treatment. Extra food and fluids are given through a gastrostomy tube, also called a G-tube. GASTROSTOMY TUBE Is placed in the stomach to help with feeding or venting of stomach gas. There are 2 main types of G-tubes: o A G-tube that is placed in the stomach during surgery and has a tube that stays on the outside. This tube is held in place by a small fluid-filled balloon inside the stomach. o A percutaneous endoscopic gastrostomy (PEG) tube placed in the stomach using a scope passed through the mouth into the stomach. A balloon or plastic disc (cap) in the stomach holds the tube in place. GASTROSTOMY CARE Wash your hands with soap and water before and after touching the area. 2. Use warm water and soap to clean around the gastrostomy site 2 to 3 times a day or as needed. 3. Make sure that you gently soak or scrub off all crusted areas on the skin around the tube and on the tube itself. You may need to use a diluted solution of hydrogen peroxide (1/2 peroxide and 1/2 water) with Q-tips to clean around the tube site. 1. 4. After cleaning, rinse around the area with plain water and pat dry. 5. You may use an antibiotic ointment around the site if the area looks red or sore COLOSTOMY Is a reversible surgical procedure in which a stoma is formed by drawing the healthy end of the large intestine or colon through an incision in the anterior abdominal wall and suturing it into place. This opening, in conjunction with the attached stoma appliance, provides an alternative channel for feces to leave the body. A temporary colostomy may be needed to allow the colon to rest and heal for a period of time. It may be in place for weeks, months, or years. It will eventually be closed and bowel movements will return to normal. A permanent colostomy is usually needed when a part of the colon must be removed or cannot be used again. Types of Colostomies: 1. Ascending colostomy Has a stoma (opening) that is located on the right side of the abdomen. The output (stool) that drains from this stoma is in liquid form. 2. Transverse colostomy: Has stoma that is located in the upper abdomen towards the middle or right side. The output that drains from this stoma may be loose or soft. 3. Descending or sigmoid colostomy: Has stoma that is located on the lower left side of the abdomen. The output that drains from this stoma is firm. Things used for Colostomies: 1. Pouch Are lightweight and odor-proof. Pouches have a special covering that prevents the pouch from sticking to the body. Some pouches also have charcoal filters which release gas slowly and help to decrease gas odor. Types of Pouches: 1. Open-ended pouch 2. Close-ended pouch 3. One-piece 4. Two-piece 5. Pre-cut or cut-to-fit pouches 2. Stoma covers and caps Can be placed on the stoma when the stoma is not active (draining). People with descending or sigmoid colostomies who irrigate may use stoma covers or caps. Is attached to the skin in the same way as pouch 3. Skin protection Film Can be placed on the skin to protect against damage from the adhesive material. Are helpful for people with sensitive, dry, or oily skin. Pectin-based paste or paste strips/rings Are helpful for protecting skin against output that contains digestive enzymes (proteins that break down foods). Ascending or transverse colostomies can produce output that contains digestive enzymes, which can irritate or damage the skin. The paste is also used to create a flat pouch surface by filling in small skin creases. POUCH STOMA CAPS Emptying the pouch: Empty the pouch when one-third to one-half full. Do not wait until the pouch is completely full because this could put pressure on the seal, causing a leak. The pouch may also detach, causing all of the pouch contents to spill. Place toilet paper into the toilet to reduce splash back and noise. Take the end of the pouch and hold it up. Remove the clamp (if the pouch has a clamp system). Take the end of the end of the pouch and make a cuff to keep it from getting soiled. Some pouches will not require you to cuff the pouch. Drain the pouch by squeezing the pouch contents into the toilet. Clean the cuffed end of the pouch with toilet paper or a moist paper towel. You may also rinse the pouch but it is not necessary. Make sure and keep the end of the pouch clean. Undo the cuff at the end of the pouch. Replace the clamp or close the end of the pouch according to your caregiver's instructions. IRRIGATION Means putting an enema into the stoma. Allows a person to have timed bowel movements. Allow a person to be free from stool output for about 24 to 48 hours. Things Needed: 1. 2. 3. Plastic irrigating container Irrigation sleeve Adjustable belt Procedure: Fill the irrigating container with about 16 to 50 ounces of lukewarm water. The water should not be cold or hot. The amount of water each person needs to put in the irrigating container varies. 2. Hang the irrigation container at a height in which the bottom of the container is level with your shoulder. Sit up straight on the toilet or on a chair next to the toilet. 3. Take the adjustable belt and attach it to the irrigation sleeve. Place the belt around your waste and place the sleeve over your stoma. Place the end of the irrigation sleeve into the toilet bowel. 1. 4. Release air bubbles from the tubing on the plastic irrigating container by releasing the clamp. Allow a small amount of water to be released into the sleeve. Clamp the tubing again. 5. Moisten the end of the cone with water or lubricate it with water-soluble lubricant. 6. Place the tip of the cone about three inches deep into the stoma. Make sure there is a snug fit but do not place the cone too deeply or forcefully into the stoma. Release the clamp on the tubing again and allow the water to flow into the stoma. The water must go in slowly and takes about five to ten minutes. Keep the cone in place for another 10 seconds. 7. Remove the cone from the stoma. Allow the output to drain into the irrigation sleeve for about 10 to 15 minutes. 8. Dry the end of the irrigation sleeve. Clip the bottom of the sleeve to the top with a clasp or close the end of the sleeve with the tail closure. You may move around for about 30 to 45 minutes until all the water and stool has drained. 9. Drain the output from the sleeve into the toilet. Clean the area around the stoma with mild soap and water and pat dry. IRRIGATION CONTACT A CAREGIVER IF: You have a fever (increased body temperature). Unusual odor that lasts longer than a week. Your skin around the stoma is red and irritated and you do not know what to do. You have nausea, vomiting, pain, cramping, or bloating. You have diarrhea. Your bowel habits change, like having little or no stool output. Your stoma size changes or becomes narrow (stenosis). Your stools are black or bloody. SEEK CARE IMMEDIATELY IF: o Your stoma is bleeding and you cannot stop the bleeding. o You are too weak to stand up. o You have bad abdominal (belly) pain. DM FOOT CARE DM FOOT CARE A person with diabetes should do the following: Foot Examination Examine your feet daily and also after any trauma, no matter how minor, to your feet. Report any abnormalities to your physician. Use a waterbased moisturizer every day (but not between your toes) to prevent dry skin and cracking. Wear cotton or wool socks. Avoid elastic socks and hosiery because they may impair circulation. Eliminate obstacles Move or remove any items you are likely to trip over or bump your feet on. Keep clutter on the floor picked up. Light the pathways used at night indoors and outdoors. Toenail trimming Always cut your nails with a safety clipper, never a scissors. Cut them straight across and leave plenty of room out from the nail bed or quick. If you have difficulty with your vision or using your hands, let your doctor do it for you or train a family member how to do it safely. Footwear Wear sturdy, comfortable shoes whenever feasible to protect your feet. To be sure your shoes fit properly, see a podiatrist (foot doctor) for fitting recommendations or shop at shoe stores specializing in fitting people with diabetes. Your endocrinologist (diabetes specialist) can provide you with a referral to a podiatrist or orthopedist who may also be an excellent resource for finding local shoe stores. If you have flat feet, bunions, or hammertoes, you may need prescription shoes or shoe inserts. Exercise Regular exercise will improve bone and joint health in your feet and legs, improve circulation to your legs, and will also help to stabilize your blood sugar levels. Consult your physician prior to beginning any exercise program. Smoking If you smoke any form of tobacco, quitting can be one of the best things you can do to prevent problems with your feet. Smoking accelerates damage to blood vessels, especially small blood vessels leading to poor circulation, which is a major risk factor for foot infections and ultimately amputations. Diabetes control Following a reasonable diet, taking your medications, checking your blood sugar regularly, exercising regularly, and maintaining good communication with your physician are essential in keeping your diabetes under control. Consistent long-term blood sugar control to near normal levels can greatly lower the risk of damage to your nerves, kidneys, eyes, and blood vessels. MANAGEMENT DURING SEIZURES AND EPILEPSY SUPPOSITORIES FOR HIGH FEVER Fever Is part of the body's normal defense mechanisms for killing bugs in the blood (viruses). When you get a fever, your body heats up to burn out the viruses that are making you feel unwell. While a fever may burn itself out over time, a prolonged high fever may cause brain damage. FeverAll Acetaminophen Suppositories Are the perfect solution when your child can't or won't take liquid medicine to get the fever down. You can use one suppository every four to six hours as needed to bring the fever down, but not to exceed six in 24 hour period. NOSEBLEEDING NOSEBLEEDING Is the relatively common occurrence of hemorrhage from the nose, usually noticed when the blood drains out through the nostrils. There are two types: 1. 2. Anterior (the most common) Posterior (less common, more likely to require medical attention). Can generally be divided into two categories: a. Local o Blunt trauma (usually a sharp blow to the face such as a punch, sometimes accompanying a nasal fracture) o Foreign bodies (such as fingers during nose-picking) o Inflammatory reaction (e.g. acute respiratory tract infections, chronic sinusitis, allergic rhinitis or environmental irritants) b. Systemic o Allergies o Infectious diseases (e.g. common cold) o Hypertension HOME CARE MANAGEMENT: If the nose starts bleeding after a trauma, seek medical help immediately, as it could indicate a skull fracture. When dealing with a common nose bleed not caused by trauma, stand with head tilted forward. Using the thumb and forefinger, grab the front of your nose, squeezing tightly and hold this pressure for five minutes. A cold compress on the bridge of the nose can also help. If you cannot stop the bleeding within 15 minutes, you need to seek medical care. PROFESSIONAL CARE: If trauma is suspected, your doctor will perform an X-ray to see if the skull has been damaged. If no trauma or damage is present, your physician will probably pack your nose with gauze. If this does not work, a catheter in the nose may be used to collect the blood and put pressure on the artery. If you suffer from chronic nose bleeds, your doctor may cure your condition by cauterizing the blood vessels in your nose. This involves heating them so that they are permanently sealed. FOLEY CATHETER Is a flexible tube that is passed through the urethra and into the bladder. Are commonly made from silicone rubber or natural rubber Size is described using French units The tube has two separated channels, or lumens, running down its length. a. One lumen is open at both ends, and allows urine to drain out into a collection bag. b. The other lumen has a valve on the outside end and connects to a balloon at the tip. INDICATIONS: On patients who are anesthesized or sedated for surgery or other medical care On comatose patients On some incontinent patients On patients with acute urinary retention. On patients who are unable due to paralysis or physical injury to use either standard toilet facilities or urinals. Following urethral surgeries Following ureterectomy Types: 1. "Three way" or "triple lumen" catheter - Which is used to infuse sterile saline or another irrigating solution. - These are used primarily after surgery on the bladder or prostate, to wash away blood and blood clots. 2. Indwelling catheter - A urethral catheter designed to be held in place to drain urine from the bladder. 3. Straight catheter - Is a straight tube of pliable plastic or rubber. - One end is rounded to prevent any trauma to tissue, with the opening of the lumen (the opening) down the center of the tube) on the side. - The other end of a catheter is enlarged to form a connection to some type drainage or collection system, and more importantly prevent theV catheter from being completely "lost" into the urethra. REMOVAL OF URINARY CATHETER 1. Gather equipment. 2. Explain procedure to the patient 3. Assist patient into supine position with legs spread and feet together 4. Apply sterile drape 5. Locate the inflation port on the catheter's side and attach a small syringe. Draw out the fluid using your syringe until no more fluid can be drawn. 7. Remove the catheter slowly by gently pulling it out completely Cut the balloon port tubing, using surgical scissors, as a second alternative to remove your catheter. Wait for all the fluid to drain before slowly pulling out the catheter. 8. Evaluate catheter function and amount, color, odor, and quality of urine 9. Remove gloves, dispose of equipment appropriately, wash hands. 10. Document all pertinent information. 6. SUCTIONING Used to clear the airway of excessive secretions when the patient is unable to clear the respiratory tract with coughing. Nasotracheal Suctioning Remove secretions from the pharynx by means of a suction catheter to maintain a patent airway To promote pulmonary gas exchange Help prevent infections caused by accumulated secretions. Oropharyngeal Suctioning Is usually performed using a rigid plastic catheter with one large and several small eyelets that mucous enters when suction is applied. This type of catheter is called a Yankauer or tonsil suctioning device. Alert patients can be taught to use this device to control excess secretions in the mouth. TRACHEOSTOMY TUBE SUCTIONING General Considerations: 1. Never ever remove outer cannula. It is changed only by the doctor. If accidentally expelled, keep airway open with a hemostat. 2. Always keep an extra, complete tracheostomy tube set at the bedside, and a forcep or tracheal dilator or obturator. 3. If patient shows signs of cyanosis, difficult breathing, or the tube become dislocated, call the doctor at once. 4. Do not use any cotton or cotton applicator around a tracheostomy. ENDOTRACHEAL SUCTIONING A deep suctioning by the use of catheter which is inserted farther into the trachea and or trachea; Usually, 20cm or 8 in. of the catheter is inserted in an adult. PURPOSES: 1. 2. Maintain patent airway by stimulating cough reflex To aspirate mucus and other secretions farther down into the trachea NOTE: Never apply suction during insertion. Application of suction pressure while introducing the catheter into the trachea increases risk of damage to the mucosa and increases the risk of hypoxia because the removal of oxygen present in the airway. Remember that the epiglottis is open during inspiration and facilitates insertion of the catheter into the trachea. Elevated pressure settings increase risk of trauma to mucosa SKELETAL TRACTION Traction Is the act of pulling or drawing which is associated with countertraction. PURPOSES: To lessen muscle spasm b. To reduce fracture c. To provide immobilization d. To maintain body alignment a. SKELETAL TRACTION Traction applied directly upon long bones by means of pins and wires. Examples: 1. 2. 3. 4. 5. 6. Halo- Pelvic – for scoliosis Halo- Femoral – severe scoliosis 90 – 90- subtrochanteric fracture of femur BST – femur and hips Overhead – humerus Halo Traction – cervical spine HALO PELVIC HALO-FEMORAL 90-90 SUBTROCHANTERIC OVERHEAD BALANCE SKELETAL TRACTION (BST) HALO TRACTION THANK YOU!!!